
Abstract
Background:
Major differences with respect to the diagnostic performance of a “ruling in” approach in the presurgical diagnosis of indeterminate thyroid fine-needle aspirations (FNAs) have been reported. Therefore, the aim of this prospective multicenter study was to investigate the specific diagnostic impact of mutation testing using a seven-gene panel in a routine primary referral setting analyzing FNAs from endocrinology and nuclear medicine practices in Germany.
Methods:
RNA and DNA was extracted from 564 routine air-dried FNA smears obtained from 64 physicians and cytologically graded by one experienced cytopathologist. PAX8/PPARG and RET/PTC rearrangements were detected by quantitative polymerase chain reaction, while BRAF and RAS mutations were detected by pyrosequencing. Molecular data were compared to histology and follow-up >1 year, which were available for 322/348 patients undergoing surgery and 33/74 patients having follow-up. Histology results were obtained from the local routine pathologists who were blinded to the molecular test results.
Results:
BRAF and RET/PTC mutations were associated with carcinoma in 98% and 100% of samples, respectively. RAS and PAX8/PPARG mutations were associated with carcinoma in 31% and 0% of samples, respectively. Thirty-six percent of the carcinomas were identified by molecular testing in the atypia of undetermined significance/follicular lesion of undetermined significance and follicular neoplasm/suspicious for a follicular neoplasm categories, with malignancy rates of 15% and 17%, respectively. Due to a low percentage of RAS mutation-positive carcinomas in combination with a rather high percentage of RAS mutation-positive benign nodules, the positive predictive values of 41% and 36% in the atypia of undetermined significance/follicular lesion of undetermined significance and follicular neoplasm/suspicious for a follicular neoplasm categories offer only limited diagnostic potential.
Conclusion:
In conclusion, the data suggest that the application of the current seven-gene panel in a routine primary referral setting does not improve the presurgical diagnosis of thyroid FNAs. While the diagnostic relevance of RAS mutations in thyroid tumors needs further investigation, more comprehensive mutation panels with more cancer-specific mutations may improve the presurgical diagnosis of thyroid FNAs.
Introduction
O
In their 2011 single-center study, Nikiforov et al. (4) analyzed a seven-gene panel for point mutations and gene fusions in 967 indeterminate FNAs, 513 (53%) with a histological diagnosis. Since they obtained sensitivities of 63% and 57% concomitant with high positive predictive values (PPV) of 88% and 87% in the subcategories of atypia of undetermined significance/follicular lesion of undetermined significance (AUS/FLUS) and follicular neoplasms/suspicious for a follicular neoplasms (FN/SFN), respectively, they suggested a positive genetic test should be considered an indication for total thyroidectomy (4). Beaudenon-Huibregtse et al. (5) analyzed 97 indeterminate FNAs with a seven-gene panel in a prospective multicenter study (53 [55%] with a histological diagnosis). They obtained, in comparison to the study by Nikiforov et al. (4), a rather low sensitivity of 36% concomitant with a PPV of 67% in the AUS/FLUS category (1). Finally, Labourier et al. (6) analyzed 282 indeterminate FNAs (AUS/FLUS + FN/SFN) using a combination of a seven-gene mutation panel and a miRNA classifier in a prospective multicenter study, 109 (39%) with a histological diagnosis. Focusing on the results of the mutation panel, they reported a sensitivity of 69% and a PPV of 71% for their indeterminate FNAs (1). Varying sensitivities and PPVs can be explained by high intra- and inter-observer variabilities in the cytological and histological evaluation of thyroid nodules (7 –9), a different prevalence of mutations in different populations, and different local malignancy rates in identical cytological categories largely dependent on the referral situation evaluated (10). Moreover, contrary to the present study, for both of the latter studies, the pathologists were not blinded to the molecular test results. Due to the important diagnostic variability introduced by these factors, it is mandatory to evaluate the diagnostic performance of FNA cytology and molecular FNA diagnostics for each specific local setting.
In contrast to the studies using additional or residual fresh FNA material, a method was established to use routine air-dried FNA smears for molecular testing (11,12), which offers major advantages (13). In two subsequent retrospective studies (14,15), a comparable methodological performance to assays that use fresh FNA material was demonstrated. However, these two retrospective studies—one with samples from Denmark (14) and one with samples from Italy (15)—revealed strong differences with regard to the diagnostic potential within the indeterminate categories. While the analysis of the 163 Italian indeterminate FNAs revealed a sensitivity of 49% and a PPV of 71% (15), the molecular testing of the 141 Danish indeterminate FNAs performed rather poor with a very low sensitivity of 18% and a PPV of 19% (14), highlighting even more the need to evaluate a diagnostic test in its specific, local field of application. Based on these strongly varying data in the retrospective studies, the diagnostic performance of the methodology was evaluated under real routine diagnostic conditions in a primary referral setting in Germany. The methodology was introduced into a routine diagnostic laboratory in Germany in 2012 (16), which performed the molecular analysis of indeterminate specimens of a single cytopathologist who received FNA specimens from 38 physicians performing FNAs throughout Germany in a primary referral setting. During a two-year period, 9460 FNAs were cytologically graded according to the Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) guideline (17), of which 606 were prospectively tested for mutations. The results of this two-year routine application of the seven-gene panel in a primary referral setting are now presented.
Materials and Methods
Patients and samples
Within a time frame of two years (June 2012–June 2014), 9460 thyroid FNAs were cytologically graded by an experienced thyroid cytopathologist (I.R.) according to the TBSRTC guideline (17). At variance with other data mostly originating from tertiary centers, these data demonstrate low percentages for malignant (MAL), suspicious for malignancy (SFM), FN/SFN, and AUS/FLUS cases, and high percentages for cysts/cystic nodules in this primary care setting in Germany. Of the 9460 FNAs, mostly performed with ultrasound (US) guidance by 64 different physicians, 564 were selected for molecular diagnostics according to the following criteria: FNAs with a AUS/FLUS cytology if additional signs of follicular proliferation, including suspicion for a follicular variant of papillary thyroid carcinoma (fvPTC), were present or if the AUS/FLUS diagnosis was based on a low number of cells, unless molecular diagnostics was not ordered by the referring physician (n = 195); most cytologies with the diagnosis FN/SFN, unless molecular diagnostics was not ordered by the referring physician (n = 278); cytologies with the diagnosis SFM if ordered by the referring physician (n = 55); and cytologies with a MAL diagnosis if ordered by the referring physician, except for those with cytological evidence for anaplastic thyroid carcinoma or a primary tumor outside the thyroid (n = 36). Current guidelines do not recommend molecular diagnosis for SFM and MAL cytologies. For the 564 patients, the standardized collection and analysis of the following data was performed: thyrotropin (TSH), thyroid autoantibody values, calcitonin, thyroid ultrasound, nodule size, sonographic malignancy criteria, Tc scintiscan results, recommendation for surgery by the treating physician, surgery report, histology and/or follow-up ultrasound. The median age of the 564 patients was 55 years (range 13–88 years), and the median size of the nodules was 2.4 cm (range 0.6–13 cm). No histologic or follow-up data could be obtained for 142/564 patients (Fig. 1). While 348/564 patients with molecular diagnostics underwent thyroid surgery, 74 patients had follow-up. For 322/348 patients with thyroid surgery, histology results could be obtained from the local routine pathologists who were blinded to the molecular test results. For 33/74 patients who had follow-up, follow-up data of at least one year could be obtained revealing no evidence of malignancy.
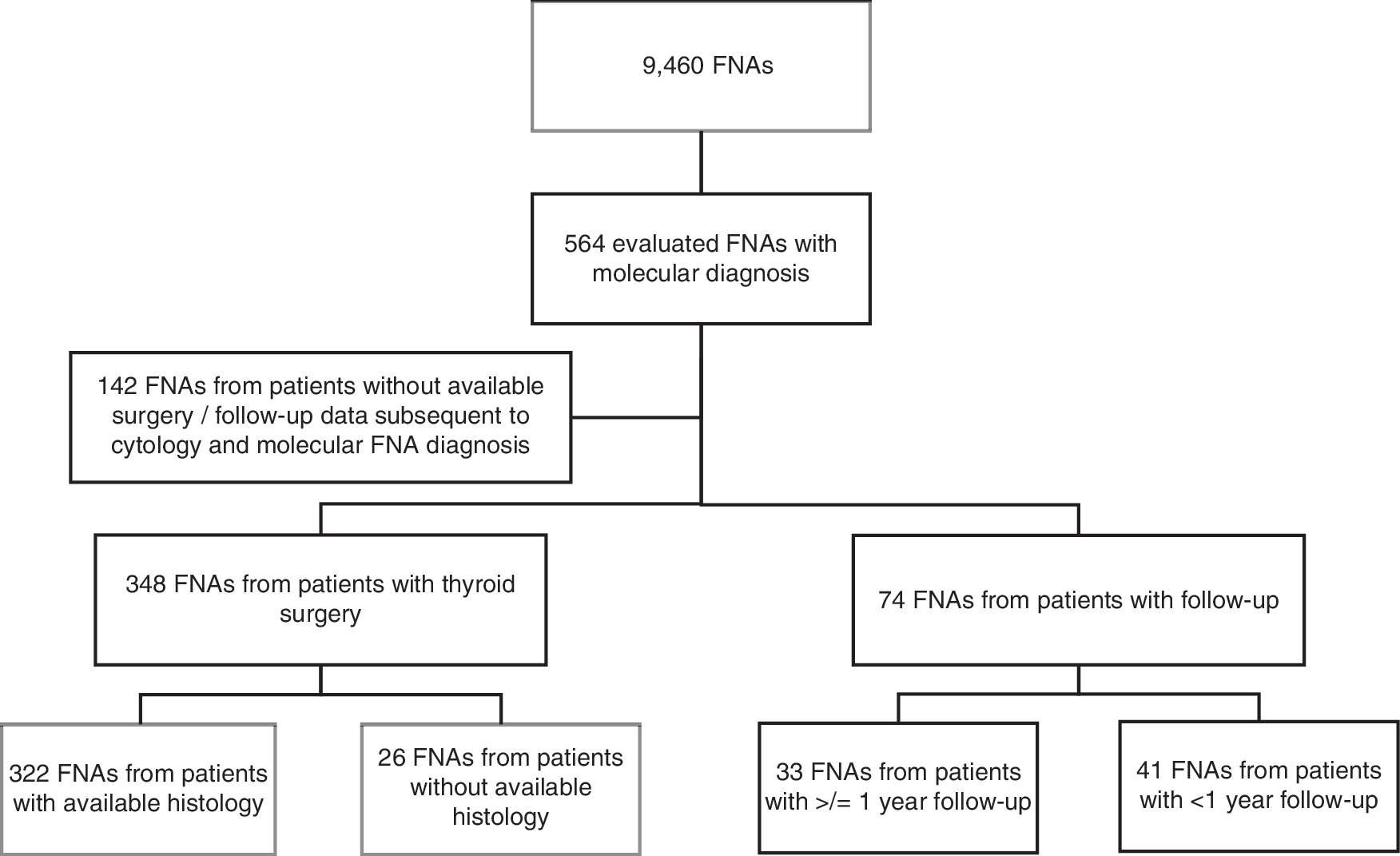
Composition of the set of thyroid nodules receiving presurgical molecular fine-needle aspiration (FNA) diagnosis with regard to thyroid surgery, follow-up, and available histology and follow-up data, respectively.
Because mutation testing on FNA samples is the standard of care in the routine diagnostic setting, the molecular analysis did not require approval of the ethics committee of the University of Leipzig. The retrospective analysis of cytological, histological, clinical, and molecular data was approved by the ethics committee of the University of Leipzig.
DNA and RNA extraction from FNA smears
DNA and RNA were extracted from the routine air-dried FNA smears using the AllPrep FFPE Kit (Qiagen, Hilden, Germany) according to the manufacturer's protocol. In brief, the FNA smears were incubated in xylene for four to five days to remove the cover slips. Thereafter, 150 μL of PKD buffer was added to the slide, and the cells on the slide were detached within the PKD buffer using a cell scraper. The detached cells were transferred to a new tube, and DNA and RNA were extracted according to the manufacturer's protocol.
cDNA synthesis
cDNA was synthesized using the miScript Reverse Transcription Kit (Qiagen) according to the manufacturer's protocol. In brief, 7.5 μL of template RNA was added to a master mix consisting of 2 μL of 5 × miScript RT buffer and 0.5 μL of miScript Reverse Transcriptase Mix and incubated for 60 min at 37°C. Subsequently, the miScript Reverse Transcriptase Mix was inactivated for 5 min at 95°C.
Detection of rearrangements by quantitative polymerase chain reaction
PAX8/PPARG, RET/PTC1, and RET/PTC3 rearrangements were detected in multiplex-quantitative polymerase chain reactions (PCR) on a LightCycler 480 (Roche, Mannheim, Germany) using the QuantiTect SYBR Green PCR kit (Qiagen), with one primer pair amplifying an intron spanning 125 bp control fragment of PAX8 mRNA (exon 5–6; for cDNA quality control), and one rearrangement specific primer pair, as described previously (14,15). Following the PCR, a fluorescence melting curve analysis was performed to detect and discriminate the control fragment and the rearrangement specific amplicons by their specific melting points (14).
Detection of point mutations by pyrosequencing
BRAF (codons 600/601), KRAS (codons 12/13), HRAS (codon 61), and NRAS (codon 61) point mutations were detected by pyrosequencing. In brief, 3 μL of genomic DNA was amplified using self-designed template specific PCR primers (Supplementary Table S1; Supplementary Data are available online at
Histologic re-evaluation of mutation-positive histological benign samples
Mutation-positive nodules, which were surgically removed and were histologically diagnosed as adenomatous nodule (AN), follicular adenoma (FA), or oncocytic subtype of FA (oFA) by the local pathologists, were, in case of available blocks, re-reviewed according to the World Health Organization criteria (18) and Piana et al. (19) by an expert referral pathologist (U.S.), who was aware of the molecular testing results. Statistical analysis was based on these revised histological diagnoses. While one follicular thyroid carcinoma (FTC) case was considered as malignant, follicular tumors of uncertain malignant potential (FT-UMP) were considered as benign. The histologic re-evaluation did not significantly influence the statistical outcome of the data (p = 1).
Statistics
Sensitivities, specificities, PPV, and negative predictive values (NPV) were calculated as follows:
The prevalence of malignancy based PPV and NPV were calculated as follows:
In the comparisons of cytology versus histology, and molecular FNA analysis (mFNA) versus histology, histology is the gold standard. In the comparison mFNA versus histology, a mutation-negative, histologically benign sample is considered as “true negative”; a mutation-positive, histologically malignant sample is considered “true positive”; a mutation-positive, histologically benign sample is considered as “false positive”; and a mutation-negative, histologically malignant sample is considered “false negative.”
Results
Inadequate PCR product
In total, molecular testing revealed inadequate results in 30/355 analyzed FNAs (8%). While in 31 FNAs the RNA-based detection of one or more rearrangements failed, the DNA-based detection of point mutations failed in only two FNAs. In one sample, both RNA and DNA were insufficient for molecular testing. Of the 355 FNAs with available histology or follow-up of at least one year, 30 were classified “not evaluable” (NE), since they were characterized by at least one inadequate PCR and a mutation-negative test outcome in all the other tests (Table 1). The percentage of NE-FNAs was highest in the AUS/FLUS-FNAs (15.2% NEs), followed by 7.1%, 6.6%, and 3% NE-FNAs in the SFM-FNAs, FN/SFN-FNAs, and MAL-FNAs, respectively. FNAs classified as NE were not considered in the calculation of sensitivity and specificity.
For the reclassified FT-UMP cases, the original routine diagnosis was used for this table. For comparison, see Table 4.
One BRAF mutation was detected in a FNA with a cytological diagnosis of suspicion of malignancy. Since the histology block of this tumor could not be obtained, the histological diagnosis of an oncocytic subtype of a follicular adenoma could not be validated.
AN, adenomatous nodule; AUS/FLUS, atypia of undetermined significance/follicular lesion of undetermined significance; cPTC, classical papillary thyroid carcinoma; FA, follicular adenoma; FNA, fine-needle aspiration; FN/SFN, follicular neoplasms/suspicious for a follicular neoplasms; FTC, follicular thyroid carcinoma; fvPTC, follicular variant papillary thyroid carcinoma; MAL, malignant; NE, not evaluable due to failed PCR; oFA, follicular adenoma, oncocytic subtype; oFTC, follicular thyroid carcinoma, oncocytic subtype; PCR, polymerase chain reaction; SFM, suspicious for malignancy.
Performance of cytology in comparison to histology
Cytological evaluation of the 355 FNAs with histology or follow-up of at least one year revealed 81 AUS/FLUS, 199 FN/SFN, 42 SFM, and 33 malignant results (Table 1). All 33 cytologically malignant samples were carcinomas at histology (30 classic papillary thyroid carcinomas (cPTCs), three fvPTC). The final histological classification of the 42 SFM-FNAs revealed 26 cPTCs, eight fvPTCs, one oncocytic subtype of FTC (oFTC), one FTC, two oFA, three FA, and one thyroiditis. The final histological classification of the 199 FN/SFN-FNAs revealed eight cPTCs, 12 fvPTCs, eight FTCs, six oFTCs, 68 FAs, 36 oFAs, 40 ANs, three thyroiditis, and 18 samples without surgery but follow-up of at least a year. The final histological classification of the 81 AUS/FLUS-FNAs revealed four cPTCs, four fvPTCs, three FTCs, one oFTC, 31 FAs, two oFAs, 20 ANs, one thyroiditis, and 15 samples without surgery but follow-up of at least a year. As shown in Table 2, these data result in a cytology-based risk of malignancy (ROM) of 15%, 17%, 86%, and 100% for the AUS/FLUS, FN/SFN, SFM, and malignant categories, respectively.
ROM, risk of malignancy.
Overall performance of molecular FNA testing in comparison to histology
Molecular FNA (mFNA) revealed 85 mutations in total (Table 1). Forty-four BRAF mutations were detected in 36 cPTCs, seven fvPTCs, and one oFA. Unfortunately, although the detection of a BRAF mutation and the cytological diagnosis of SFM question the histological diagnosis of an oFA, the histological diagnosis could not be validated, since the histology block of this tumor could not be obtained because the patient did not consent. Furthermore, 22 NRAS mutations were detected in the FNAs, representing two cPTC, six fvPTCs, one FTC, seven FAs, two oFAs, one AN, one thyroiditis at final histology, and two FNAs with follow-up of at least a year. In addition, nine HRAS mutations could be detected in the FNAs (one fvPTC, five FAs, one oFA, and two ANs). One KRAS mutation was detected in an FNA representing an oFA at histology. Furthermore, the following rearrangements were detected: three PAX8/PPARG rearrangements in three FAs, four RET/PTC1 rearrangements in three cPTCs and one fvPTC, and two RET/PTC3 rearrangements in two cPTCs. A total of 240 FNAs were mutation negative, representing 21 PTCs, 10 fvPTCs, 11 FTCs, six oFTCs, 81 FAs, 33 oFAs, 47 ANs, four thyroiditis, and 27 FNAs with follow-up of at least a year. Overall, these data result in a sensitivity of 55%, a specificity of 88%, and a PPV and NPV of 69% and 80%, respectively, for mFNA (Table 3).
PPV, positive predictive value; NPV, negative predictive value.
Performance of mFNA in the AUS/FLUS and FN/SFN group in comparison to histology
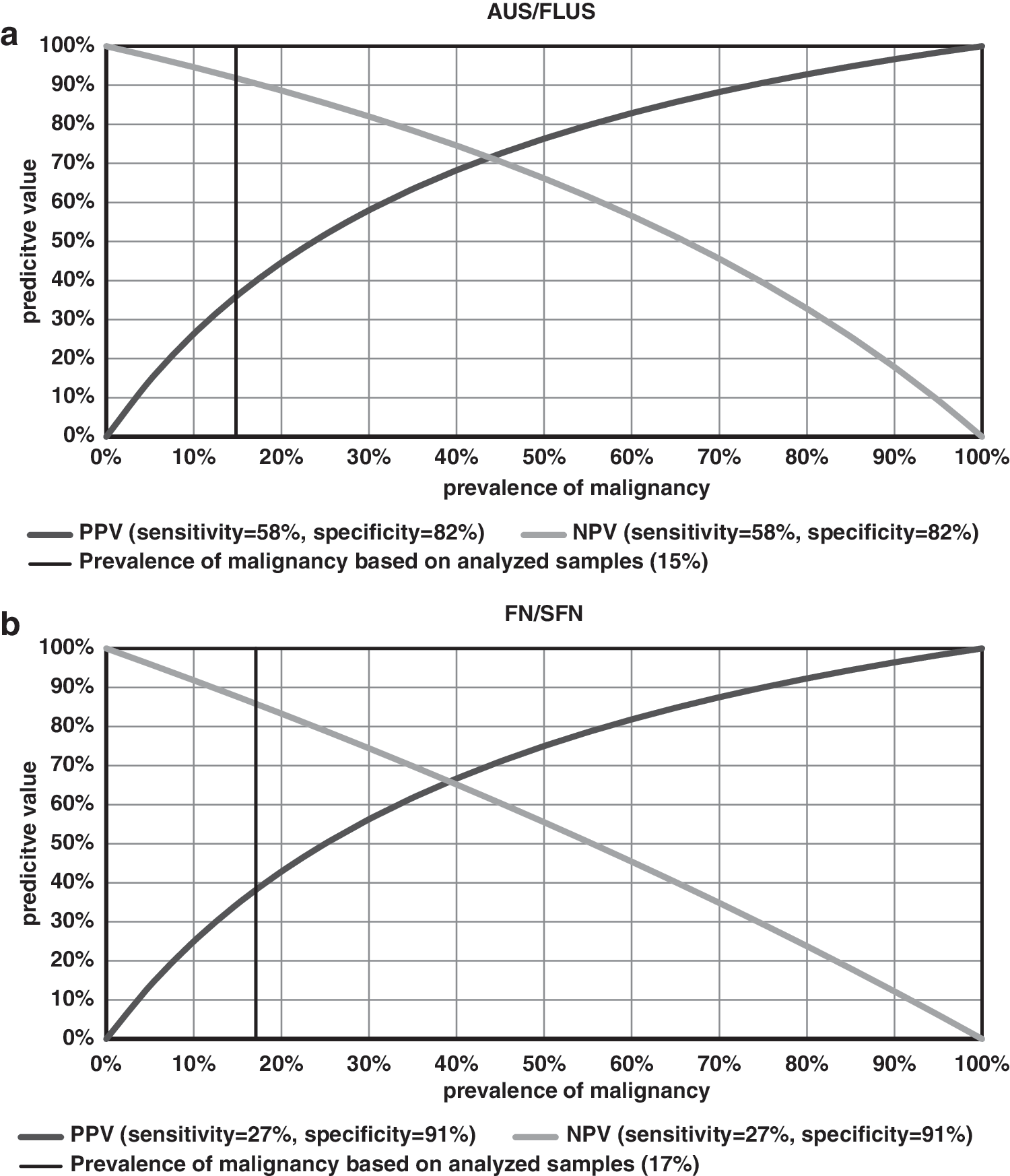
mFNA detected 17 mutations (two BRAF, seven NRAS, four HRAS, three PAX8/PPARG, and one RET/PTC3) in the 81 AUS/FLUS samples with histology or follow-up of at least a year, representing three cPTCs, four fvPTCs, six FAs, one oFA, two ANs, and one nodule with follow-up of at least a year (Table 1). Fifty-one AUS/FLUS FNAs were mutation negative, representing one cPTC, three FTCs, one oFTC, 21 FAs, 13 ANs, one thyroiditis, and 11 nodules with follow-up of at least a year. Based on these data, mFNA allowed the detection of 7/12 carcinomas in the AUS/FLUS category, while 10/56 benign samples revealed a false-positive test outcome, resulting in a sensitivity of 58%, a specificity of 82%, and a PPV and NPV of 41% and 90%, respectively (Table 3).
In the 199 FN/SFN samples, mFNA detected 22 mutations (two BRAF, 13 NRAS, five HRAS, one KRAS, and one RET/PTC3), with histology or follow-up of at least a year, representing four cPTCs, three fvPTCs, one FTC, nine FAs, three oFAs, one AN, and one nodule with follow-up of at least a year (Table 1). A total of 164 FN/SFN FNAs were mutation negative, representing two cPTC, eight fvPTC, seven FTCs, five oFTCs, 57 FAs, 32 oFAs, 34 ANs, three thyroiditis, and 16 nodules with follow-up of at least a year. Based on these data, mFNA allowed the detection of 8/30 carcinomas in the FN/SFN category, while 14/156 benign samples revealed a false-positive test outcome, resulting in a sensitivity of 27%, a specificity of 91%, and a PPV and NPV of 36% and 87%, respectively (Table 3).
Histologic re-evaluation of mutation-positive histological benign samples
For 16 mutation-positive histologically benign samples, histology blocks could be obtained for a histologic re-evaluation by a second pathologist who was aware of the mutation testing results. The re-evaluation was based on the criteria described by Piana et al. (19), and resulted in the reclassification of one FA into FTC, while five nodules where re-classified as FT-UMP (Table 4).
Mutation-positive nodules that underwent surgery and were histologically diagnosed as AN/FA/oFA were, in case of available blocks, re-reviewed according to the World Health Organization criteria (18) and Piana et al. (19) by an expert pathologist (U.S.) who was aware of the molecular testing results.
AN, adenomatous nodule; FA, follicular adenoma; FTC, follicular thyroid carcinoma; FT-UMP, follicular tumor of uncertain malignant potential.
Discussion
After setting up a methodology of mutation testing that is based on routine air-dried FNA smears (11,12) and evaluating this method in two retrospective studies (14,15), here the results of a two-year prospective application in a routine diagnostic laboratory in Germany are presented. Within the two years, 9460 FNAs were graded by a single cytopathologist who received FNA specimens from 38 physicians performing FNAs in a primary referral setting. With molecular results for 564 FNAs and an available histology or follow-up of at least a year for 355 nodules (Fig. 1), this study is the second largest prospective study for the seven-gene panel after the study by Nikiforov et al. (4). Regarding histology/follow-up data for 63% of the analyzed FNAs, this study is again comparable to Nikiforov et al. (4), with histology/follow-up data for 67% of analyzed FNAs, whereas in the studies by Beaudenon-Huibregtse et al. (5) and Labourier et al. (6), these data were available for only 15% and 39%, respectively.
While the sensitivity for mFNA of 58% in the AUS/FLUS category (Table 3) is comparable to a sensitivity of 63% in (4), the specificity of 82% is lower compared to a specificity of 99% in Nikiforov et al. (4) but identical with the specificity described by Beaudenon-Huibregtse et al. (5). Interestingly, the sensitivity of 27% in the FN/SFN category is lower than in the studies of Nikiforov et al. (4) and Beaudenon-Huibregtse et al. (5), while the specificity of 91% is similar to the 92% determined by Beaudenon-Huibregtse et al. (5). A comparison to the authors' two previous retrospective studies is rather difficult, since in these studies, the cytological grading of the FNAs was done according to the 2006 American Thyroid Association (ATA) guidelines (20) with only one indeterminate category, and according to the Italian Society for Anatomic Pathology and Cytopathology (SIAPEC)-International Academy of Pathology five-tier reporting system (21,22), which is superimposable to the 2007 BTA guidelines (23) with two indeterminate categories, respectively. Nevertheless, the low sensitivity of 27% in the FN/SFN category compares well to a low sensitivity of 18% in the first retrospective study (14).
This low sensitivity in the FN/SFN category is mainly due to two findings. First, a very low mutation prevalence in FTCs (9%): only one NRAS mutation could be detected in 11 FTCs (Table 1). Second, while the prevalence of fvPTCs in the AUS/FLUS (6%) and FN/SFN (5%) categories is nearly identical, an exceptional low mutation frequency in the fvPTCs was observed in the FN/SFN category (27%). This mutation frequency is significantly lower than the mutation frequency observed in the fvPTCs in the AUS/FLUS category (100%; p < 0.05), and is lower than the mutation frequency of the fvPTCs in the SFM (71%) and MAL (100%) category. For no other cancer entity were such differences observed between the cytological categories. While the specificities of 82% in the AUS/FLUS and 91% in the FN/SFN category (Table 3) are comparable to the specificities observed by Beaudenon-Huibregtse et al. (5), Labourier et al. (6), and in the previous retrospective studies (14,15), they are lower in comparison to Nikiforov et al. (4) who observed specificities of 99% and 97%, respectively. As in the previous studies (14,15), this lower specificity is due to RAS/PAX8/PPARG mutations in histologically benign nodules (Table 1). Especially, the prevalence rates of 22% and 14% RAS/PAX8/PPARG mutations in FAs in the AUS/FLUS and FN/SFN categories is higher than the prevalence of these mutations in FTCs (9%), resulting in lower specificities and also lower PPVs. In detail, the PPV of RAS mutations over all cytological categories is rather low. While in the authors' setting NRAS mutations have the highest PPV of 41% (AUS/FLUS: 57%, FN/SFN: 31%), HRAS and KRAS mutations have an overall PPV of 11% (AUS/FLUS: 0%, FN/SFN: 20%) and 0% (FN/SFN: 0%), respectively (Tables 1 and 2). Only BRAF and RET/PTC mutations are highly specific for thyroid cancer, resulting in PPVs of 98% and 100%, respectively.
Based on a recent study (15) in which the histological re-evaluation of nodules initially diagnosed as FAs resulted in a re-classification of 3/10 RAS-positive tumors as minimally invasive FTCs, the mutation-positive histologically benign nodules of this study also underwent a histological re-evaluation by an expert referral pathologist (in case the histology block could be obtained; Table 4). This re-evaluation was performed considering criteria such as vascular invasion, capsular invasion, and PTC-type nuclei according to Piana et al. (19), and resulted in the re-classification of 1/16 benign nodules as FTC, while five FAs/ANs were classified as FT-UMP due to capsular invasion but no capsule breakthrough. With regard to the recently updated ATA guidelines (24), which recommend a less aggressive treatment of thyroid cancer than before, especially the classification of five nodules as FT-UMP most likely will not significantly change the clinical management of these patients. However, the one reclassified FTC highlights once more the dilemma of high intra- and inter-observer variabilities, not only in the cytological but also in the histological evaluation of thyroid nodules, and thus the difficulty of establishing histology as the gold standard (7 –9).
So what is the final impact of molecular FNA testing on the clinical management of patients based on this study? First, for the ROM based on cytology alone, a 15% ROM was observed in the AUS/FLUS category, which is at the upper end with regard to the TBSRTC recommendation for the AUS/FLUS category (5–15%) (17) but comparable to both studies of the Nikiforov group (4,25), whereas the study of Beaudenon-Huibregtse et al. (5) is characterized by a very high (50%) ROM in the AUS/FLUS category. In contrast to the AUS/FLUS category, the ROM observed in the FN/SFN category (17%) is closer to the lower end with regard to the TBSRTC recommendation for this category (15–30%) (17) and is also considerably lower in comparison with the studies of Nikiforov et al. (4) and Beaudenon-Huibregtse et al. (5), with a 27% and a 32% ROM, respectively. This lower ROM is most likely due to the fact that in the primary referral setting, 38 general endocrinology and nuclear medicine practices submitted a mean number of only 15 FNAs for molecular testing in two years, whereas in the study of Beaudenon-Huibregtse et al. (5), 806 FNAs were obtained from five clinical sites in a period of 2.3 years, and in the setting of Nikiforov et al. (4), the FNAs were obtained in a tertiary referral center with a higher probability of malignant nodules (10). Since the PPV of a test increases with an increasing prevalence of malignancy (i.e., pretest ROM; Fig. 2), this low prevalence of malignant tumors in the cytological indeterminate categories, especially in the FN/SFN category, results vice versa in low PPVs of 41% and 36% in the AUS/FLUS and FN/SFN categories, respectively (Table 3).
(
In conclusion, the current data suggest that overall the application of the current seven-gene panel as a “rule-in” test in a routine setting analyzing FNAs in a primary referral setting from endocrinology and nuclear medicine practices in Germany does not improve the presurgical diagnosis of thyroid FNAs. The low diagnostic impact is mainly due to a low prevalence of RAS mutations in thyroid carcinomas (resulting in a low sensitivity), a rather high prevalence of RAS mutations in HNs/FAs (resulting in a rather low specificity, even after a second histopathology review), and finally a low prevalence of malignancy in the indeterminate FNA samples in this primary referral setting, resulting in low PPVs. While the diagnostic relevance of RAS mutations in thyroid tumors needs further investigation, more comprehensive mutation panels with more cancer-specific mutations may improve the presurgical diagnosis of thyroid FNAs.
Footnotes
Acknowledgments
We would like to thank Praxen für Diagnostische und Therapeutische Nuklearmedizin, Berlin, Germany; Dr. Seidel, Schilddrüsenpraxis Kantstraße, Berlin, Germany; Dr. Grußendorf, MVZ Rothebühlplatz der Medivision, Stuttgart, Germany; Dr. Rehder, Radiologische Gemeinschaftspraxis, Buchholz, Germany; Prof. Dr. Reinhardt, Oldenburg, Germany; Dr. Yousef, MVZ Nuklearmedizin, Bremerhaven, Germany; Radiologiezentrum Nordharz, Wolfenbüttel, Germany; Röntgenpraxis im Tesdopfhaus, Lübeck, Germany; Dr. Troglauer, Gemeinschaftspraxis für Radiologie und Nuklearmedizin Wiesbaden, Germany; Dr. Wilbert, Radiologisches Institut, Koblenz, Germany; Dr. Körber, Diagnostikum Nuklearmedizin, Fulda, Germany; Radiologische Gemeinschaftspraxis Fischer & Fischer, Trier, Germany; MVZ Endokrinologikum Frankfurt/Main, Germany; Dr. de la Roche, MVZ am Klinikum, Oldenburg, Germany; MVZ Endokrinologikum, Osnabrück, Germany; PD Dr. Dobschütz, Krankenhaus Reinbeck St. Adolf-Stift, Reinbeck, Germany; Dr. Pinick, Internistische Gemeinschaftspraxis, Buchholz, Germany; MVZ Endokrinologikum, Berlin, Germany; and Dr. Strache, Radiologische Gemeinschaftspraxis, Buxtehude, Germany, for participating in this study by submitting FNAs for molecular diagnostics and by comprehensively supporting the analysis of the data. Markus Eszlinger is supported by a Deutsche Krebshilfe grant (109994) and a Wilhelm-Sander-Stiftung grant (2013.010.1). Ralf Paschke is supported by the DFG, a Deutsche Krebshilfe grant, and a Wilhelm-Sander-Stiftung grant (2013.010.1).
Author Disclosure Statement
All authors have nothing to declare. No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.