
Abstract
Background:
Thyroid cancer (TC) is the most common endocrine malignancy. TC patients have a good prognosis and a low disease-related mortality rate. Since such patients are often young, they may be at a higher risk for a second primary malignancy (SPM). This study sought to determine the incidence, risk, and types of SPM between 1980 and 2011, and to assess SPM trends over time among Israeli TC patients.
Methods:
Data were derived from the Israel National Cancer Registry. Primary TC patients diagnosed during 1980–2009 were followed up for SPM incidence until December 31, 2011. Standardized incidence ratios (SIRs) of observed to expected SPM (based on the general population rates) were calculated using Poisson regression. Analyses were stratified by time period of initial TC diagnosis (1980–1995 and 1996–2009).
Results:
A total of 11,538 TC patients were identified. After exclusion of 107 duplicate cases, records of 1032 patients with SPM were analyzed (an SPM incidence of 8.9%). SIRs for all-site SPMs were 1.23 [confidence interval 1.08–1.35] for males and 1.19 [confidence interval 1.10–1.27] for females. SIRs for tumors of the urinary system and prostate were significantly elevated in males, as were SIRs for tumors of the brain, urinary system, breast, and lung in females. Variables associated with increased risk of developing SPMs included a younger age at TC diagnosis, a shorter latency period, being born in Asia/Africa for both sexes, and being born in Israel for females. Compared with the general population, a subanalysis by TC diagnosis during 1980–1995 and 1996–2009 disclosed a higher SPM incidence for the latter time period in males and for both time periods, with a slightly higher SIR for the latter time period in females.
Conclusions:
The overall risk of SPM in Israeli TC patients was significantly greater for both sexes compared with the general population, thus identifying TC patients as a high-risk group and calling for caretakers to apply specific follow-up guidelines.
Introduction
T
The age-standardized incidence rates of TC have increased in Israel over the past decades from eight new cases per 100,000 persons in 1980 to 15 new cases per 100,000 persons in 2012 (9). More than 12,000 patients in the current Israeli population have been diagnosed with TC, and about 800 new cases are reported each year (5). Israel is a multi-ethnic society, containing populations from all over the world. Approximately 75% of the population are Jewish, of whom 74.4% are Israeli born, 17.4% are European/American born, 5.1% are African born (mostly Northern Africa), and 3.1% are Asian born (mostly Western Asia). Arabs make up most of the non-Jewish population (21% of the total Israeli population) (10).
TC is diagnosed more frequently among younger than older populations (1,11,12). Two-thirds of TC patients are women, with a peak incidence (23.9%) seen in people at 45–54 years of age (7). Patients with DTC generally have an excellent prognosis, and their overall five-year survival rate is >95% (13,14). However, because of the long life expectancy, an increased incidence of second primary malignancy (SPM) may be expected.
Several studies from different continents have reported an increased risk of SPM in patients with TC. One European cohort demonstrated that the rate of SPM was 27% higher in TC patients relative to the corresponding general population (15), and a British pooled analysis of 13 cancer registries showed a 31% increase in the risk for a SPM among TC patients (16). Analysis of the Surveillance, Epidemiology, and End Results (SEER) registry for the period from 1973 through 2002 indicated a 9% increase in the incidence of SPM in TC patients (17). A Taiwanese population-based study revealed a 33% higher rate of SPM in TC patients relative to the corresponding general population (18). A recent population-based study from Korea demonstrated a 6% increase in SPM among patients with TC (19).
Using data from the Israel National Cancer Registry (INCR), the risk of a SPM in a cohort of TC patients diagnosed in Israel between 1980 and 2009 was examined. Specifically, the first aim of this study was to evaluate and compare the SPM rates among TC patients of different ethnic populations in Israel. The second aim was to investigate whether patients diagnosed with TC from 1981 to 1995 had a different SPM rate than those diagnosed from 1995 to 2009, both compared to the general population.
Methods
This was a historical cohort study, based on the records of the INCR.
Data source
The INCR was established in 1960 under the auspices of the Israeli Health Ministry. New cancer cases diagnosed in Israel are subjected to mandatory reporting to the INCR since 1982, and they are coded according to the Standard International Classification of the Disease for Oncology (ICD-0-3). Although reporting on cases diagnosed outside the country is not mandatory, the INCR mostly includes information on them, thanks to cross-reporting. Data collected by the Registry are based on a personal identification number that is given to all Israelis at birth or upon immigration to the State, and they include demographic characteristics, date of diagnosis, and the site, laterality, and histological type of the tumor. The completeness of the INCR for solid tumors is about 95% (20), and was considered to be very high prior to 1982 as well.
Study cohort
This study consisted of individuals with a first primary malignancy of TC, who were identified by site code ICD-0-3:C739 between January 1, 1980, and December 31, 2009, as reported to the INCR database. Exclusion criteria were the presence of another primary malignancy before the diagnosis of TC and inaccurate pathological diagnosis. The date of TC diagnosis was considered the beginning of patient data observation. The end of the follow-up observation was either December 31, 2011, the date of SPM diagnosis, or the date of death, whichever occurred earlier. No data were available with respect to emigration.
Outcome ascertainment
The SPM incidence was based on linkage with the INCR database and on identifying SPM cases diagnosed from 1981 to 2011. Any SPM detected within the first year of follow-up after TC diagnosis was defined as synchronous and was excluded from the study analysis. Following the guidelines of the International Agency for Research on Cancer (21), cases of duplicate SPMs were excluded.
Statistical analysis
Standardized incidence ratios (SIRs) and corresponding confidence intervals (CIs) for SPM were calculated as the ratio of the observed number of SPMs in the TC cohort to the expected number of cancers using Poisson regression. The expected number of cancers was calculated based on the cancer incidence in the corresponding general population. Stratified analyses were conducted by various characteristics of the first TC, which included place of birth, histological subtypes of the TC (papillary, follicular, medullary, and anaplastic), age at initial diagnosis of the TC, latency period (time between TC diagnosis and SPM diagnosis), and calendar years of diagnosis of the TC (1980–1995 and 1996–2009). Stage at TC diagnosis was not analyzed largely due to missing data in the INCR. The selection criterion for SIR calculation of different cancer types was five or more cases of SPM in each cancer type. All statistical tests were two-sided, and CIs and p-values were at 0.05 significance alpha levels. All analyses were performed using JMP Statistical v10.0 (SAS institute, Inc., Cary, NC).
Results
Patient characteristics
A total of 13,263 patients with an initial diagnosis of TC were registered in Israel between 1980 and 2009. Of them, 1093 individuals with TC as a SPM and another 632 individuals with an incomplete pathological diagnosis were excluded from the study, leaving 11,538 patients with TC as the first malignancy for the study analysis (Fig. 1).
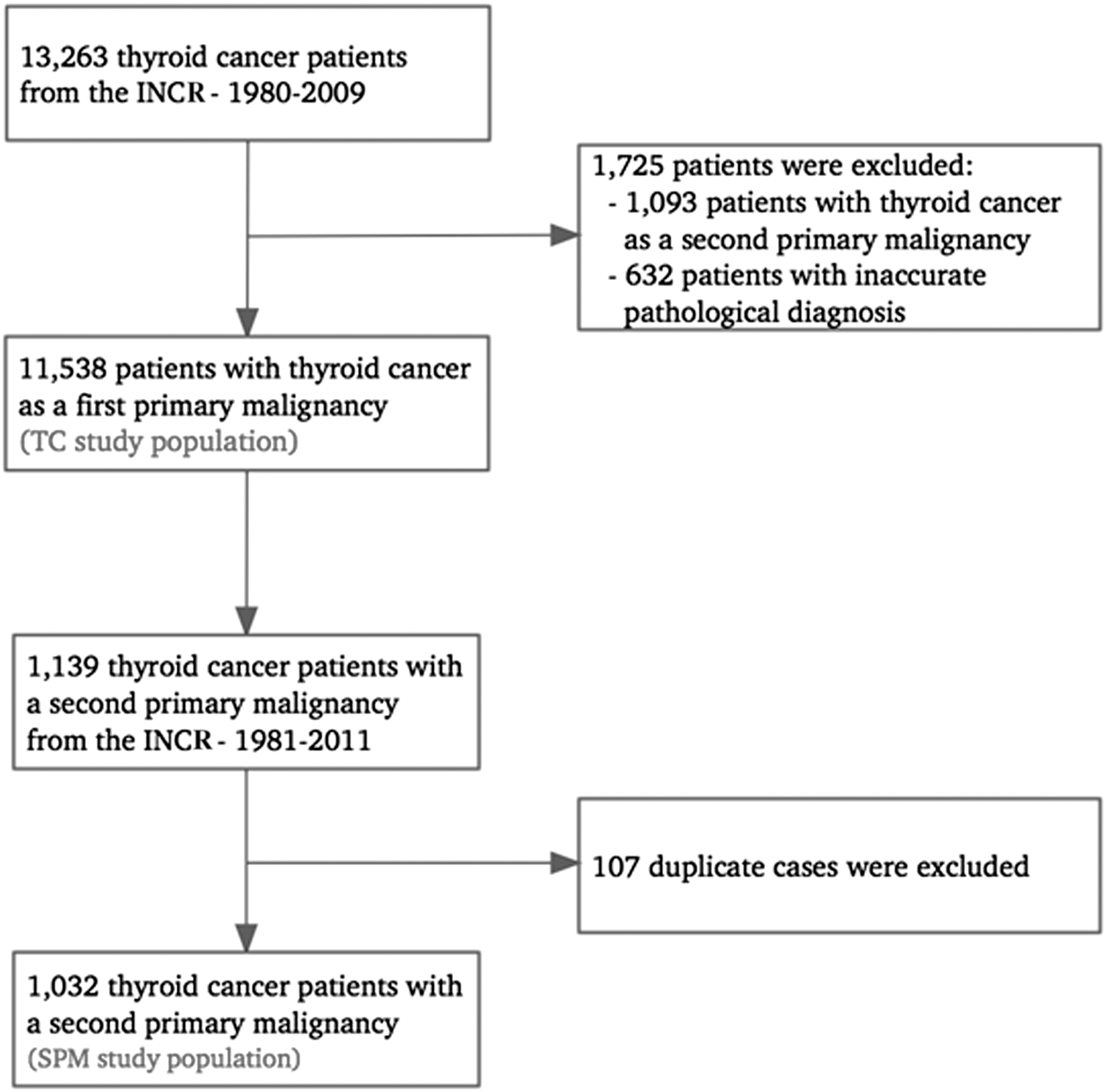
Flow chart of the TC patient cohort. INCR, the Israeli National Cancer Registry; TC, thyroid cancer; SPM, second primary malignancy.
The mean follow-up period for the study cohort was 9.7 years (range 1–30 years). The ratio of Jews to Arabs with a TC diagnosis was 10:1. The ratio of females to males with a TC diagnosis was 3.3:1 among the Jews and 3.6:1 among the Arabs, and the mean age at TC diagnosis was 51.2 and 41.4 years, respectively (Table 1). Males and females up to 59 years of age had the highest incidence of TC compared with other age groups (p < 0.001).
Chi-square test for categorical variables and t-test for continuous variables.
M, males; n, number of patients; IR, incidence rate in the study population; F, females; SPM, second primary malignancy; As/Afr, Asian/African-born Jews; Eu/Am, European/American-born Jews; Uk, unknown; SD, standard deviation; DTC, differentiated thyroid carcinoma; ns, non-significant.
The age-adjusted incidence of TC per 100,000 person years increased from six on average during 1980–1984 to 16 on average during 2005–2009 in Jewish females, and from two on average to six on average in Jewish males, respectively.
The crude TC incidence increased fivefold from 1980–1984 to 2004–2009 (736 to 3801 cases), while the Israeli population only doubled during the same time. The vast majority of TCs were of the papillary type (85%; Table 1).
Risk for a SPM
Among the 11,538 patients with primary TC, 194 cases of synchronous SPM were detected within the first year after TC diagnosis, and 1139 metachronous SPM cases were detected one year or more after TC diagnosis. After exclusion of 107 duplicate cases, overall, 1032 individuals with the metachronous SPM were included in the study analysis, of whom 764 (74%) were female. Table 1 compares characteristics between the total study cohort and the subgroup with SPM. There was a 10-year age difference at the time of TC diagnosis between the Jewish and the Arab populations (51.2 and 41.4 years, respectively; p < 0.001), and a similar 10-year gap between the Jewish and Arab populations at the time of SPM diagnosis (63.5 and 52.9 years, respectively; p < 0.001). The mean latency period from the first primary TC to SPM diagnosis was 8.6 years.
The overall SIRs for SPMs were significantly elevated among both the Jewish males (SIR = 1.23 [CI 1.08–1.35]) and the Jewish females (SIR = 1.19 [CI 1.10–1.27]; Table 2). The SIRs for SPMs among the Arab males (SIR = 1.26 [CI 0.48–2.05]) and the Arab females (SIR = 1.35 [CI 0.83–1.88]) showed similar trends but with larger CIs, most probably due to the small numbers of the TC cases in this population.
Bold denotes significance level of p < 0.05.
Obs, observed; Exp, expected; SIR, standardized incidence ratio of second primary malignancy; CI, confidence interval.
The following analyses by selected characteristics of the original thyroid tumors and SPMs were restricted to the Jewish population only, due to the small number of the Arab persons diagnosed with TC in this database (about 15 cases annually during 1980–1995), which prevented further stratifications. For the Jewish males, the two significantly numerous sites of SPM were the urinary system (including tumors of the bladder, the urethras, the ureter, and the kidney; SIR = 1.53 [CI 1.08–1.98]) and the prostate (SIR = 1.39 [CI 1.02–1.76]; Table 3). There was an elevated risk for SPM in the Jewish females mostly at four sites: the brain (SIR = 2.37 [CI 1.75–3.0]), the urinary system (SIR = 1.57 [CI 1.09–2.04]), the breast (SIR = 1.44 [CI 1.26–1.61]), and the lung (SIR = 1.43 [CI 1.00–1.87]; Table 3).
Bold denotes significance level of p < 0.05.
CNS, central nervous system; NHL, non-Hodgkin's lymphoma; UCCOC, uterine cervix and corpus ovary cancer; CRC, colorectal cancer; Gastro, gastrointestinal cancer.
SIRs of SPMs following TC diagnosis by selected characteristics are listed in Table 4. Excess of SPMs was observed for all Jewish TC patients, but was higher in those diagnosed with TC before 50 years of age compared with those diagnosed at a later age in both males (SIR = 1.57 [CI 1.18–1.96] and SIR = 1.15 [CI 0.99–1.31], respectively; p < 0.001) and females (SIR = 1.37 [CI 1.21–1.53] and SIR = 1.1 [CI 1.00–1.20], respectively; p < 0.001).
Bold denotes significance level of p < 0.05.
TC, thyroid cancer; MTC, medullary thyroid carcinoma.
The risk of a SPM among the Jewish population appeared to be particularly higher among the Asian/African-born males and females (by 37% and 25%, respectively; SIR = 1.37 [CI 1.04–1.38] and SIR = 1.25 [CI 1.06–1.44], respectively) and among the Israeli-born females (by 26%; SIR = 1.26 [CI 1.09–1.43]) compared with the corresponding general population (Table 4).
SPM incidences differed according to the histological subtypes of the initial TC. The risk for SPM in the DTC histological subtype was increased by 27% in males and by 19% in females (SIR = 1.27 [CI 1.12–1.43] and SIR = 1.19 [CI 1.1–1.28], respectively). However, the risk of SPM in male patients with medullary and anaplastic histological subtypes of TC did not differ from that of the general male population (SIR = 0.78 [CI 0.2–1.36]). In contrast, the SPM incidence among females with those histological subtypes was significantly increased (SIR = 2.09 [CI 1.15–3.03]) compared with the general female population.
Stratification of SPM by latency period (Table 5) showed that the SPM incidence was most elevated within the first nine years of TC diagnosis in males (1–4 years: SIR = 1.35 [CI 1.08–1.63]; 5–9 years: SIR = 1.38 [CI 1.08–1.69]). The SPM incidence in females was significantly elevated within the first 14 years of TC years of TC diagnosis (1–4 years: SIR = 1.41 [CI 1.24–1.58]; 5–9 years: SIR = 1.27 [CI 1.10–1.44]; 10–14 years: SIR = 1.21 [CI 1.01–1.40]).
Bold denotes significance level of p < 0.05.
Obs, observed cases; Exp, expected cases; SIR, standardized incidence ratio of second primary malignancy; CI, confidence interval; TC, thyroid cancer; SPM, second primary malignancy.
The risk of SPM in patients diagnosed with TC in 1981–1995 was different from that of TC patients diagnosed in 1995–2009. Compared with the general population, SPM occurrence was significantly higher (by 40%) for males diagnosed with TC during 1996–2009 but not for those diagnosed during 1980–1995 (SIR = 1.40 [CI 1.18–1.62] and SIR = 0.97 [CI 0.79–1.16], respectively; p < 0.001). However, SPM occurrence among females was elevated in both time periods, with a slightly higher risk during 1996–2009 compared with 1980–1995 (by 21% and by 17%; SIR = 1.21 [CI 1.09–1.33] and SIR = 1.17 [CI 1.05–1.29], respectively; p = 0.09; Table 4).
Discussion
There were a total of 1032 (8.9%) cases of metachronous SPM during a 30-year follow-up period in this nationwide cohort of 11,538 TC patients. Compared with the expected rates in the general population, the overall incidence of a SPM was significantly elevated—by 23% and 19%—for Jewish males and females with TC, respectively. Studies from the United States, Europe, and Asia have reported an increased overall risk of SPM subsequent to TC diagnosis in the range of 6–31% (15 –17,19,22,23).
In order to assess the metachronous SPM, only cases of SPM were included that were diagnosed at least one year following the diagnosis of thyroid cancer in the study. Previous studies defined a lag period as short as two to three months (19) or six months (24). It is unlikely that a SPM would develop within such a short time period, and when such a definition is used, it may cause an overestimation of the SPM incidence.
In the current study, the risks of SPM following TC were significantly elevated for all-site, urinary system, and prostate cancers in males, and for all-site, brain, urinary system, breast, and lung cancers in females. Others have reported solid cancer sites of higher risk for SPM in TC patients as being salivary gland, breast, kidney, brain, bone, colon, prostate, lung, bladder, nasopharynx, thymus, adrenal gland, and stomach, while the most common non-solid cancer types were non-Hodgkin's lymphoma, multiple myeloma, leukemia, and soft-tissue sarcoma (15 –17,23,25 –31).
The present findings indicate that the risk for SPM is associated with being aged <50 years at the time of TC diagnosis, as well as with a short latency period between TC and SPM diagnosis. The incidence of SPM following the initial TC diagnosis was mostly elevated within the first decade in males and within the first 14 years in females. A U.S. study with up to 30 years of follow-up also reported that a younger age at the time of the initial TC diagnosis was linked to a greater risk for SPM among individuals with first TC. In that study, SPMs were detected at similar rates in males and females, and more often within five years of TC diagnosis (17).
One of the specific aims of this study was to investigate whether patients diagnosed with TC between 1981 and 1995 had a different SIR of SPM than those diagnosed between 1995 and 2009. An elevated overall risk of SPM was found among the Jewish males diagnosed during 1996–2009, but not in those diagnosed during 1980–1995. For the Jewish females, although the rate of SPM was significantly elevated during both study periods, the SPM risk during 1996–2009 was slightly higher than that during 1980–1995 (21% vs. 17%; p = 0.09), possibly implying a tendency of increased risk over time. The changes in treatment guidelines may explain, at least in part, the differences observed during the two study periods. From the end of 1990 until 2009, when new guidelines for the treatment of thyroid cancer were published, the trend in Israel was to treat TC with radioiodine (RAI) after thyroidectomy, even in cases of microcarcinomas and low-risk carcinomas, in order to cause thyroid remnant ablation and to prevent recurrence and metastasis. During 1996–2009, the use of RAI as treatment for TC increased significantly in the United States as well, a trend that was attributed predominantly to hospital treatment protocols (32).
Several studies have shown a greater risk of SPM following TC in RAI-treated than in non-RAI-treated individuals (17,33 –37). A recent analysis of the SEER cancer registry (1973–2008) showed an elevated SPM incidence in RAI-treated patients, with a particularly increased risk for salivary gland cancer, and no excess risk in non-RAI-treated patients (31). In a Hong Kong study, RAI was the only independent risk factor for SPM, after adjusting for age, sex, period of DTC diagnosis, and stage of DTC. Elevated rates of bone and soft-tissue, colorectal, and salivary gland cancers were detected among individuals treated by RAI for TC in Europe (15), but not in the current study. The absence of data on RAI treatment is a limitation of the current study.
Indeed, the specific distribution of SPM sites may be related to the RAI treatment administered to TC patients. The sodium iodide symporter (NIS), a transmembrane protein, is essential for the active transport of iodide across the basolateral membrane of follicular cells in the thyroid gland (38). NIS mRNA and protein are also expressed in a variety of extrathyroidal tissues, including the salivary glands, mammary glands, gastric and colonic mucosa, and the renal tubular system (38 –41). Iodide is excreted by the kidneys, digestive tract, and saliva. The expression of NIS in these tissues may cause exposure of the related organs to ionizing radiation, which may potentially initiate carcinogenesis (42). Multiple factors unrelated to RAI treatment may have also contributed to the elevated risk of SPM in TC patients, and to differences in the rates and sites observed between various studies. Such factors include unhealthy life-style behavior (43 –45), germline and somatic mutations, environmental factors, and methodological factors, such as length of follow-up (45 –50).
The SPM rate differed by ethnicity among the study participants. The risk for SPM was pronounced for both Jewish Asian/African-born males and females and for Israeli-born Jewish females. Factors associated with this differential effect may be environmental and genetic.
A number of genetic factors have been found to be associated with TC, such as a high frequency of BRAF and RAS mutations (46). BRAF mutations are also observed in head and neck cancer, non-small-cell lung cancer, colorectal cancer, and skin melanoma (47 –50). RAS mutations have been reported in multiple malignancies, with the highest incidence in tumors of the pancreas, colon, and lung (51). Rearrangements of the RET protooncogene, which have been associated with papillary TC, have also been associated with breast cancer, prostate cancer, and leukemia (52 –54). Mutation of the checkpoint kinase 2 (CHEK2) gene (55), the multi-organ cancer susceptibility gene that is crucial in the DNA repair process, may increase the risk for SPM in individuals with TC as well as other types of cancer. Furthermore, Cowden syndrome patients with underlying germline PTEN mutations are at increased risk of breast, thyroid, endometrial, and renal cancers, as well as being at higher risk for SPMs than the general population (56). An assessment of genetic associations to the findings is not within the scope of this study.
An increased risk of breast cancer in females, and of prostate cancer in males, was found compared with the expected rates in the general population. Beyond the potential links to treatment-related, genetic, and environmental factors, this finding raises the possibility of a surveillance bias: patients diagnosed with TC may undergo more intensive examinations than the general population, especially with respect to cancers for which there are well-attended screening programs, such as breast and prostate cancers.
The strength of the current investigation is the long-term follow-up of a relatively large nationwide cohort (11,538 TC patients). This is the first study to investigate trends of SPM in the Israeli TC patient population and to identify TC patients at risk for a SPM.
One of the limitations of this study is the lack of follow-up on emigrated patients. However, the rate of emigration from Israel is very low (0.44% in 1995) and has been decreasing in recent years (0.19% in 2014) (57). It is likely that among TC patients, this rate is even lower, since Israel has a National Health Insurance Law that ensures full treatment to all citizens. Therefore, the potential selection bias is not expected to be large or to affect the SIR estimates substantially. It is recognized that the most important limitation of the current study is the incomplete information on tumor size, stage of TC, and types of treatment received by each patient. This limitation precludes attempts to distinguish between the impact of detection patterns on the temporal changes and the differences observed between subpopulations, as well as discern the impact of these characteristics on the risk for SPMs.
In conclusion, the risk of SPM in Israeli patients with primary TC is higher than expected based on the general population rates and tended to increase over time (1996–2011 vs. 1981–1995). Predilection for the emergence of SPM at specific time windows and subpopulations further emphasizes and perhaps provides additional tools for the long-term surveillance in the post-treatment period.
Footnotes
Acknowledgments
Esther Eshkol is thanked for editorial assistance.
Author Disclosure Statement
The authors have nothing to disclose. No competing financial interests exist.