
Abstract
Background:
Thyroid autoimmunity is a major risk factor for gestational thyroid disease, and recently various other risk factors have been identified, including maternal age, body mass index (BMI) and parity. Human chorionic gonadotropin (hCG) is an important determinant of gestational thyroid function, yet it is unknown to what extent differences in hCG concentration affect the risk for thyroid disease. We have recently shown that thyroperoxidase antibody positivity impairs the thyroidal response to hCG stimulation, which may suggest that this is a mechanism through which thyroid autoimmunity acts as a risk factor for thyroid disease.
Objective:
The purpose of this study is to determine whether hCG is a risk factor for thyroid disease entities and whether recently identified risk factors for thyroid disease may influence the thyroidal response to hCG stimulation.
Methods:
Human chorionic gonadotropin, thyrotropin (TSH), and free thyroxine (FT4) were measured in 5435 pregnant women participating in a prospective cohort. The association of hCG with thyroid disease entities, and the association of known risk factors with thyroidal response to hCG stimulation were studied using multivariable linear regression models.
Results:
Higher hCG concentrations were associated with a higher risk of subclinical and overt hyperthyroidism. Lower hCG concentrations were associated with a higher risk of hypothyroxinemia. In contrast, hCG concentrations were not associated with subclinical hypothyroidism. Further analyses showed that in women with hypothyroxinemia, high hCG concentrations still suppressed TSH. However, in women with subclinical hypothyroidism, high hCG concentrations were not associated with higher FT4. Higher BMI, male fetal sex, and maternal parity >2 were associated with a lower thyroidal response to hCG stimulation.
Conclusions:
Human chorionic gonadotropin is associated with the risk of (subclinical) hyperthyroidism and hypothyroxinemia, but not with the risk of (subclinical) hypothyroidism. Women with hypothyroxinemia have a normal response to thyroidal stimulation by hCG, but this was abnormal in women with subclinical hypothyroidism. Known risk factors for thyroid dysfunction (BMI and parity), and also male fetal sex, are associated with a lower thyroidal response to hCG stimulation.
Introduction
H
Overt thyroid disease is a well-known risk factor for various adverse pregnancy and/or child outcomes (9 –11). Although a fast growing body of evidence now suggests that milder forms, such as subclinical hypothyroidism and hypothyroxinemia, also increase the risk of adverse outcomes, the underlying pathogenic mechanism for these disease entities remains to be elucidated (9,12). Since thyroid disease entities are defined by the absolute levels of TSH and FT4 concentrations, it is important to note that any determinant of thyroid function can be considered a risk factor for thyroid dysfunction. Thyroid autoimmunity, in most studies reflected by thyroperoxidase antibody (TPOAb) positivity, is the most important risk factor for thyroid disease (13). However, recent studies indicate that other characteristics such as maternal body mass index (BMI), age, smoking, parity, ethnicity, and urinary iodine excretion are also risk factors for thyroid disease during pregnancy (14 –20). Although it is well known that hCG is an important stimulator of thyroid function during pregnancy, it is currently unknown if, and to what extent, the hCG concentration at time of blood sampling is a risk factor for thyroid disease (1,2,21).
In addition, both low and high hCG concentrations are associated with adverse outcomes that have also been associated with an abnormal thyroid function (22 –26). Therefore, it is possible that abnormal hCG concentrations underlie the association of thyroid function with adverse outcomes, or abnormal hCG concentrations subsequently cause thyroid dysfunction which may mediate the adverse effects.
We have previously shown that TPOAb positivity is associated with a severely impaired thyroidal response to hCG stimulation (27). This suggests that an impaired response to hCG stimulation may be a mechanism through which thyroid autoimmunity increases the risk of thyroid dysfunction during pregnancy. However, it is unknown to what extent other risk factors may attenuate the thyroidal response to hCG stimulation and whether this is a relevant mechanism through which these risk factors increase the risk of thyroid disease during pregnancy.
This study aims to identify to what extent the hCG concentration at blood sampling is a risk factor for thyroid disease, and also, whether more recently identified risk factors for thyroid disease during pregnancy may impair the thyroidal response to hCG stimulation.
Materials and Methods
Design
This study was embedded in the Generation R Study, a population-based prospective cohort from early fetal life onward in Rotterdam, The Netherlands (28). hCG and TSH, FT4 or TPOAb measurements were available for 5707 pregnant women. Women with twin pregnancies (n = 128), preexisting thyroid disease (n = 73), thyroid (interfering) medication usage (n = 4), or fertility treatment (n = 67) were excluded. The general design, all research aims, and the specific measurements in the Generation R Study have been approved by the Medical Ethical Committee of the Erasmus Medical Center, Rotterdam, and written informed consent was available for all participants (28).
Biochemical measurements
Maternal serum samples were obtained in early pregnancy (median 13.2 weeks; range 9.6–17.6). Plain tubes were centrifuged and serum was stored at −80°C. TSH and FT4 were determined in maternal serum samples using chemiluminescence assays (Vitros ECI; Ortho Clinical Diagnostics, Rochester, NY). The intra- and interassay coefficients of variation were <4.1% for TSH at a range of 3.97–22.7 mU/L and <5.4% for FT4 at a range of 14.3–25.0 pmol/L. TPOAbs were measured using the Phadia 250 immunoassay (Phadia AB, Uppsala, Sweden). TPOAb concentrations were regarded as positive if >60 IU/mL. Euthyroidism and thyroid disease entities were defined according to predefined population-based cutoff values using the 2.5th and 97.5th percentiles in TPOAb negative women (29). Additionally, in order to achieve adequate statistical power, overt hypothyroidism was also defined by the 5th–95th percentile cutoffs (assuming a similar effect estimate as for the proportion of women with overt hyperthyroidism above versus below the hCG median, n = 50 women with overt hypothyroidism would be required to achieve alpha = 0.05 and power = 80%).
Human chorionic gonadotropin was analyzed in serum using a solid-phase, two-site chemiluminescent immunometric assay, calibrated against World Health Organization Third International Standard 75/537, on an Immulite 2000 XPi system (Siemens Healthcare Diagnostics, Deerfield, IL). The Siemens assay measures total hCG and detects serum hCG, hyperglycosylated hCG, serum nicked hCG, serum nicked hCG missing the β-subunit C-terminal peptide, serum nicked hyperglycosylated hCG, serum asialo hCG, serum hCG-β, and serum nicked hCG β (30). The inter-assay coefficient of variation was 8.0, 6.3 and 5.1% at the concentration of 9.7, 53.1 and 821.5 IU/L, respectively (3). Iodine and creatinine were measured in spot urine samples of a subset of women (n = 1986) in samples collected at the same time as serum. The urinary iodine/creatinine ratio was calculated and used for analyses, further details have been described elsewhere (31). As we determined previously, this study population is iodine sufficient (31).
Based on the literature and data availability, we selected known risk factors for thyroid disease or determinants of hCG as potential determinants of the thyroidal response to hCG stimulation. These included maternal age, BMI, smoking, ethnicity, parity, fetal sex, and urinary iodine excretion (3,14 –20). Information on maternal age, smoking status, and ethnicity was obtained by questionnaires during pregnancy. Ethnicity was determined by country of origin and was defined according to the classification of Statistics Netherlands (28). Ethnicity was categorized according to the four major ethnic groups in the Netherlands (Dutch, Moroccan, Turkish and Surinamese) and a Western or non-Western group, details on which have been described previously (18). Maternal smoking status was classified as no smoking, smoking until known pregnancy, and continued smoking during pregnancy. Weight and length were measured at intake (same time as blood sample collection) and were used to calculate BMI. We have previously shown that TPOAb-positive women have a severely impaired thyroidal response to hCG stimulation (27). Therefore, TPOAb-positive women were excluded from analyses on the course of hCG, FT4, and TSH and also on analyses on determinants of hCG-mediated thyroid stimulation. In addition, we have previously shown that placental angiogenic factors (soluble FMS-like tyrosine kinase [sFlt1] and placental growth factor [PlGF]) are determinants of maternal thyroid function during pregnancy and therefore we also additionally adjusted analyses for these factors (32).
Covariates
Information on maternal education level was obtained by questionnaires during pregnancy and was defined as low (none/primary), middle (secondary), or high (higher education). Information on fertility treatment and the sex of the child were obtained from community midwives, obstetricians, and hospital registries.
Statistical analysis
To fulfill model assumptions and acquire optimal fit of regression models, TSH and FT4 concentrations were log transformed and models were fitted using restricted cubic splines with three or four knots. The course of hCG, TSH, and FT4 during early pregnancy was plotted by calculating the median concentrations per week of pregnancy. The association of hCG with the risk of thyroid disease entities was investigated using multivariable logistic regression models. We investigated determinants of hCG mediated thyroid stimulation by using multivariable linear regression models with a product interaction term of each variable of interest with hCG. Due to known constraints of statistical power for interaction analyses, a p-value <0.15 was considered statistical significant of interaction terms and analyses were subsequently stratified to assess (clinical) relevance. In order to investigate the role of thyroidal hCG stimulation in different disease entities we investigated the association of hCG with FT4 in women with subclinical hypothyroidism and subclinical hyperthyroidism (because opposite to TSH, there is still large variation in FT4 concentrations per definition of the diagnosis), and the association of hCG with TSH in women with hypothyroxinemia (because opposite to FT4, there are still large variations in TSH concentrations per definition of the diagnosis). In order to investigate this, we selected euthyroid TPOAb-negative women (and women with one of the subclinical disease entities) and introduced a product interaction term of the clinical disease entity (as a binary variable) with hCG into the linear regression model.
For covariates with missing data, multiple imputation according to the Markov Chain Monte Carlo method was used. Five imputed data sets were created and pooled for analyses. Smoking, education level, ethnicity, parity, and BMI were added to the model (missing due to nonresponse/nonrecording in 13.1%, 7.2%, 4.1%, and <1.0%, respectively). Furthermore, we added hCG, TSH, FT4, and TPOAb concentrations, gestational age at blood sampling, maternal age, and fetal sex as prediction variables only. No significant differences in descriptive characteristics were found between the original and imputed datasets. For clarity, nulliparous and primiparous were combined into a single category because the slope was similar and figures better displayed associations with three categories. All statistical analyses were performed using Statistical Package of Social Sciences version 20.0 for Windows (SPSS Inc., Chicago, IL) or R statistical software version 3.03 (package rms and visreg) and a p-value <0.05 was considered statistically significant.
Results
The final study population comprised 5435 women who were predominantly nulliparous or primiparous (86.9%), nonsmokers (73.5%), and of Dutch origin (51.6%; Table 1). Compared to euthyroid women, mean BMI was higher in women with subclinical hypothyroidism (+0.63 kg/m2; p = 0.045) and in women with hypothyroxinemia (+2.46 kg/m2; p < 0.001) but not for women with subclinical hyperthyroidism (−0.42 kg/m2; p = 0.39). Median hCG concentrations swiftly increased to peak values around the ninth week and then steadily decreased until the 18th week of pregnancy (Fig. 1A–C). Throughout early pregnancy, the course of median FT4 concentrations mimicked that of hCG concentrations (Fig. 1A, C), while the course of TSH concentrations mirrored the course of hCG concentrations (Fig. 1B, C).
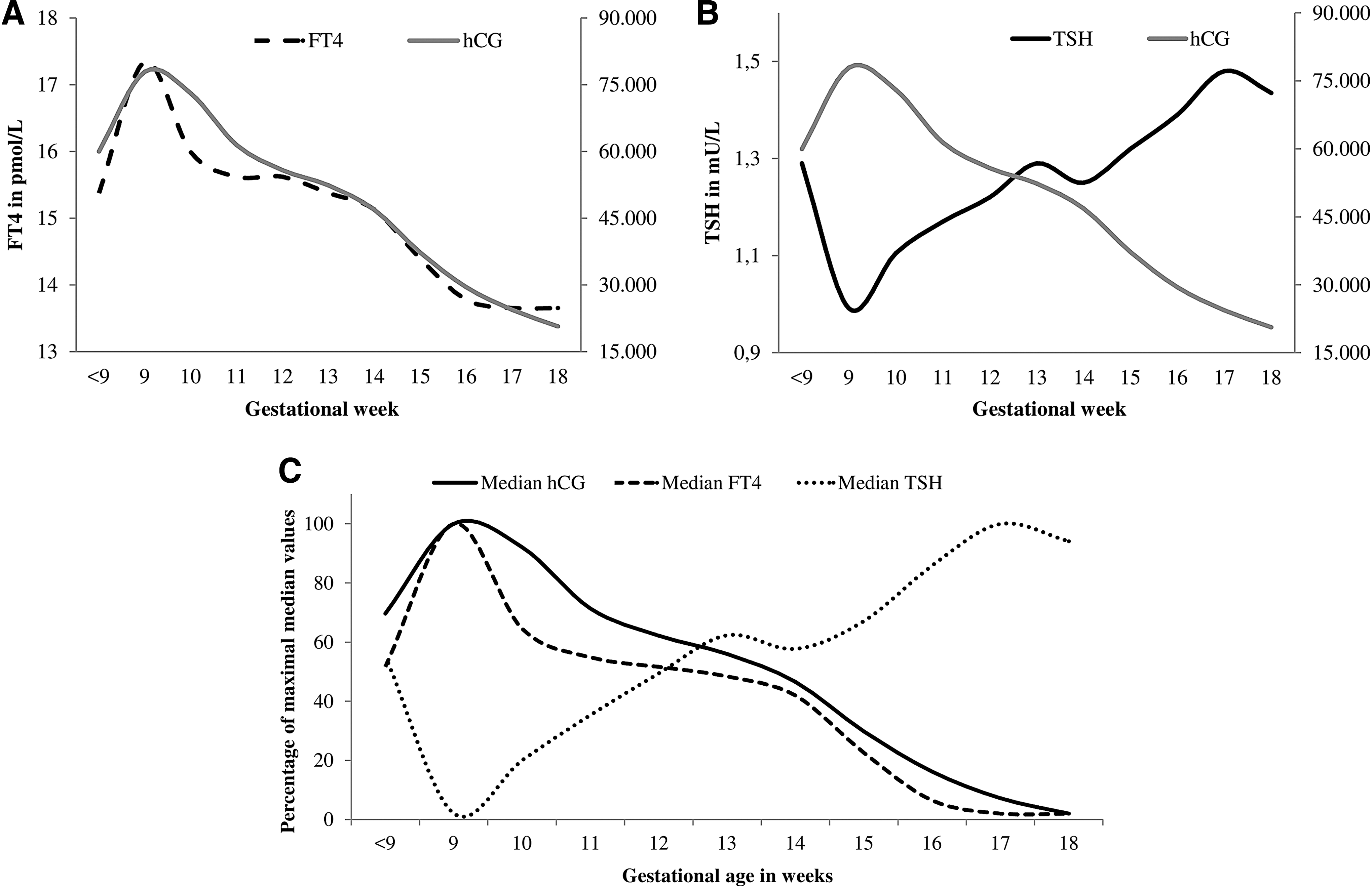
The course of median human chorionic gonadotropin (hCG;
After exclusion of TPOAb–positive women n = 118 (2.3%)
At time of blood sampling; data shown as median in weeks.
Data shown as median in years.
Data shown as n (%).
Data shown after imputation of missing data (13.1% for smoking, 7.2% for education level, 4.1% for ethnicity, and <1.0% for BMI and parity).
BMI, body mass index; hCG, human chorionic gonadotropin; FT4, free thyroxine; T4, thyroxine; TPOAb, thyroperoxidase antibody; TSH, thyrotropin.
The association of hCG concentrations with thyroid disease
There was a positive association of hCG concentrations with subclinical and overt hyperthyroidism (both p < 0.001); Fig. 2C, D). There was a negative association of hCG concentrations with hypothyroxinemia (p < 0.001; Fig. 2B). In contrast, there was no association of hCG concentrations with overt hypothyroidism, also when overt hypothyroidism was defined according to 5th and 95th percentile cutoffs range (n = 19 and n = 54, respectively; p > 0.22; Supplementary Fig. S1A, B; Supplementary Data are available online at

The association of hCG with (subclinical) thyroid disease entities subclinical hypothyroidism (
Because little is known on the mechanisms underlying the biochemical discrepancies of subclinical hypothyroidism and hypothyroxinemia, we subsequently investigated the thyroidal stimulation by hCG within these two groups. We studied the association of hCG concentrations with TSH concentrations in women with hypothyroxinemia, and of hCG concentrations with FT4 concentrations in subclinical hypothyroidism (because the definitions of both disease entities do not allow to study variation of FT4 or TSH respectively) and compared this with euthyroid women. In women with hypothyroxinemia, the association of hCG concentrations with TSH concentrations was similar to euthyroid women (P for difference with euthyroid = 0.72, Fig. 3B). However, in women with subclinical hypothyroidism, the association of hCG concentrations with FT4 concentrations was considerably attenuated compared to euthyroid women (p for difference with euthyroid = 0.047; Fig. 3A). All results remained similar after exclusion of TPOAb positive women (data not shown).
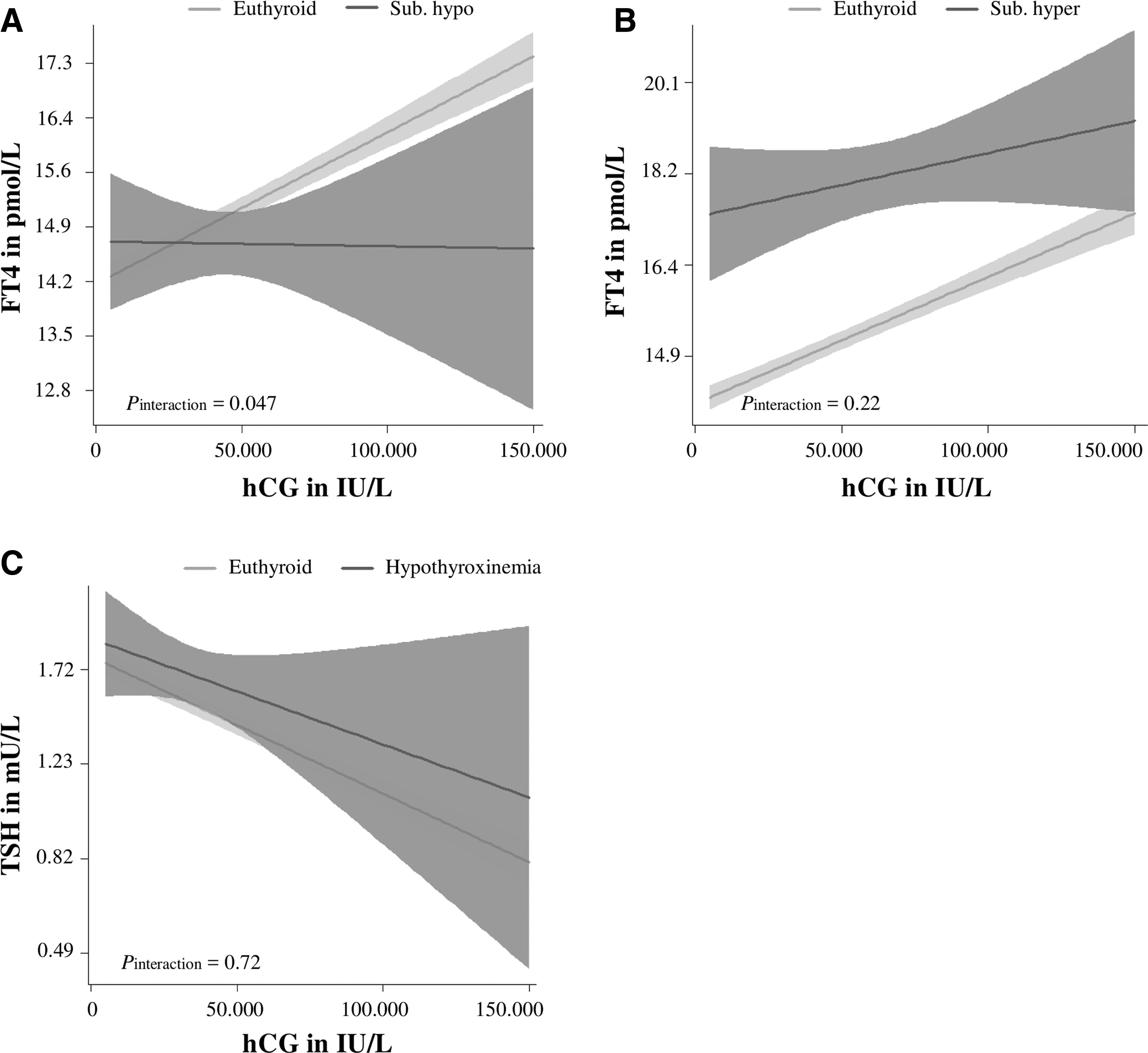
hCG-mediated gestational thyroid stimulation in women with subclinical disease. Figures are shown as estimated mean values (lines) and 95% confidence intervals (colored area) for women with subclinical hypothyroidism (
Thyroidal response to hCG stimulation according to known risk factors
Overall, a higher BMI was associated with higher TSH and lower FT4 concentrations. However, this was amplified at higher hCG concentrations, indicating that a higher BMI was associated with a lower thyroidal response to hCG stimulation (p for difference = 0.003 and 0.068; Fig. 4A, B). Although there were no fetal sex differences in TSH and FT4 at low hCG concentrations, male fetal sex was associated with a lower thyroidal response to hCG stimulation, since women pregnant of a male fetus had higher TSH and lower FT4 concentrations when hCG concentrations were high (p for difference = 0.0064 and 0.0006; Fig. 4C, D). A high parity was associated with a lower thyroidal response to hCG stimulation (p for difference = 0.019 and 0.036; Fig. 4E, F).
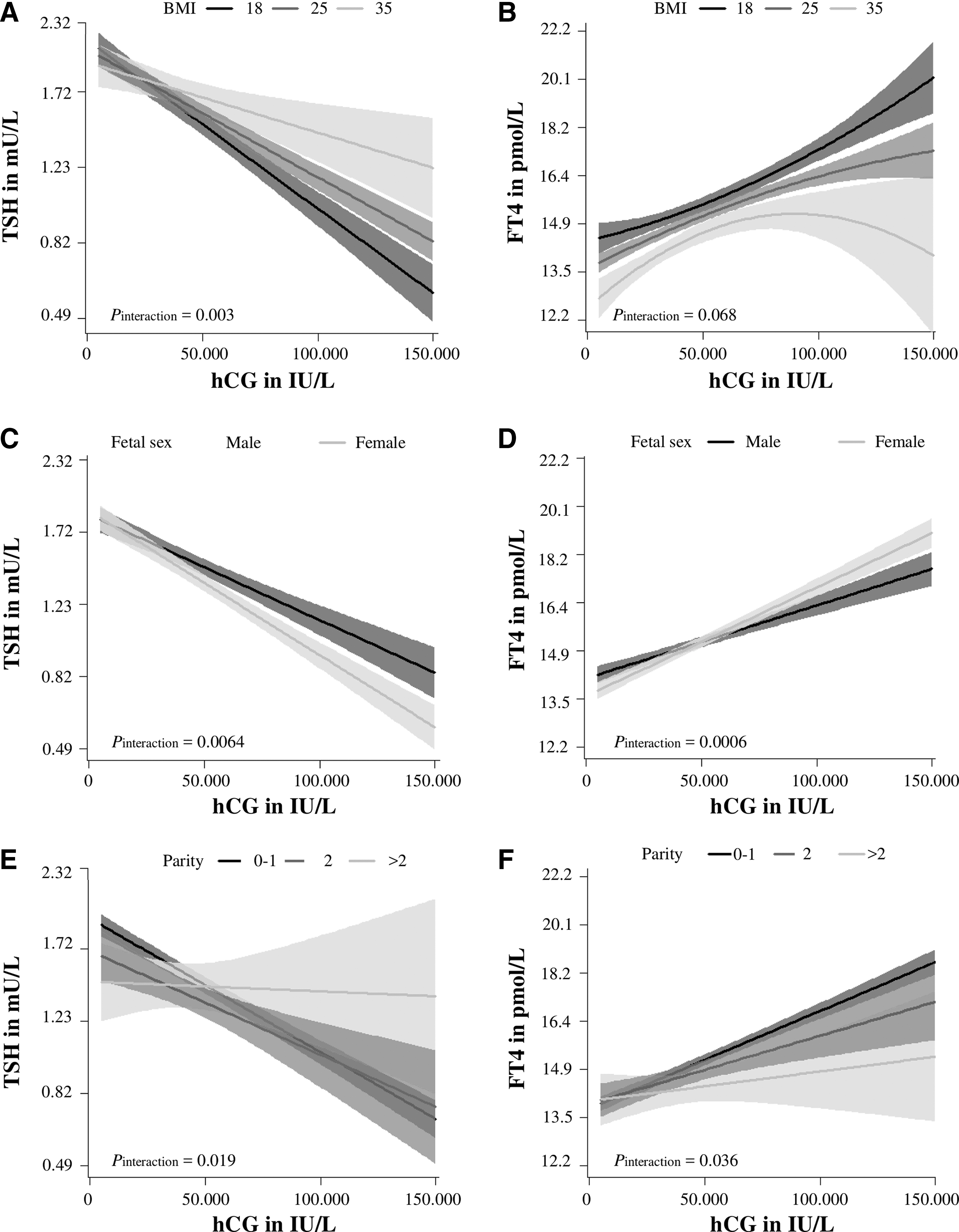
Differences in hCG-mediated gestational thyroid stimulation. Figures are shown as estimated mean values (lines) and 95% confidence intervals (colored area) for women with a body mass index of 18, 25, or 35 kg/m2 (
There were no consistent differences in thyroidal response to hCG stimulation according to maternal ethnicity, age, smoking, or iodine status (data not shown). All results remained similar after additional adjustment for angiogenic factors (sFlt1 and PlGF; data not shown).
Discussion
Since the seminal study by Glinoer et al. (1990) which reported on the association of hCG concentrations with TSH and FT4 concentrations, only few studies have investigated the effects of hCG concentrations on thyroid function during pregnancy (1,2,21). However, accumulating evidence since 1990 has shown that subclinical thyroid disease is associated with a higher risk of adverse pregnancy and child outcomes (8,9). In the current study we identify differences in the association of hCG concentrations with thyroid disease entities. We demonstrate that high hCG concentrations are associated with a lower risk of hypothyroxinemia and a higher risk of subclinical and overt hyperthyroidism, while hCG concentrations are not associated with the risk of overt or subclinical hypothyroidism. In line with these results, we also show that the association of hCG concentrations with thyroid function in women with hypothyroxinemia and subclinical hyperthyroidism is similar that for euthyroid women, while it was considerably attenuated in women with subclinical hypothyroidism. Furthermore, we show that higher BMI, male fetal sex, and parity >2 are associated with a lower thyroidal response to hCG stimulation.
Within a self-proclaimed healthy population, practically all women with the biochemical phenotype of overt hyperthyroidism according to the recommendations of international guidelines will have transient gestational hyperthyroidism, or thyrotoxicosis, due to high hCG concentrations (6 –8,33). In the current study, we show that hCG concentrations are indeed a major determinant of gestational hyperthyroidism. These numbers confirm the current belief that gestational hyperthyroidism should be considered as a mild thyroid function abnormality, unlikely to lead to adverse outcomes or require antithyroid drug treatment (33,34). However, because our results indicate that even very high hCG concentrations do not account for all cases of gestational hyperthyroidism, further studies are warranted to investigate the existence of potential subphenotypes (35).
Hypothyroxinemia is associated with an increased risk of adverse offspring outcomes, in particular neurocognition (36 –39), but the pathogenic mechanism for hypothyroxinemia remains unclear. Although hypothyroxinemia was for long considered as a pregnancy-specific disease entity that reflects a state of mild iodine deficiency, this is challenged by the occurrence of hypothyroxinemia in iodine sufficient areas as well as the lack of (F)T4 increase following iodine supplementation (40 –45). The current study, performed in an iodine sufficient population, is the first study to demonstrate that low hCG concentrations at blood measurement are a risk factor for hypothyroxinemia. These results suggest that hypothyroxinemia in iodine-sufficient areas is caused, at least partially, by low hCG concentrations and confirms that hypothyroxinemia is a pregnancy-specific disease entity. Subsequently, we also show that in women with hypothyroxinemia, the negative association of hCG with TSH is similar to euthyroid women. Given that the association of hCG concentrations with TSH is predominantly mediated via a hCG-mediated increase in FT4 concentrations, this suggests that the functional capacity of the thyroid is not impaired in women with hypothyroxinemia. In other words, it is likely that a pregnancy-specific increase in FT4 concentrations in hypothyroxinemic women is similar to euthyroid women. These findings may add to the scientific debate on the cause of hypothyroxinemia. In addition, it can be speculated that women with hypothyroxinemia are more sensitive to thyroid hormone at the level of the hypothalamus and/or the pituitary, and that this adds to their biochemical phenotype of low FT4 with high TSH concentrations. Further studies are needed to investigate non-gestational thyroid function of women with hypothyroxinemia during pregnancy and the effects of hCG in populations with (moderately) deficient iodine status.
This is the first study to demonstrate that serum hCG concentration are not associated with the risk of subclinical hypothyroidism, suggesting a lack of thyroidal response to hCG stimulation in women with subclinical hypothyroidism during pregnancy. In women with a lower thyroid functional capacity, the hCG-mediated increase in FT4 concentrations may be impaired, which may lead to a lack of decrease in TSH concentrations during pregnancy. This is also supported by our finding that high hCG concentrations were not associated with higher FT4 concentrations within the group of women with subclinical hypothyroidism. On top of the lack of decrease in TSH concentrations, we speculate that women with a lower thyroid functional capacity may already have high-normal TSH concentrations going into pregnancy. Together, this may lead to the biochemical phenotype of subclinical hypothyroidism.
Several factors may contribute to an impaired thyroidal response to hCG. It has been reported that approximately one-third of all women with subclinical hypothyroidism are TPOAb positive (46). We have previously shown that the thyroidal response to hCG stimulation is severely impaired in the majority of TPOAb positive women (27). However, the results in this study all remained similar after exclusion of TPOAb positive women. Although women with subclinical hypothyroidism had a higher mean BMI, women with hypothyroxinemia had an even higher mean BMI but still a hCG mediated FT4 response similar to euthyroid women and all analyses were adjusted to BMI. This suggests that the lower thyroid functional capacity in women with subclinical hypothyroidism is not due to thyroid autoimmunity or a higher BMI. Future studies are needed in order to investigate the underlying cause of a lower thyroid functional capacity in women with subclinical hypothyroidism.
Various studies have shown that a high BMI is associated with higher TSH and lower FT4 concentrations (47). Most likely the effects on TSH are mediated via higher leptin levels, increasing thyrotropin releasing hormone via upregulation of thyrotropin releasing hormone (TRH) gene expression and by increasing the conversion of proTRH to mature TRH (48,49). Additionally, a higher BMI may be associated with lower FT4 through an increase in T4 binding or increased FT4 assay interference, as higher body fat mass is associated with higher thyroxine-binding globulin concentrations (50). We now demonstrate that a higher BMI is also associated with a lower thyroidal response to hCG stimulation, which might suggest that a higher BMI leads to a lower thyroid functional capacity or toward the presence of an underlying factor that is associated with both BMI and the thyroid functional capacity. Based on the results from the current study, gestational FT4 and TSH concentrations in overweight or obese women reflect changes in hCG concentrations than in normal-weight women to a lesser extent.
We show that there are small, but consistent fetal sex specific differences in the thyroidal response to hCG stimulation. Fetal sex-specific differences have been shown for various outcomes including placental gene expression, placentation markers, disease symptomatology, and risk and severity of adverse pregnancy outcomes (51 –53). Although our results might be confounded by fetal sex specific differences in placental angiogenic factors (such as sFlt1 and PlGF) (32,53), additional adjustment for sFlt1 and PlGF did not change the results. Alternatively, as hCG isoforms have a different stimulating potential for the TSH receptor (54 –56), fetal sex specific differences in hCG isoforms could explain fetal-sex specific differences observed in the current study.
Iodine is an important determinant of thyroid function and both low and high urinary iodine to creatinine ratios have been associated with lower thyroid function (20). In this study, we did not find differences in thyroidal response to hCG stimulation between groups with a different iodine status based on urinary iodine to creatinine ratios. However, our cohort is iodine sufficient and therefore we could not properly investigate the difference in thyroidal response to hCG according to low concentrations of iodine.
To our knowledge, this is the first study that investigated the association of differences in hCG concentrations with the risk of (subclinical) disease entities and the thyroidal response to hCG stimulation. We were able to study this in a large, prospective cohort with detailed phenotype data. We were limited by the fact that only a single measurement of hCG and thyroid function tests was available. However, thyroid function measurements are highly correlated throughout pregnancy (57). Furthermore, in clinical practice, decisions are based on the interpretation of a single measurement which mimics the data availability in this study. We were also limited by the relative low number of women with overt hypothyroidism which did not allow for adequately powered analyses. However, an alternative definition for hypothyroidism according to the highest and lowest fifth percentiles did not change the results. In addition, inadequate statistical power may also account for the lack of association between hCG concentrations and subclinical hypothyroidism. However, the number of women with subclinical hypothyroidism was equal or higher than other disease entities, suggesting that the potential effect of hCG concentrations on subclinical hypothyroidism would be much smaller. Another potential limitation is the fact that we were not able to measure the various isoforms of hCG, that may exert a different stimulation of the TSH receptor. However, changes in the ratio of hCG isoforms predominantly occur in the first six weeks of pregnancy, which is well before women were included in this study (58).
In conclusion, we show that hCG concentrations are a determinant of hypothyroxinemia and subclinical or overt hyperthyroidism. hCG concentrations are not a determinant of subclinical hypothyroidism, and women with subclinical hypothyroidism have an impaired FT4 response to hCG stimulation. We demonstrate that some, but not all, risk factors for thyroid disease in pregnancy (higher BMI, parity) as well as male fetal sex are determinants of the thyroidal response to hCG stimulation. These data give novel insights into the (patho)physiology of thyroid disease during pregnancy. Future studies are needed to determine to what extent differences in thyroidal response are associated with adverse pregnancy outcomes or offspring development.
Footnotes
Acknowledgments
The contributions of the endocrine laboratory technicians are highly appreciated. The Generation R study is conducted by the Erasmus Medical Center (Rotterdam) in close collaboration with the School of Law and Faculty of Social Sciences of the Erasmus University, Rotterdam; the Municipal Health Service Rotterdam Area, Rotterdam; the Rotterdam Homecare Foundation, Rotterdam; and the Stichting Trombosedienst and Artsenlaboratorium Rijnmond, Rotterdam. We gratefully acknowledge the contribution of children and parents, general practitioners, hospitals, midwives, and pharmacies in Rotterdam. The general design of the Generation R Study is made possible by financial support from the Erasmus Medical Center, Rotterdam; the Erasmus University Rotterdam; The Netherlands Organization for Health Research and Development; The Netherlands Organisation for Scientific Research; the Ministry of Health, Welfare, and Sport; and the Ministry of Youth and Families.
This work was supported by a clinical fellowship from The Netherlands Organisation for Health Research and Development (ZonMw), project number 90700412 (grant to R.P.P.).
Author Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.