
Abstract
Background:
Papillary thyroid carcinomas (PTC) in the pT3 category constitute a heterogeneous group of tumors with a variable risk of recurrence. The objectives of this study were (i) to estimate disease-free survival (DFS) and identify prognostic factors associated with recurrence in a cohort of pT3 PTC, and (ii) to evaluate the concept of delayed risk stratification in a cohort of pT3 tumors.
Methods:
A total of 560 patients with pT3 PTC, treated and followed at the authors' institution, were studied. They were divided into three groups: group 1, pT3 ≤10 mm; group 2, pT3 >10 mm with extrathyroidal invasion (ETI); and group 3, pT3 due to a tumor size >4 cm. DFS was estimated using the Kaplan–Meier method, and associated prognostic features were studied in univariate and multivariate Cox model–based analyses in each group. Then, DFS was studied for each group according to the six- to eight-month status (remission or not).
Results:
DFS at 10 years was 75% for the entire cohort and was 89%, 67%, and 82% in groups 1, 2, and 3, respectively (p < 0.0001). Multivariate analysis identified three factors significantly associated with reduced DFS: lymph node (LN) involvement, male sex, and group 2 (>1 cm with ETI). A trend toward a worse prognosis in patients with pT3 N0/Nx PTC >10 mm with ETI was found in comparison with the other pT3 N0/Nx patients. When the six- to eight-month checkup was normal, the DFS at 10 years increased to 98%, 96%, and 91% in groups 1–3, respectively. Furthermore, in this case, initial LN involvement no longer seemed to affect the prognosis in those groups.
Conclusion:
PTC ≤10 mm with ETI and large tumors >4 cm without ETI both have a low-recurrence risk when there are no adverse associated prognostic features such as LN involvement. LN involvement, especially in the lateral compartment (N1b), is a strong prognostic factor of recurrence in pT3 PTC. Delayed risk stratification can be applied in pT3 PTC patients. Those cured at the first checkup, including those with limited LN involvement, have excellent outcomes, which should prompt clinicians to adapt subsequent management accordingly.
Introduction
A
Regarding size, large intrathyroidal tumors are upgraded to the pT3 category when the tumor size reaches 4 cm, based on previous data demonstrating higher cumulative risk of recurrence (2,3) or distant metastases (4) with increasing tumor size. However, provided there is no aggressive histology or massive lymph node (LN) metastases, these intrathyroidal pT3 tumors are included in the low recurrence risk category of the 2009 and 2015 ATA risk stratification systems (5,6), including intrathyroidal, encapsulated follicular variants of papillary thyroid carcinoma (PTC), which are now considered to have the lowest recurrence risk (1–2%) (6). This excellent prognosis contrasts with that of pT3 PTC in general, which varies between 3% and 10% and can even reach 40% in the presence of a BRAF mutation (6).
Regarding ETI, it has been well demonstrated that massive ETI alters the outcome of PTC (7,8). PTC presenting with minimal ETI (i.e., into the sternothyroid muscle or perithyroidal soft tissues) are included in the pT3 category whatever the size of the tumor and are considered to have an intermediate recurrence risk (5,6). It should be noted that minimal ETI significantly increases the risk of LN metastases (9 –11). However, previous data suggest that papillary microcarcinomas with minimal ETI have excellent outcomes (12 –14), and thus upstaging to the pT3 and intermediate recurrence risk category may not be justified. Others have also suggested that minimal ETI does not affect the recurrence-free survival of patients with PTC measuring up to 4 cm (7,14).
First, this study focused on pT3 PTC to estimate disease-free survival (DFS) for the entire cohort and for each subgroup of pT3 tumors (micro pT3 ≤1 cm, 1–4 cm pT3 with ETI, large pT3 >4 cm without ETI) and also according to the degree of LN involvement (nodal metastasis in the central or lateral compartment). The prognostic factors associated with a disease-related event were analyzed for the entire cohort of pT3 PTC patients. The outcomes of pT3 N0/Nx PTC patients were also analyzed to evaluate whether ETI is an independent prognostic factor in the absence of LN involvement.
Second, the study evaluated the effect of initial treatment on clinically relevant outcome. Nowadays, the concept of risk re-stratification six to eight months after initial treatment is applied in daily practice. Nevertheless, clinicians remain concerned about the risk of recurrence in a pT3 group presenting by definition with high-risk features, since cumulative risk of ETI and LN metastasis rose with increasing primary tumor size (4). Depending on their status at six to eight months (remission or not), at this point in time the study investigated whether the prognostic factors associated with DFS had changed. The risk of events after re-stratification was evaluated in each group of pT3 patients in order to identify and distinguish between those needing aggressive management and a closer follow-up and those who were progressing favorably.
Subjects and Methods
Patients
Of the 4422 patients with differentiated thyroid cancer (DTC) who were initially treated and followed up at the Department of Nuclear Medicine of the Groupe Hospitalier Pitié-Salpêtrière from 1975 to 2014, 566 (12.7%) presented with pT3 PTC. Patient information was obtained from a database and from their medical, surgical, and pathological records. Based on the 2010 revised pTNM classification, all cases of histologically confirmed pT3 PTC were included. For PTC diagnosed before 2002, the histological reclassification was based on the reading of the pathological reports. Data collection from the clinical medical charts of this retrospective study was authorized by the Institutional Review Board of the Biostatistics and Public Health Department of the Groupe Hospitalier Pitié Salpêtrière.
The following variables were analyzed: age at primary tumor diagnosis, sex, complete initial surgery (total or subtotal thyroidectomy; LN dissection), tumor size, invasion of the initial tumor (multifocality, ETI, and vascular invasion), initial LN metastases (presence, location, and LN extracapsular involvement), initial radioiodine therapy, and radioiodine activity.
The pT3 series was artificially split into three groups according to tumor size and the presence of ETI: group 1 (n = 160), pT3 ≤ 10 mm with ETI (micro pT3 carcinomas); group 2 (n = 328), pT3 > 10 mm with ETI; and group 3 (n = 78), pT3 due to a tumor size >4 cm without ETI. Patients presenting with pT3 N0/Nx PTC were also analyzed to evaluate the impact of ETI on prognosis.
Initial treatment and follow-up
Patient follow-up data were obtained from the database, medical records, and periodic correspondence with patients or their referring physicians. Initial treatment of PTC included total or near-total thyroidectomy (for 529 and 37 patients, respectively) and LN surgery (modified radical LN dissection in 330 patients, limited LN excision in 133 patients), completed by an ablative 131I dose of 100 mCi after surgery (566 patients; M 102 ± 13 mCi). For many years, radioiodine ablation was based on the result of the diagnostic whole-body scan (WBS) performed six weeks after surgery. For the past two decades, indication for RAI ablation has been discussed at multidisciplinary staff meetings at the authors' hospital, according to the international guidelines. All patients were thereafter subjected to levothyroxine treatment at a suppressive dose.
Many changes were made regarding the follow-up of patients with DTC during the period of the study. Since 1995, ultrasonography (US) and, where necessary, fine-needle aspiration biopsy have been performed before radioiodine ablation, thus replacing the pre-radioiodine WBS diagnostic tool, and are included in the follow-up in combination with thyroglobulin (Tg) measurements. Nowadays, the follow-up protocol consists of a first appointment six to eight months after the first therapy in order to assess the efficacy of thyroid remnant ablation. This appointment is based on clinical examination, recombinant human thyrotropin (rhTSH)-stimulated serum Tg-level measurement, assay for anti-Tg antibodies, and neck ultrasonography. A diagnostic WBS is no longer performed systematically. According to their clinical status, patients were re-stratified as follows: clinical remission (normal clinical examination, undetectable Tg level and normal US) or with persistent disease (suspicious Tg level, abnormal US or WBS when performed). Patients in the first group were moved to the long-term follow-up group; patients in the second group were followed with the appropriate imaging or diagnostic technique (US-guided fine-needle aspiration biopsy, chest X-ray, 18-fluorodeoxyglucose-positron emission tomography, computed tomography, magnetic resonance imaging) and treatment if indicated. Data regarding the six- to eight-month checkup were available for 496/566 patients.
Definition and diagnosis of event
An event was defined as: • A locoregional recurrence (LRR) defined as a thyroid bed, soft tissue, or cervical LN recurrence of an initially treated PTC. LRR was detected by clinical examination, 131I positive uptake in the cervical area, or abnormal features at US, and was confirmed by fine-needle aspiration biopsy and histological analysis at surgery. • An elevated blood Tg level that required the administration of a second radioiodine treatment. • The occurrence of a distant metastasis detected by iodine uptake or imaging technique.
Statistical analysis
The descriptive statistics used numbers and percentages for qualitative variables, means ± standard deviation, or median (min – max) for quantitative ones, and survival rates ± standard error at 5, 10, and 15 years for censored data.
Clinicopathologic variables between the three groups were compared using unbalanced analyses of variance followed by Tukey tests for pair-wised comparisons for quantitative variables and chi-square tests or Fisher's exact test for qualitative ones.
Patients with distant metastases at diagnosis were excluded from survival and recurrence analysis. DFS was defined as the time between thyroidectomy and the first event, as defined above. DFS was analyzed in the framework of survival analysis, with the time of the last follow-up among the patients with no event history considered as a censoring time. Estimation of DFS rates was based on the Kaplan–Meier method.
The determination of DFS prognostic factors was carried out in two stages. First, a univariate analysis was performed using univariate Cox models for quantitative variables and log-rank tests for qualitative ones. Following this, a Cox model was estimated by forward stepwise regression. The variables with a univariate p-value <0.10 were entered in the stepwise regression, and those with a p-value <0.05 with the Wald test were retained in the final model. Tumor size and ETI were not included individually in the univariate analysis, as these two parameters are used to define the three pT3 groups.
The six-month status was found to be a very significant prognostic factor. Thus, in order to redefine the prognosis at six months, a new Cox model was estimated with the same methodology as the initial one, but with the initial time shifted to six months.
All computations were performed using the SAS v9.3 statistical package.
Results
Characteristics of pT3 subgroups of patients at initial presentation
The characteristics of pT3 subgroups of patients at initial presentation are shown in Table 1. No significant difference was found in the three groups regarding sex, rate of thyroidectomy, or initial distant metastases.
ETI, extrathyroidal invasion; LN, lymph node; N.S., not significant.
Not surprisingly, group 2 patients (pT3 >10 mm with ETI) presented more frequently with LN metastases (18.6% N1a, 37.8% N1b) and with extranodal extension (21.6%), and the rate of LN dissection was significantly higher in this group than in the other groups. LN metastases and multifocality were more frequent in group 1 (micro pT3) than they were in group 3 (>4 cm without ETI). In addition, group 3 had received a significantly higher activity of 131I than group 2 had, but this was of no relevant clinical significance.
DFS and prognostic factors for recurrence
The DFS rate of patients at 5, 10, and 15 years was 78%, 75%, and 72%, respectively, with a mean DFS of 114 ± 2.3 months. The DFS according to the pT3 subgroups is shown in Figure 1A. DFS at 10 years was 89%, 67%, and 82% in groups 1, 2, and 3, respectively (p < 0.0001; Fig. 1A). Regarding initial LN status, 10-year DFS was 59% in N1b patients, 70% in N1a patients, and 84% in N0-Nx patients (p < 0.0001; Fig. 1B).

Time to event stratified by the three pT3 subgroups or by the lymph node status. (
At univariate analysis, factors that significantly worsen the DFS are: male sex (p = 0.0007), pT3 with ETI >10 mm (group 2; p < 0.0001), multifocality (p = 0.04), N1b LN status (p < 0.0001), presence of an extracapsular LN involvement (p < 0.0001), and having persistent disease at the six- to eight-month checkup (p < 0.0001; Table 2). Age was not significantly associated with DFS in univariate analysis. A trend, albeit not a significant one (p = 0.1), was found of a worse prognosis for patients diagnosed before 1990. However, this group only included 33 patients. Considering the median year of initial diagnosis (i.e., 2004), no significant difference was found in the outcome of patients diagnosed with PTC during or before 2004 in comparison to those diagnosed after 2004. Tumor size and ETI were not included individually in the univariate analysis, as both these parameters were used to define the three pT3 groups.
DFS, disease-free survival; HR, hazard ratio; CI, confidence interval.
In the multivariate analysis (Table 2), male sex (p = 0.002), pT3 >10 mm with ETI (group 2; p = 0.001), and LN involvement (p < 0.0001), especially in the lateral compartment (N1b), still have a negative influence on DFS.
To go a step further, the outcomes of pT3 N0/Nx PTC patients were analyzed in order to evaluate whether ETI is an independent prognostic factor in the absence of LN involvement. As shown in Table 3 and Figure 2, a trend toward a worse prognosis for patients with pT3 N0/Nx PTC >10 mm with ETI was found in comparison with the other pT3 N0/Nx patients, but this was not statistically significant. Factors significantly associated with the DFS in univariate analysis of pT3 N0/Nx patients were age (p = 0.02) and “status at six months” (cured vs. persistent disease; p < 0.0001). On multivariate analysis, only “status at six months” remained significant (p < 0.0001).
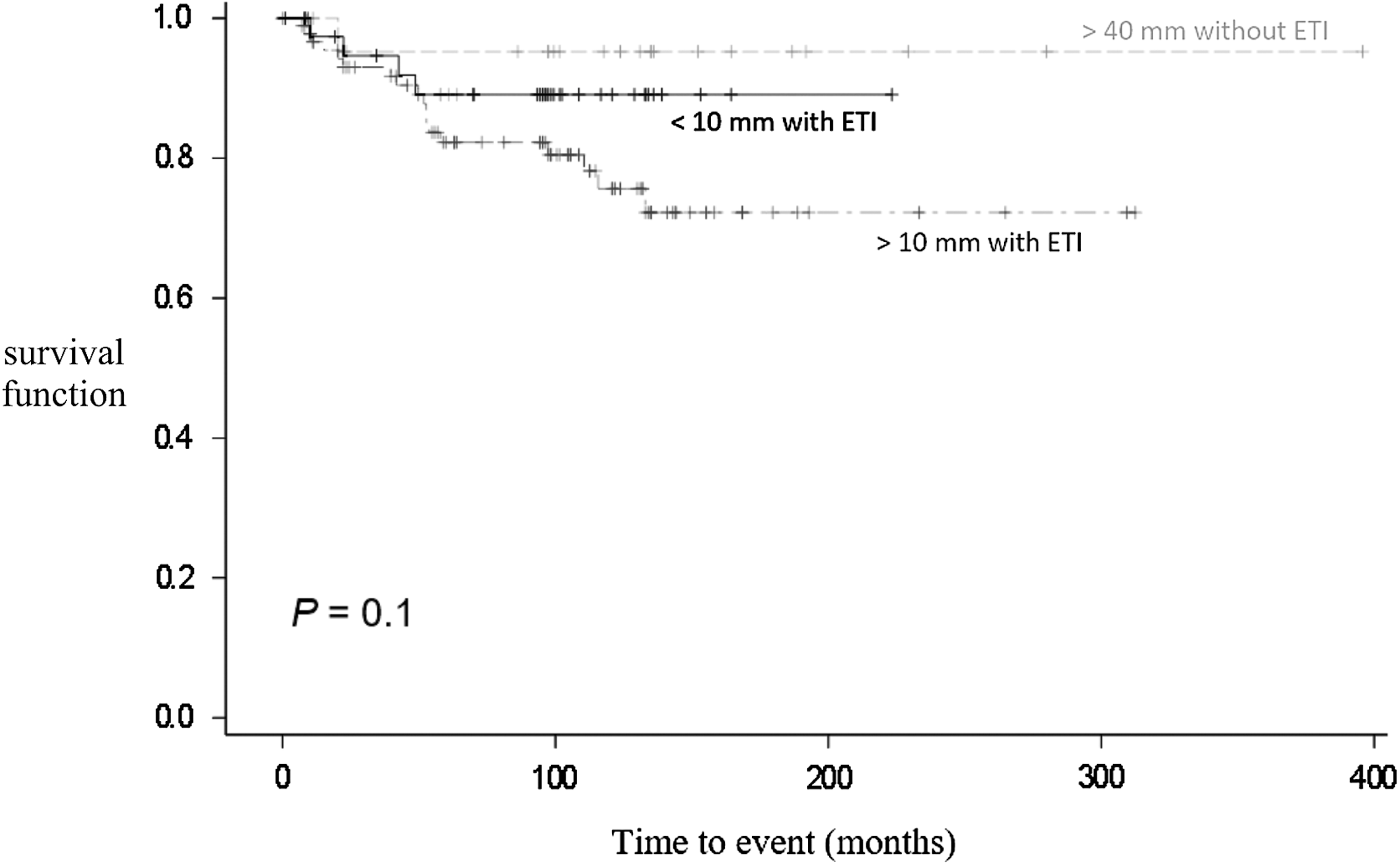
Time to event for patients with pT3N0/Nx papillary thyroid carcinoma according to the pT3 subgroup: group 1 (black line), group 2 (dark gray line), and group 3 (light gray line).
Description of disease-related events and outcome after the six- to eight-month checkup
In this study, the median follow-up was 6.6 years (range 1.9–9.2 years). During follow-up, 106 (18.7%) events were observed: 12 (7.5%) in group 1, 82 (25%) in group 2, and 12 (15.3%) in group 3.
Histological reports of such recurrent patients were reviewed: nonaggressive variants were identified in 91 (85.8%) cases, and 15 (14.24%) aggressive variants (six diffuse sclerosing variant, five tall-cell variant, two Hürthle cell variant, and two minor poorly differentiated component).
Most events were LRR (n = 77; 13.6%) as follows: nine in group 1, 63 in group 2, and five in group 3. Among the series, 10 patients had isolated and repeatedly elevated serum Tg levels that justified the administration of a second therapeutic dose of 131I, and eight patients developed distance metastases during follow-up (mediastinal metastases in one case and lung metastases in seven cases).
At the end point, 486 (85.9%) patients were cured, 19 (3.3%) patients had progressive disease, 55 (9.7%) patients had stable disease, and six (1.1%) patients were lost to follow-up. Sixteen (2.8%) patients died—six from their thyroid cancer, seven from another cause, and three from an unknown cause of death.
Six to eight months after initial treatment, 389/496 (78.4%) patients were in clinical remission and 107 (21.6%) had persistent disease (60 biochemical disease, 12 morphological disease, 35 biochemical and morphological disease).
In patients cured at the six- to eight-month checkup, 10-year DFS improved significantly in each group, from 89% to 98% in group 1, from 67% to 96% in group 2, and from 82% to 90.5% in group 3, with a low probability of event (Table 4) in comparison with uncured patients.
NA, not available.
In contrast, none of the patients re-stratified as having persistent disease in group 1 were disease free (Table 4). In group 2, 10-year DFS decreased to 19% in patients re-stratified as having persistent disease and to 57% in group 3, with a higher probability of events in comparison with the cured group (Table 4).
In patients in clinical remission at the six- to eight-month checkup, LN involvement had no significant impact on DFS (Fig. 3A; p = 0.6) on multivariate analysis. In patients with persistent disease at six to eight months, initial LN involvement (N1a or N1b) influenced and worsened the prognosis (Fig. 3B; p = 0.001).
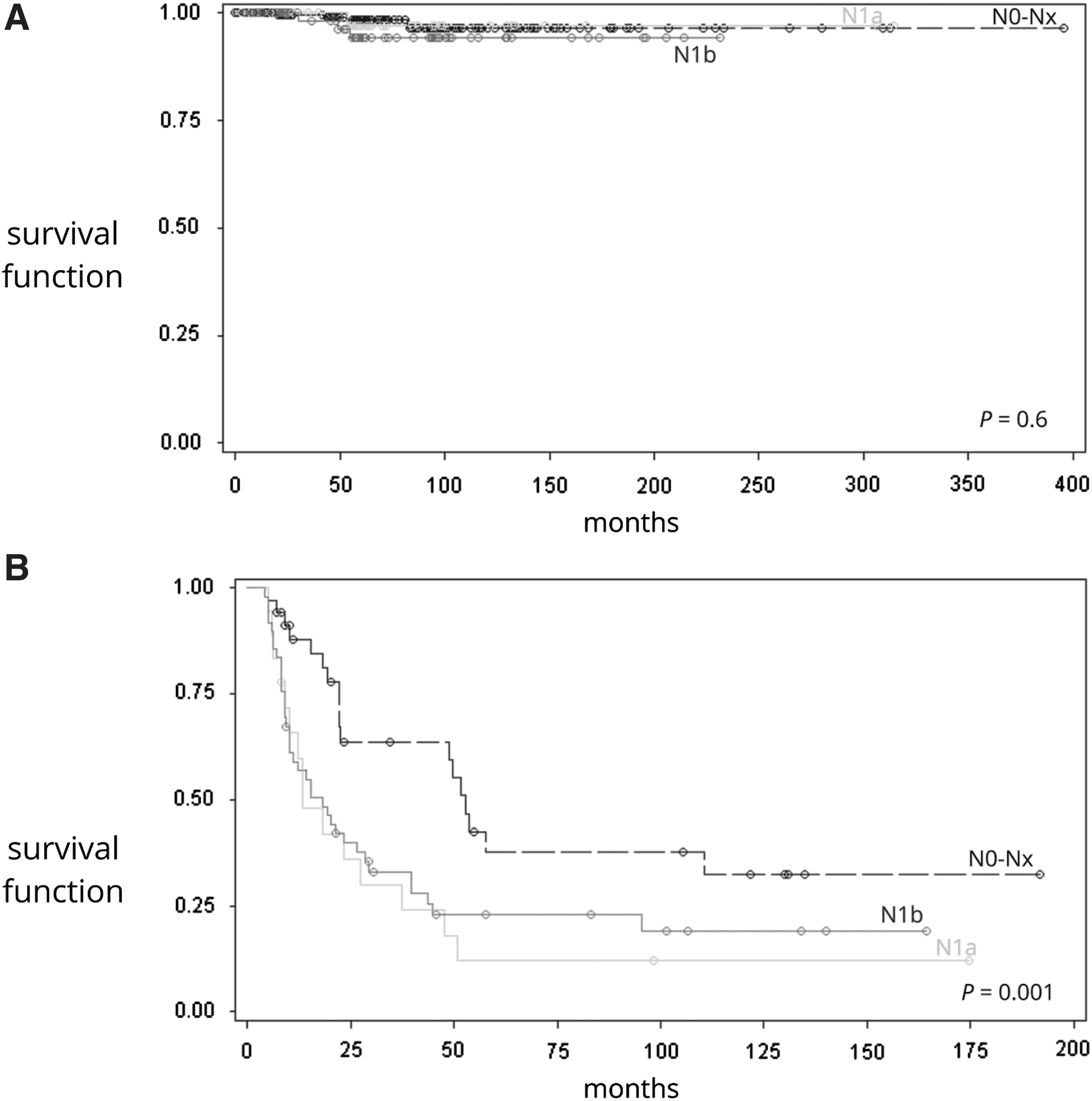
Time to event stratified by the lymph node status: (
Discussion
PTC that fall into the pT3 group of the latest pTNM classification represent a heterogeneous group of carcinomas ranging from large tumors without ETI to small tumors, even those <1 cm, with minimal ETI. There is a growing need to identify prognostic variables that can further refine the risk stratification of these pT3 tumors. First, this study identified three independent factors significantly associated with reduced DFS in the cohort: LN involvement and especially N1b LN status (p < 0.0001, hazard ratio [HR] = 3.4 [confidence interval (CI) 2.2–5.4]), ETI only for tumors >1 cm (i.e., group 2; p = 0.001; HR = 2.6 [CI 1.4–4.8]), and male sex (p = 0.002). In line with previous publications (8,15,16), it is demonstrated that the strongest independent prognostic factor significantly associated with reduced DFS (59% at 10 years) in multivariate analysis was the N1b status. The data suggest that the location of LN metastases should be taken into account in the ATA risk-stratification system. N1b PTC patients, including those with limited LN involvement, may be included in the intermediate-risk category. pT3 patients were divided into three groups in an attempt to evaluate more accurately the role of both the size of the tumor and ETI in the recurrence risk of a pT3 PTC cohort. It was found that there is a continuum of risk with group 1 (i.e., tumors ≤1 cm with ETI) having a better 10-year DFS (89%) than group 3 (i.e., large tumors >4 cm without ETI; 82%), which in turn is better than in group 2 (i.e., tumors >10 mm with ETI; 67%). Intrathyroidal tumors, even those large in size, have a good outcome, in accordance with previous literature (17) and the 2009 and 2015 ATA risk stratification system where they are included in the low-risk category. Their low-recurrence risk supports the de-escalation in radioiodine therapy recommended in the latest 2015 ATA guidelines for these tumors, as well as a decrease in the intensity and frequency of follow-up. However, the retrospective, nonrandomized nature of this study and the radioiodine ablation performed in virtually all patients are two limitations that prevent any definite conclusion from being drawn. The good prognosis for the tumors that fall into group 3 can be explained by the high prevalence of a noninvasive encapsulated follicular-variant of PTC (NIFTP), which accounts for 49% of group 3 in this series. Indeed, this variant has been proved to be extremely indolent, provided that there is no vascular invasion in conjunction with its molecular profile, which closely resembles that of the follicular adenoma group of tumors (18 –22). Moreover, among the 106 patients who recurred, none had a NIFTP.
In this study, microcarcinomas with ETI have an excellent outcome. This is consistent with the literature (7,13,14,23), and it was previously demonstrated that the outcomes of the micropT3 N0-x patients were similar to those of the low-risk PTC patients (pT2 N0-x) (15). The findings suggest that the upstaging of conventional microcarcinomas with minimal ETI to the pT3 category of the latest pTNM classification or to the ATA intermediate risk category is disputable.
The worse prognosis in patients that fall into group 2 (i.e., tumors >10 mm with ETI) in comparison with the other groups can probably be accounted for by the significantly higher frequency of LN involvement in this subgroup (see Table 1). A decision was therefore made to focus on pT3 N0/Nx patients so as not to include the effect of LN involvement and to study whether ETI is an independent prognostic factor in that setting, thereby addressing a very important clinical issue. The results suggest that the worse prognosis in patients that fall into group 2 can probably be accounted for by the frequent metastatic LN involvement. However, it could also be explained by ETI, given the trend toward a worse prognosis in pT3 N0/Nx patients with PTC >10 mm, despite the lack of statistical significance.
As expected, the study has demonstrated that male sex is associated with worse overall and DFS, as in most but not all studies (24 –30).
Second, the study supports the relevance of the concept of “ongoing risk stratification” proposed by Castagna et al. (31) and Tuttle et al. (32), which integrates the initial risk-stratification system with the clinical, biochemical, and morphological data available during follow-up. It was found that in the 390 patients with a normal six- to eight-month checkup, the 10-year DFS improved from 89% to 98%, 67% to 96%, and 82% to 91% in groups 1, 2, and 3, respectively. As expected, among the patients not cured by initial treatment, those with LN metastases (N1a or N1b) had a worse prognosis than those with N0-Nx PTC.
Interestingly, in patients with a complete response to initial therapy, LN involvement no longer affected DFS in multivariate analysis. This result is in accordance with Bardet et al. who demonstrated that microscopic N1, meaning small LN metastasis not diagnosed pre- or perioperatively, do not independently predict persistent disease at the last visit (33). Similarly, in N1 PTC patients, a normal postoperative cervical ultrasound combined with a RAI-Tg value <10 μg/L conferred a five-year cumulative incidence risk of recurrence (<6%) comparable with those in the ATA low-risk recurrence group (34). However, in the authors' opinion, the high recurrence risk conferred by the N1b or macroscopic N1 (33,35) status should be taken into consideration before modulating the subsequent follow-up of patients in apparent remission six to eight months after initial treatment.
The main limitation of this study is its retrospective nature. However, the large number of consecutive pT3 PTC patients included in the series, the homogeneous initial management of patients (93.5% of total thyroidectomy and 99.2% of radioiodine ablation), and the follow-up at a single referral institution overcome the potential bias associated with this limitation.
To conclude, this study found that among pT3 PTC patients, those with micro-pT3N0/Nx with ETI or with large tumors >4 cm but without ETI N0/Nx both have excellent outcomes. N1b status remains an independent factor of adverse outcome in pT3 patients. Being in remission six to eight months after initial treatment allows pT3 PTC patients, including those with limited LN involvement at diagnosis, to be reclassified into a low risk of recurrence category.
Footnotes
Author Disclosure Statement
The authors have nothing to disclose.