
Abstract
Background:
The reported malignancy rates of thyroid nodules that appear suspicious on ultrasound (US) but yield benign fine-needle aspiration (FNA) cytology results range from 13.6% to 56.6%. However, the malignancy risk of nodules that are discordant on US and core-needle biopsy (CNB) pathological findings has not been evaluated. This study evaluated the malignancy risk associated with thyroid nodules that are suspicious on US but yield benign CNB results.
Methods:
Between July 2008 and November 2011, 1309 patients with 1313 thyroid nodules underwent US-guided CNB. Among these, 166 thyroid nodules that were suspicious on US but yielded benign CNB results were retrospectively reviewed. Benign nodules were diagnosed by surgery, FNA, and/or CNB that was repeated at least twice or CNB and lesion size stability on follow-up. The malignancy risk of US-pathology discordant nodules was calculated according to recommendations by Moon et al., and a further evaluation was conducted using four different US risk systems. Factors that differentiated benign from malignant nodules were assessed using the chi-square test or Fisher's exact test. Moreover, the histological findings of US-pathology discordant nodules were analyzed.
Results:
Patients with benign and malignant nodules did not differ significantly regarding clinical and demographic characteristics. Of the 166 US-pathology discordant nodules, seven (4.2%) were confirmed malignant. The malignancy risks associated with the five US risk systems ranged from 3.6% to 5.5%. Regarding suspicious US features, only the number of suspicious features was associated with malignancy (p = 0.002). Histological analysis of benign CNB specimens with suspicious US features revealed fibrosis (77.6%), thyroiditis (28.7%), calcifications (10.6%), and hemosiderin deposition (6.4%).
Conclusions:
The malignancy risk among thyroid nodules with discordant US and CNB results ranged from 3.6% to 5.5%, depending on US risk systems. However, repeated biopsy may be necessary for selected thyroid nodules with more than two suspicious US features.
Introduction
U
Recently, core-needle biopsy (CNB) has been proposed as an additional diagnostic method to supplement FNA of the thyroid (10 –12). CNB yields larger tissue samples and may provide additional information and more precise histological diagnoses (10,13,14). The post-CNB follow-up strategy is determined by risk stratification based on US features. However, the malignancy risks associated with US-CNB pathology discordant nodules have not been evaluated, and no consensus has been reached regarding further management. Accordingly, many thyroidologists find it difficult to manage patients with such lesions. Therefore, this study aimed to evaluate the malignancy risks associated with US-CNB pathology discordant thyroid nodules using various malignant stratification systems and to suggest management strategies for such cases.
Materials and Methods
Patient selection
This retrospective study was approved by the Institutional Review Board. Written informed consent was obtained from all patients prior to FNA or CNB.
The medical records and US images were reviewed of patients who underwent US-guided CNB for thyroid nodules at the authors' institution between October 2008 and November 2011. During this period, 1309 patients underwent US-guided CNB of 1313 thyroid nodules. The CNB pathology results are described in Figure 1. Among the 719 nodules with a benign CNB findings, 210 nodules with suspicious US features (US-pathology discordance) were selected, according to the recommendations made by the Korean Society of Thyroid Radiology and Moon et al. (15,16).
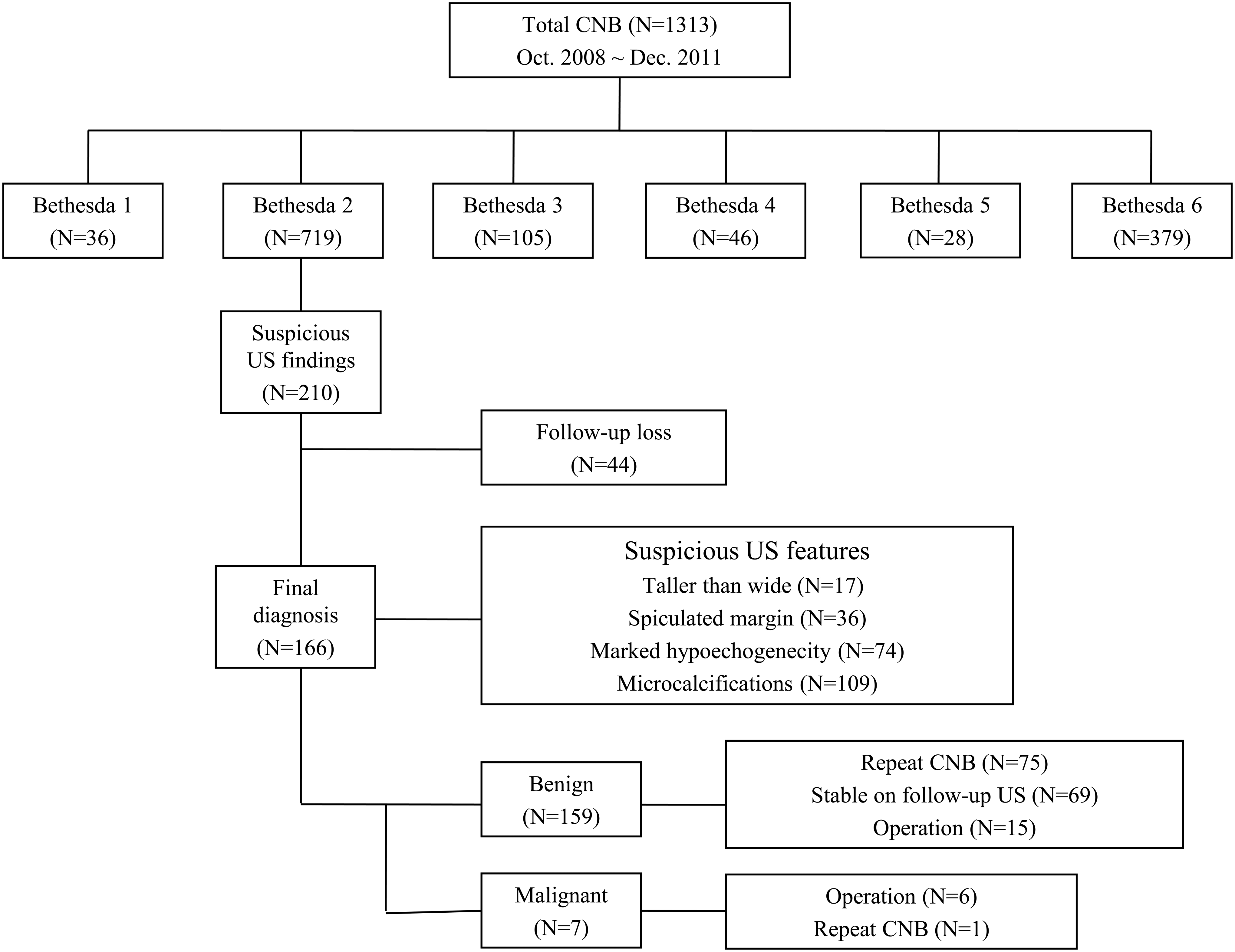
Flow chart of patients undergoing core-needle biopsy for thyroid nodules.
US-guided CNB procedures
US examinations were performed using either an iU22 unit (Philips Healthcare, Bothell, WA) or EUB-7500 unit (Hitachi Medical Systems, Tokyo, Japan) equipped with a linear high-frequency probe (5–14 MHz). All US examinations and US-guided CNBs were performed by radiologists under the supervision of expert faculty (J.H.B. and J.H.L. with 20 and 11 years of thyroid US experience, respectively).
US-guided CNBs were performed using disposable 18-gauge double action, spring-activated needles (1.1 or 1.6 cm excursion; TSK Ace-cut; Create Medic, Yokohama, Japan) under local anesthesia with 1% lidocaine (9,17). The tip of the core needle was advanced into the edge or within the nodule using a freehand technique, and the stylet and cutting cannula of the needle were then fired sequentially. After CNB, each patient was observed while firm, local compression was applied to the biopsy site for 10–20 minutes (14).
Analysis of US findings and malignancy risk
US images were reviewed retrospectively and independently by two radiologists (S.R.C. and J.H.B. with 5 and 20 years of experience with thyroid US, respectively). Neither reviewer had any knowledge of the patients' clinical histories, previous imaging results, or cytopathology results. Any discrepancy between the two reviewers was resolved by consensus. US findings of the nodules were evaluated for the following features: shape (oval to round, irregular, or taller than wide); margin (well-defined, ill-defined, or spiculated); echogenicity (hyperechoic, isoechoic, hypoechoic, or marked hypoechoic); presence of echogenic dots suggesting microcalcifications; and presence of macrocalcifications. The following suspicious US features have been suggested by the Korean Society of Thyroid Radiology and Moon et al. (15,16): taller-than-wide shape, spiculated margin, marked hypoechogenicity, and presence of microcalcifications. A thyroid nodule with at least one suspicious US finding was classified as a suspicious nodule. The malignancy risk of these US-pathology discordant nodules was calculated, and this value was compared with the risk calculated using a web-based US risk system (
Analysis of histological results
CNB and surgical specimens were reviewed by a staff pathologist (S.D.E.) with 12 years of experience in thyroid cytopathology. Six categories of CNB results were reported in compliance with a proposal of The Korean Endocrine Pathology Thyroid Core Needle Biopsy Study Group (20). Non-diagnostic CNB reading (category I) included specimens with an insufficient number of follicular cells to facilitate appropriate diagnosis and specimens that were not representative of the corresponding US image (e.g., skeletal muscle and mature adipose tissue, virtually acellular specimen, acellular fibrotic nodule, and blood clot only). The benign category (category II) included all benign thyroidal and non-thyroidal findings, including benign follicular nodules (e.g., nodular hyperplasia, follicular adenoma, colloid nodules, and nodule in Graves' disease), Hashimoto's thyroiditis, subacute granulomatous thyroiditis, and non-thyroidal lesions (e.g., parathyroid lesion, benign neurogenic tumor, and benign lymph node). Category III comprised indeterminate lesions, which were subcategorized as indeterminate follicular lesions with nuclear atypia (IIIA) and indeterminate follicular lesions with architectural atypia (IIIB). Category IIIA included follicular proliferative lesions with focal nuclear atypia or atypical follicular cells embedded in fibrotic stroma, whereas category IIIB included microfollicular proliferative lesion specimens lacking a fibrous capsule or an adjacent normal thyroid tissue. Category IV included “follicular neoplasm or suspicious of a follicular neoplasm,” based on the presence of a fibrous capsule and microscopic features that differed from the adjacent thyroid parenchyma. A “suspicious of malignancy” (category V) CNB reading was defined by atypical features that were insufficient for a definite diagnosis of malignancy. The “malignancy” (category VI) CNB reading reflected specimens with unequivocal features of cancer. Immunohistochemistry data were not used as a basis for these readings.
Specific pathological diagnoses or descriptions such as the presence of hemorrhage, fibrosis, tissue granulation, calcification, infarction, atypia, mitoses, vascular proliferation, and thyroiditis were included for US-pathology discordant nodules (21 –23). Other histological findings that were not included in the above list were indicated in the pathological report.
For surgically confirmed malignant nodules with benign CNB results, the staff pathologist in thyroid cytopathology (S.D.E.) and two thyroid radiologists (S.R.C. and J.H.B) reviewed the US images and pathological specimens to identify the causes of discordance.
Statistical analysis
The IBM SPSS Statistics for Windows v19.0 (IBM Corp., Armonk, NY) was used for statistical analyses. Continuous variables are expressed as means ± standard deviations, and categorical variables are shown as percentages. To evaluate differences in demographic data between benign and malignant nodules, Student's t-test was used for continuous variables and the chi-square test or Fisher's exact test was used for binary variables. The latter tests were also used to analyze the incidence of each suspicious US features in benign (discordant) and malignant (concordant) thyroid nodules. Further, the chi-square test was used to evaluate any association between the number of suspicious US features and malignancy.
Results
In all patients, the CNB procedures were successful and well tolerated. The mean number of tissue cores obtained during a single CNB session was 1.3 (range 1–3).
CNB results and final diagnoses
Patients with benign and malignant nodules did not differ significantly with regard to clinical and demographic characteristics (Table 1).
Data shown are n (%) unless otherwise indicated.
Data indicate the mean ± standard deviation (range).
The criteria of the Korean Society of Thyroid Radiology and Moon et al. (15,16) were used to identify 210 US-pathology discordant nodules. Of these, 44 nodules were excluded because follow-up data were not available. This study finally included 166 patients (128 women and 38 men; M age = 53.8 years; range 22–77 years) with 166 thyroid nodules. The mean nodule size on US was 14.5 ± 10.8 mm (range 2–48 mm). For malignant nodules (n = 7), definite diagnoses were based on the histopathological results of surgical (n = 6) or repeated CNB (n = 1) specimens. For benign nodules (n = 159), the reference standard was based on the histopathological results of surgical specimens (n = 15), concordant benign results of repeated CNB or FNA specimens (n = 75), or stability on follow-up US for at least one year (n = 69).
Of the 166 thyroid nodules with suspicious US findings but benign CNB results, seven (4.2%) were finally confirmed as malignant. The pathological results of these seven malignant nodules included five (71.4%) papillary thyroid carcinomas (PTCs) and two (28.6%) follicular thyroid carcinomas. The CNB results of these malignant thyroid nodules were as follows: nodular hyperplasia (n = 5) and lymphocytic thyroiditis (n = 2).
Differences in suspicious US features between benign and malignant thyroid nodules
Table 2 compares the incidence of each suspicious US feature between benign and malignant thyroid nodules. None of the four suspicious US features was significantly associated with malignancy in isolation. However, malignant nodules had a significantly higher number of suspicious features than benign nodules (p = 0.002), particularly among nodules with more than two suspicious features.
Data shown are the number of nodules (%).
US, ultrasound.
Histological analysis of discordant nodules
According to the reference standard, 157 thyroid nodules with suspicious US features were diagnosed as benign. Histological analyses about the causes of discordance were available for 94 nodules (Table 3). The most common histological CNB feature was fibrosis (73/94; 77.6%), followed by thyroiditis (27/94; 28.7%), dystrophic calcification (10/94; 10.6%), old hemorrhage (6/94; 6.4%), foreign body reaction (1/94; 1.1%), vascular proliferation (1/94; 1.1%), and mild nuclear atypia (1/94; 1.1%). The 27 CNB specimens diagnosed as focal thyroiditis included 20 specimens of lymphocytic thyroiditis, five of chronic thyroiditis, and two of granulomatous thyroiditis.
A review of pathological slides and US images of CNB to determine the possible causes of discordance in the seven malignant thyroid nodules led to the conclusion that most cases were attributable to the mistargeting of thyroid nodules during CNB. In particular, the majority of biopsy specimens contained only normal thyroid parenchyma or lymphocytic thyroiditis, and the biopsy needle notch did not clearly target the center of the nodule, according to US. These lesions were usually posteriorly located to the biopsy needle.
Comparison of malignancy risk using various malignant risk systems
Table 4 demonstrates the malignancy risks of US-pathology discordant nodules under each US risk system. In this study, US-pathology discordant nodules had a malignancy risk of 4.2% (7/166), based on the criteria suggested by the Korean Society of Thyroid Radiology and Moon et al. (15,16). The malignancy risks ranged from 3.6% to 5.5% when other US risk systems were used: the lowest risk was observed with the French US risk system, whereas the ATA criteria yielded the highest risk.
www.gap.kr/thyroidnodule.php
K-TIRADS.
Discussion
A malignancy risk of 4.2% was determined among US-CNB pathology discordant nodules when using criteria suggested by the Korean Society of Thyroid Radiology and Moon et al. (15,16). Similar malignancy risks (3.6%–5.5%) were achieved when other US risk systems were applied to the data (1,9,18,19). All of these malignancy risks were somewhat lower than the risks associated with FNA discordance in previous studies (13.6%–56.6%) (3 –8). Therefore, clinicians should carefully consider re-biopsy or diagnostic surgical procedures for patients with US-CNB pathology discordant thyroid nodules because the risk of malignancy is relatively low. However, a residual risk of malignancy remains, particularly for discordant nodules with more than two suspicious US features. In other words, re-biopsy should be considered for US-CNB pathology discordant thyroid nodules with more than two suspicious US features.
US-FNA pathology discordant nodules require re-biopsy because of the known high malignancy risk, which can range from 13.6% to 56.6% (3 –8). As mentioned above, this study revealed a somewhat lower risk for US-CNB pathology discordant nodules (4.2%). A recent study revealed that 28/85 (32.9%) suspicious nodules with benign FNA results were histologically upgraded based on CNB analysis, and 27 (31.8%) were ultimately confirmed as malignant (3). This result suggests that CNB histological information enables a more reliable diagnosis of benign nodules with suspicious US features. False-negative FNA results may be attributed to the nature of the lesions, including subtle cytological features of PTC (particularly the follicular variant), intrinsic limitations of the procedure, and experience of the operator (3). The large amount of tissue provided by CNB enables a more precise and confirmative histological diagnosis and lower false-negative rate than FNA. Furthermore, interest in the use of CNB as a first-line diagnostic tool for thyroid nodules has increased. Several studies revealed that CNB of solid nodules yields a high level of diagnostic accuracy (97–98%) and a lower rate of inconclusive or non-diagnostic results (3.2–7.2%) than FNA (24 –27). Recently, Zhang et al. evaluated the diagnostic performance of CNB for suspicious thyroid nodules (26) and reported a malignancy rate of 2.3% among discordant thyroid nodules, which was lower than rate observed in this study (4.2%). This difference may be attributable to different definitions of suspicious US features in thyroid nodules. Zhang et al. (26) defined suspicious US features as hypoechogenicity, calcification (microcalcification or macrocalcification), irregular or microlobulated margin, intranodular vascularity, and taller-than-wide shape. In contrast, the stricter definition in this study included only marked hypoechogenicity (not hypoechogenicity), microcalcification (not macrocalcification), spiculated margin, and taller-than-wide shape. Intranodular vascularity of the solid portion on US is not a sufficiently suspicious feature in a thyroid nodule (1).
Various institutions and professional societies have reported US risk systems for the diagnosis of thyroid nodules (1,9,15,16,18,19). To generalize the results, some of these other US risk systems (ATA guidelines, Korean US risk system (K-TIRADS), French US risk system, and web-based US risk system) were applied to the data, and similar malignancy risks were achieved (1,9,18,19). These various US risk systems use different criteria to diagnose malignancy. According to the ATA guidelines (1), a highly suspicious nodule (malignancy rate >70–90%) is defined as a solid hypoechoic nodule or solid hypoechoic component of a partially cystic nodule with one or more of the following features: irregular margin (infiltrative, microlobulated), microcalcification, taller-than-wide shape, rim calcification with small extrusive soft-tissue component, and evidence of extrathyroidal extension. The Korean US risk system (K-TIRADS) guideline (9) defines a highly suspicious nodule (malignancy rate >60%) as a solid hypoechoic nodule with any suspicious US feature, including microcalcification, non-parallel orientation, and a spiculated/microlobulated margin. The French US risk system (19) defines categories 4B and 5 (respective malignancy rates >69% and >100%) as highly suspicious nodules. In contrast to the Korean US risk system (K-TIRADS), the French US risk system includes high stiffness on elastography as a suspicious feature. The web-based US risk system (18) is a 14-point risk scoring system based on several US features, and a nodule with a score of ≥8 is categorized as highly suspicious (malignancy rate >73%).
The histopathological analyses of US-pathology discordant nodules yielded similar results as those of previous reports. Fibrosis was the most common finding, followed by thyroiditis, dystrophic calcification, and old hemorrhage. The first finding is associated with decreased echogenicity of thyroid nodules. Several studies have revealed that benign cystic nodules may exhibit suspicious US features after spontaneous size reduction, aspiration of the cystic portion, and treatment with ethanol ablation (28 –33). Benign solid nodules can also mimic malignancy after size reduction on follow-up US (31). For a partially cystic nodule, a change in US features might be attributable to collapse of the cystic portion, infarction of the solid component, or internal hemorrhage, followed by replacement with fibrous tissue (29). During this process, the nodule will shrink and demonstrate marked hypoechogenicity, with an irregular or taller-than-wide shape and irregular or spiculated margin (19,33). For solid nodules, the mechanism underlying morphological change is unclear but might involve an imbalance of proliferating cells versus necrotic cells (31). This pathophysiology could explain why the majority of benign nodules in this study exhibited fibrosis, dystrophic calcification, and old hemorrhage. Moreover, 27 (28.7%) thyroid nodules in this study exhibited signs of thyroiditis on US. Thyroiditis is known to mimic thyroid cancer on US because inflammatory cells accumulating within the thyroid render the nodule markedly hypoechoic, and it can be associated with an ill-defined margin (34,35). Clinical and laboratory data are helpful for differentiating thyroiditis from thyroid carcinoma (34,35).
This study had several limitations. First, the retrospective design and specialized single-center location may have led to selection bias. Community hospitals with less expertise might obtain different results. Second, among the 159 benign nodules in this study, 69 were confirmed by size stability on follow-up US instead of surgery or re-biopsy. However, thyroid cancers can grow very slowly, and this follow-up period might not be sufficiently long to exclude a slow-growing malignancy. However, the definition of a benign nodule was based on previously published articles (3,6,24). Third, the diagnostic categories of CNB specimens have not been standardized. Nevertheless, the diagnostic categories proposed by The Korean Endocrine Pathology Thyroid Core Needle Biopsy Study Group were used, and an attempt was made to standardize diagnoses. Fourth, there was no definite indication for CNB of thyroid nodules, and CNB was performed according to the referring physician's preference. Finally, differences in follow-up loss rates might have affected the results in the various US risk-stratification systems. However, this factor was inherent to the retrospective nature of the study. In conclusion, malignancy risks of 3.6–5.5% were observed among US-CNB discordant thyroid nodules according to various US risk systems. Repeated biopsy may be necessary for selected thyroid nodules with more than two suspicious US features.
Footnotes
Author Disclosure Statement
None of the authors have disclosed any conflicts of interest regarding this article.