
Abstract
Background:
Increased incidence of small differentiated thyroid cancer (DTC) has emphasized the need for risk stratification and individualized disease management for these low risk DTCs. The aim of this study was to validate a new dynamic risk stratification (DRS) system for the prediction of structural recurrent/persistent disease in patients with DTC treated without radioactive iodine (RAI) remnant ablation therapy.
Methods:
This historical cohort study included 357 patients with DTC treated with lobectomy or total thyroidectomy without RAI therapy. We stratified patient response to initial treatment as excellent, indeterminate, biochemical incomplete, and structural incomplete according to the DRS system.
Results:
During a median follow-up of 8.6 years, 3.6% patients had structural recurrent DTC. The response was excellent in 71.7% patients, indeterminate in 18.5%, biochemical incomplete in 8.4%, and structural incomplete in 1.4%. There were significant differences in DFS among the DRS groups (p < 0.001). The hazard ratio (HR) of recurrent/persistent disease was significantly higher in the biochemical incomplete group (HR = 20.8, p < 0.001) and structural incomplete group (HR = 243.3, p < 0.001) compared with the excellent group. However, the Tumor Node Metastasis staging system and the American Thyroid Association initial risk classification did not effectively predict recurrence of DTC.
Conclusions:
The new DRS system was effective for predicting risk of recurrent
Introduction
T
The American Joint Committee on Cancer/Union for International Cancer Control (AJCC/UICC) Tumor Node Metastasis (TNM) staging system was developed to predict mortality, and is a standard tool for the initial risk assessment of patients with DTC (10,11). However, TNM staging is not ideal for assessing the risk of recurrence of DTC (12,13). The ATA initial risk stratification system is designed to predict the risk of recurrence or persistence in DTC patients, and classifies patients into low, intermediate, and high risk categories (6,14). However, many DTC patients initially categorized as intermediate risk have varied clinical outcomes. Therefore, the potential for personalized management using this system is limited (12,13).
Several studies have proposed dynamic risk stratification (DRS), using the response to initial therapy to guide individualized management of DTC patients (12). The DRS system classified patients into four response categories (i.e., excellent, indeterminate, biochemical incomplete, and structural incomplete), on the basis of clinical, biochemical, and imaging findings obtained during the first two years of follow-up (12,15). This restaging system helps clinicians identify patients with increased likelihood of recurrent or persistent structural disease and in need of careful monitoring (10,12). The DRS system has been generally accepted for DTC patients with total thyroidectomy and RAI remnant ablation therapy. A recent study proposed that DRS might also be used in patients with lobectomy or total thyroidectomy without RAI remnant ablation therapy (16). If it could predict recurrent/persistent disease in those low-risk patients with DTC, then it might be useful for guiding DTC management and follow-up.
In this study, we evaluated the DRS system in patients with DTC who underwent lobectomy or total thyroidectomy without RAI remnant ablation therapy. The aim was to validate the system for prediction of recurrent/persistent disease in these low-risk patients. We also compared the DRS system with TNM staging and ATA initial risk stratification for predicting clinical outcomes.
Materials and Methods
Patients
This historical cohort study initially included 463 patients with DTC who underwent lobectomy or total thyroidectomy without RAI remnant ablation therapy between 2005 and 2006 at Asan Medical Center, Seoul, Korea. A total of 104 patients who lacked sufficient follow-up data to determine their DRS group were excluded; the remaining 357 were evaluated. Prophylactic central neck dissection (CND) was routinely performed in 314 patients (88.0%) who underwent lobectomy and total thyroidectomy for papillary thyroid carcinoma (PTC). The study was approved by the Institutional Review Board of the Asan Medical Center.
Laboratory tests and follow-up protocol
After initial thyroid surgery, patients were routinely followed-up every 6–12 months with determination of serum thyroglobulin (Tg), anti-Tg antibody (TgAb), free thyroxine, and thyrotropin levels. Serum Tg was determined by immunoradiometric assay (Tg-plus RIA kit; BRAHMS AG, Henningsdorf, Germany). The functional sensitivity of the assay was 0.2 μg/L, with a coefficient of variation of 20%, and an analytical sensitivity of 0.08 ug/L. Serum TgAb were determined by radioligand assay (anti-Tg RIA kit; BRAHMS AG) with a functional sensitivity of 20 IU/mL. These assays have been previously described (17). Neck ultrasound (US) was performed every 6 months during the first year after surgery and repeated at 12–24 month intervals thereafter.
Risk stratification of DTC patients
The initial risk stratification was done using the seventh edition of the AJCC/UICC TNM staging system (11) and the ATA low, intermediate and high-risk categories (6). Patients were reclassified by the response to the initial therapy using the DRS definitions proposed by Momesso et al. (i.e., excellent, indeterminate, biochemical incomplete, or structural incomplete) (16,18). The best response during the first two years of follow-up was used to define the response to initial therapy. The level of nonstimulated Tg at a constant thyrotropin level was classified as stable, decreased, or increased following a >20% change in two consecutive measurements (16,19). Positive TgAb was defined as serum TgAb ≥60 IU/mL that interfered with the Tg measurement (17). The trend of TgAb change was defined as stable, decreasing, or increasing by comparing three consecutive serum TgAb values.
Definition of clinical outcomes
As previously defined, recurrent/persistent disease was cytological or histological evidence of DTC in suspicious lymph nodes (LNs), thyroid bed nodules, or highly suspicious metastatic lesions. We evaluated disease-free survival (DFS) without recurrent/persistent disease by the risk stratification criteria. Biochemical assays such as serum Tg or TgAb were not used to determine recurrent/persistent disease (16).
Statistical analysis
R version 3.0 was used to analyze data (R Foundation for Statistical Computing,
Results
Baseline characteristics of patients
A total of 357 patients with DTC were evaluated (Table 1). Their mean age was 46.3 ± 10.6 years, 91.0% were women and 95.5% had PTCs. The mean tumor size was 0.9 ± 0.7 cm and 91 patients (25.5%) had DTCs >1 cm. Central cervical LN metastases were found in 95 of the 357 patients (26.6%), and there were no patients with lateral cervical LN metastases. Two hundred ninety-three patients (82.1%) had a lobectomy and 64 patients (17.9%) had a total thyroidectomy without RAI therapy. Patients with a lobectomy were younger than those with a total thyroidectomy (p = 0.03). More central cervical LN metastases were found in patients with lobectomy than in patients with total thyroidectomy without RAI (p < 0.001) because RAI remnant ablation was done in most patients with cervical LN metastases after total thyroidectomy. There were no significant differences in pathological subtypes, tumor size, and TNM staging in the two groups (Table 1).
Categorical variables were described by numbers with percentages and continuous variables were described by mean and standard deviation.
Extrathyroidal extension, microscopic extrathyroidal extension.
TNM stage was determined by Seventh American Joint Cancer Committee TNM stage system.
Clinical outcome and risk stratification
Median follow-up after the initial surgery was 8.6 years (interquartile range 6.39–9.47). Recurrent/persistent disease was detected in 13 of 357 patients (3.6%). Eight patients had recurrent/persistent disease in the contralateral thyroid lobe after lobectomy. Seven patients underwent completion thyroidectomy and three of them received RAI remnant ablation treatment. The remaining patient was lost to follow-up. Three patients who underwent a lobectomy had recurrences in lateral cervical LNs. One of them underwent a completion thyroidectomy with modified radical LN dissection and RAI remnant ablation, one patient was treated with radiofrequency ablation, and the remaining patient was lost to follow-up. Two patients who initially underwent total thyroidectomy, had recurrences in the operative bed and were treated with radiofrequency ablation. The patients who underwent additional treatment presented no evidence of disease thereafter.
TNM staging classified 261 of the 357 patients (73.1%) as stage I/II and 96 (26.9%) as stage III. There were no stage IV patients. DFS was not significantly different in stage I/II and stage III patients (p = 0.67;Fig. 1A), and there was no additional risk of recurrence in stage III compared with stage I/II patients; hazard ratio (HR) 0.75 [confidential interval (CI) 0.2–2.7], p = 0.67 (Table 2).
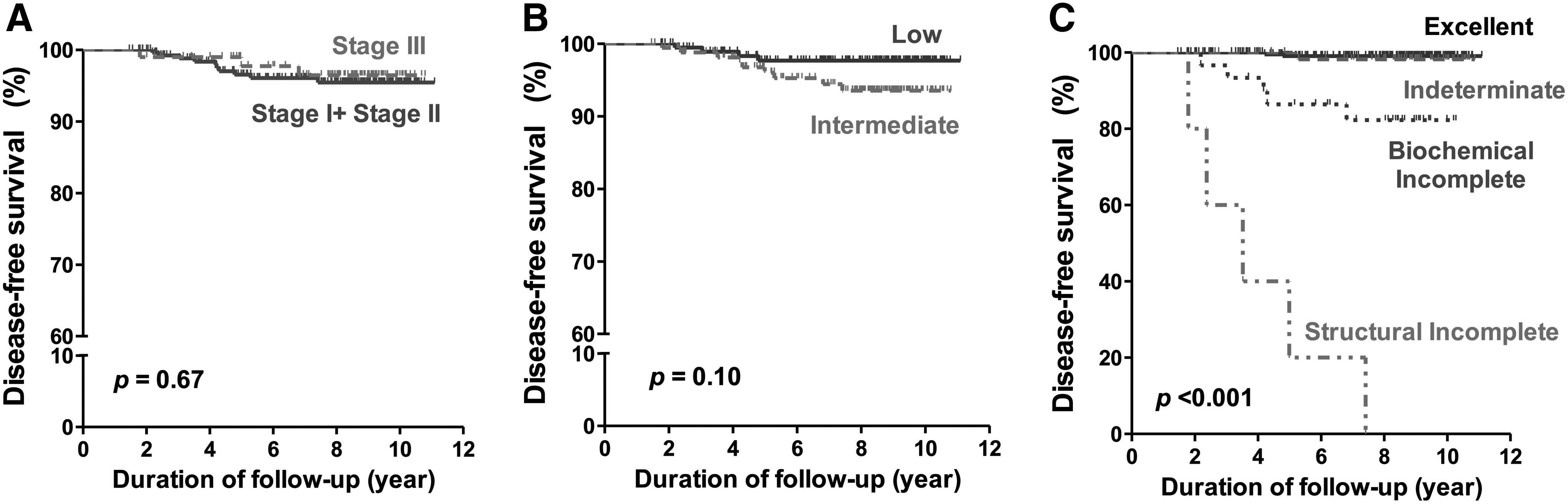
Disease-free survival (DFS) curves according to each staging system: American Joint Committee on Cancer/Union for International Cancer Control staging (
TNM stage was determined by Seventh American Joint Cancer Committee TNM stage system.
ATA, American Thyroid Association; CI, confidence interval; HR, hazard ratio; PVE, proportion of variation explained; Ref, reference.
ATA risk stratification resulted in 187 patients (52.4%) classified as low risk and 170 patients (47.6%) as intermediate risk. There were no high-risk patients. DFS in low-risk and intermediate-risk patients was not significantly different (p = 0.10; Fig. 1B). The risk of recurrent DTC did not differ significantly in the two groups (HR 2.56 [CI 0.79–8.32], p = 0.12; Table 2).
The DRS system classified 256 patients (71.7%) as having an excellent response, 66 (18.5%) with an indeterminate response, 30 (8.4%) with a biochemical-incomplete response, and 5 (1.4%) with a structural-incomplete response. After lobectomy, 201 patients (68.6%) had an excellent response, 58 patients (19.8%) had an indeterminate response, 29 patients (9.9%) had a biochemical incomplete response, and 5 patients (1.7%) had a structural incomplete response. After total thyroidectomy, 55 patients (85.9%) had an excellent response, 8 patients (12.5%) had an indeterminate response, 1 patient (1.6%) had a biochemical incomplete response, and no patients showed a structural incomplete response. There were significant differences in DFS among the patients (p < 0.001; Fig. 1C). The recurrence rate according to the DRS system was 0.78% (2/256) in the excellent response group, 1.5% (1/66) in the indeterminate response group, 16.7% (5/30) in the biochemical incomplete response group, and 100% (5/5) in the structural incomplete response group. The risk of recurrent/persistent disease was significantly greater in the biochemical-incomplete response (HR 20.8 [CI 4.0–107.1], p < 0.001) and structural-incomplete response group (HR 243.3 [CI 46.5–1272.1], p < 0.001) than in the excellent response group (Table 2). The risk of recurrent/persistent disease in the excellent response and in the indeterminate response groups did not differ significantly.
The ability of each risk stratification system to predict clinical outcome is shown in Table 2. The PVE value of the TNM staging system was 0.05%, and it was 0.74% with the ATA risk stratification system. At 12.18%, the PVE of the DRS was the highest, allowing a more reliable prediction of clinical outcomes in patients who underwent lobectomy or total thyroidectomy without RAI remnant ablation therapy.
Application of DRS in subgroups identified by ATA risk classification
We also applied the DRS system in low-risk and intermediate-risk subgroups defined by the initial ATA risk classification. In the ATA low-risk group, 72.7% (136/187) of patients were classified as having an excellent response, 17.6% (33/187) had an indeterminate response, and 9.6% (18/187) had a biochemical-incomplete response (Table 3). Of the 18 patients with a biochemical-incomplete response, three (16.7%) had recurrent/persistent disease during follow-up. There were significant differences in DFS among the DRS-group patients within the ATA low-risk subgroup (p < 0.001; Fig 2A). The risk of recurrence was higher in patients with a biochemical-incomplete response than in those with an excellent response (HR 22.48 [CI 2.34–216.10], p = 0.007; Table 4).
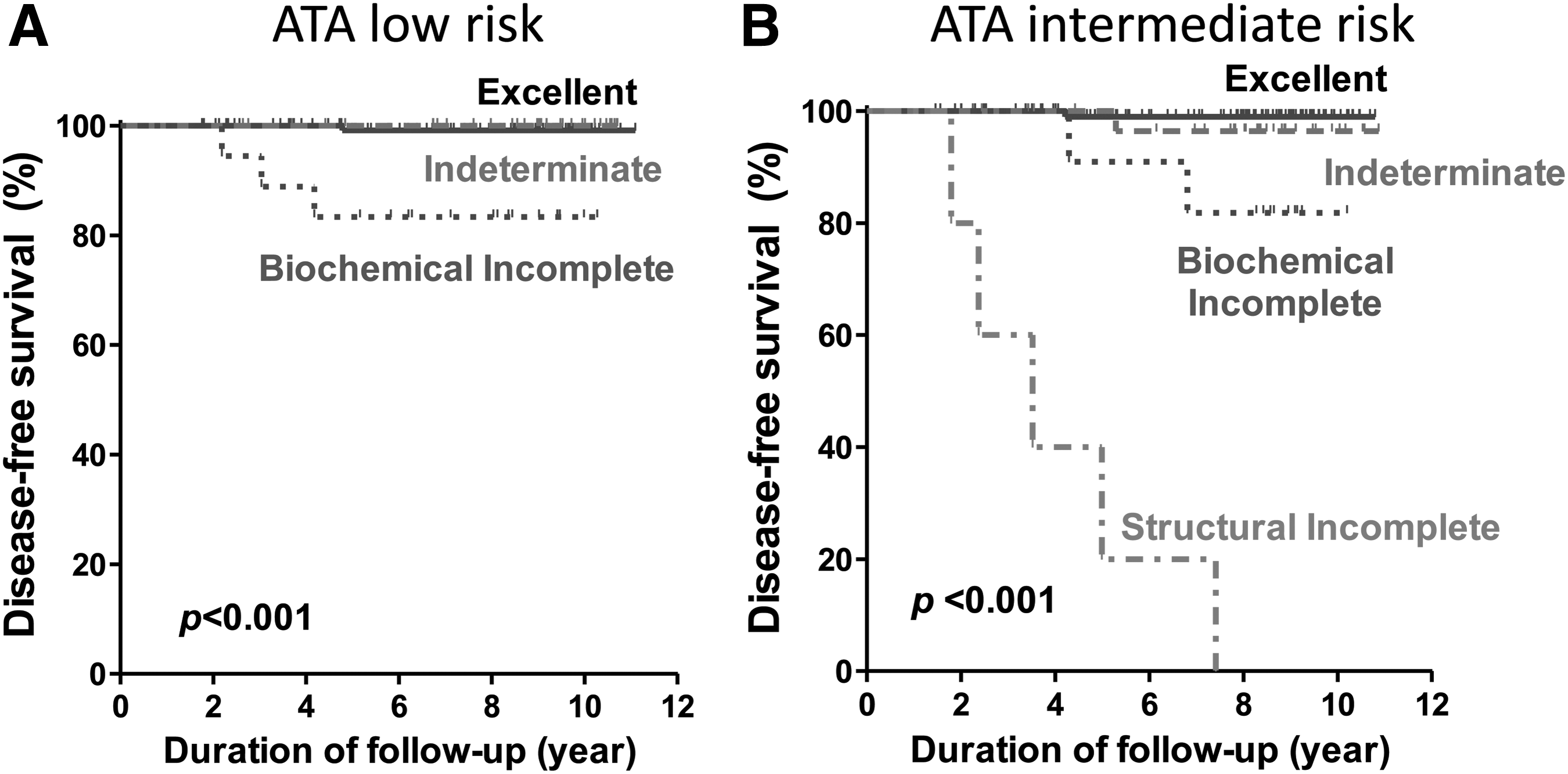
DFS curves according to DRS in each group of ATA risk stratification system: (
inf, infinity.
In the ATA intermediate-risk group, 70.6% (120/170) of patients were classified as having an excellent response, 19.4% (33/170) had an indeterminate response, 7.1% (12/170) had a biochemical-incomplete response, and 2.9% (5/170) had a structural-incomplete response (Table 3). Two of the 12 patients (16.7%) with a biochemical-incomplete response had recurrent/persistent disease during follow-up, and all 5 patients with a structural incomplete response had recurrent/persistent disease. There were significant differences in DFS among the DRS patients within the intermediate subgroup (p < 0.001; Fig 2B). The likelihood of recurrence was greater in the biochemical incomplete (HR 17.47 [CI 1.58–192.77], p = 0.019) and structural incomplete (HR = 240.01 [CI 27.53–2092.14], p < 0.001) groups than in the excellent response group. Recurrence risk in the indeterminate response (HR 3.27 [CI 0.20–52.26]) and excellent response group did not differ significantly (p = 0.40; Table 4).
Discussion
This study demonstrates that the newly proposed DRS is the most effective system for estimating the risk of recurrence in low and intermediate risk patients with DTC treated with lobectomy alone or total thyroidectomy without RAI remnant ablation therapy. We calculated PVE values to evaluate the predictability of clinically relevant outcomes. The DRS system had the highest PVE value compared with the TNM staging system and ATA initial risk classification. This study also confirms the clinical utility of the DRS system in patients classified as low risk and intermediate risk by the ATA initial risk criteria. Our study is the first to validate the DRS system as a new risk stratification system in a cohort different from the one in the original study.
TNM staging does not reflect the clinical risk factors related to recurrence of DTCs (6,10) and the initial ATA risk classification also has limitations for estimating the recurrence of DTCs, as shown in previous studies. The ATA risk classification provides only static estimates of risk at initial treatment. Furthermore, the ATA intermediate risk group includes patients with overlapping responses to and clinical outcomes of treatment (12,13). As expected, our data reveals no significant differences in DFS rates related to TNM staging and the ATA risk classification in DTC patients who were treated with lobectomy alone or total thyroidectomy without RAI therapy. However, the DRS system effectively predicted the risk of recurrence in those patients, and patients with incomplete responses had a significantly greater risk of recurrence than those with excellent responses. Our findings support the use of the DRS system in individualized risk stratification and management of DTC patients without RAI therapy.
A cutoff value of serum Tg that discriminates normal residual thyroid tissue from recurrent or persistent disease in DTC patients with lobectomy has not been established (6,8,19). The ATA guidelines recommend evaluating neck US imaging and serial Tg level during follow-up of these patients (6), but they do not specify the frequency of follow-up or a cutoff Tg level. Therefore, in these patients, risk assessment is mainly depending on stratification by initial static risk (8). A previous study proposed a nonstimulated Tg value of 30 ng/mL in patients who underwent lobectomy as a reasonable recurrence risk cutoff value. This value was based on observations that remnant normal thyroid tissue produces about half the Tg produced by the normal thyroid gland (reference range 20–60 μg/L). We adopted this cutoff value in our cohort. Serum TgAb are known to be a predictive marker of recurrence in patients with DTC (22,23), but the interpretation of TgAb level is difficult in the presence of remnant thyroid tissue. As accepted criterion for interpreting the trend of TgAb (16,18), we used three consecutive TgAb values.
Only two of the 256 patients (0.8%) in the excellent response group experienced a disease recurrence. They were diagnosed with recurrent disease 4 and 5 years after lobectomy, respectively. One patient was diagnosed with recurrent PTC manifesting as a hypoechoic ill-defined nodule in the contralateral lobe on neck US and a sudden increase in serum TgAb levels with a stable serum Tg level. The other patient presented only with suspicious US finding without biochemical changes. The majority of disease recurrences in low or very low ATA risk classification DTC patients occur within the first 3–5 years after the initial surgery, but late relapses have been identified up to 10 years after the initial surgery (24,25). These finding suggest that neck US imaging and biochemical testing should be continued at suitable intervals even after 10 years, and that reevaluation of risk may be needed at any time during follow-up. Further investigation is needed to determine the optimal follow-up intervals for each risk group.
The DRS system using response to therapy in DTC patients was validated in two cohorts from the United States and Brazil (16). The baseline characteristics of the patients enrolled in our present study were different compared to those of previous studies. First of all, the number of patients who underwent total thyroidectomy without RAI remnant ablation was smaller compared to those who underwent lobectomy without RAI therapy compared to other studies. Second, our cohort did not include patients with TNM stage IV disease and lateral neck lymph node metastasis. Third, most patients underwent prophylactic CND at their initial surgery in this cohort. Our study is of relevance because it is the first study to validate the DRS system in an Asian patient cohort.
Our study has some limitations related to its retrospective design. The number of patients with confirmed recurrent DTC during follow-up was relatively small. As the time for disease recurrence in low risk DTC patients can be very long (24,25), the 8.6 year median follow-up period in this study might not be sufficient. However, this is a valuable study to confirm the clinical utility of the DRS system in patients who underwent lobectomy or total thyroidectomy without RAI remnant ablation therapy.
In conclusion, we demonstrate that the newly proposed DRS system using the response to initial therapy gives valuable information for estimating recurrent/persistent disease in patients with DTC who were treated without RAI remnant ablation therapy. The DRS system predicts recurrence even in the low risk and intermediate risk ATA initial risk subgroups. DRS might provide important insights to tailor follow-up for low-risk patients with DTC given less aggressive treatment.
Footnotes
Acknowledgment
This study was supported by the National Research Foundation of Korea Research Grant No. NRF-2015R1C1A1A02036597.
Author Disclosure Statement
The authors have no competing financial interests to disclose.