
Abstract
Background:
Medullary thyroid carcinoma (MTC) is a rare disease. Treatment options for recurrent disease are limited. Although somatostatin analogues might have a role as anticancer agents in MTC, the evidence is inconclusive.
Patient Findings:
A 64-year-old male was diagnosed with MTC in January 2010. Total thyroidectomy with neck dissection (stage IVA, pT2pN1bM0, R1) was performed, followed by adjuvant locoregional radiotherapy. Two years later, in January 2012, the patient developed recurrent metastatic disease, evidenced by elevated carcinoembryonic antigen (CEA) and calcitonin levels, and a positive uptake (Octreoscan®) in the right adrenal gland and pancreatic head. A further computed tomography (CT) scan revealed metastases in the right adrenal gland, the duodenal bulb, and two pancreatic lesions, which were later confirmed as metastases by endoscopic ultrasound and cytology, and therefore salvage surgery was ruled out. Treatment with Somatuline Autogel® (120 mg subcutaneously every 28 days) was initiated in September 2012, and 11 months later, calcitonin and CEA levels had both normalized, and a new CT scan showed that the metastatic lesions had disappeared or shrunk markedly. An Octreoscan performed in January 2014 and a repeat contrast-enhanced CT in February 2014 showed sustained tumor response. The patient remained in remission until February 2016, when a new Octreoscan revealed recurrent disease in the right adrenal gland, a nodule in the right upper pulmonary lobe, and nodal disease in the celiac trunk. CEA and calcitonin levels remained normal, although with a slight increase in calcitonin levels (47 pg/mL).
Summary:
The unusual case is described of a patient with metastatic MTC involving the adrenal gland, duodenum, and pancreas, who achieved a sustained response to somatostatin analogues after 11 months of treatment. The patient remained in remission for nearly 3.5 years from initiation of treatment with somatostatin analogues.
Conclusions:
The case presented here is one of the few described in the literature in which long-term treatment with somatostatin analogues resulted in a sustained tumor response in a patient with metastatic recurrent MTC following curative-intent surgery. These findings suggest that prolonged treatment with somatostatin analogues may be beneficial in asymptomatic cases with a low tumor burden and a positive Octreoscan following recurrence. More data are needed to confirm these findings.
Introduction
M
Somatostatin analogues have been shown to have antitumor activity in various types of NETs (5), and it has been suggested that these medications could play a similar role in MTC (6,7). However, of the few studies that have assessed somatostatin analogues in the treatment of MTC, most—with the notable exception of Mahler et al. (6)—have reported either inconclusive results or no significant benefit (8). Importantly, the studies conducted to date are all either small case series or non-systematic trials (ranging from 3 to 22 patients) that have assessed heterogeneous treatment regimens in terms of dose and duration of treatment in diverse patient samples (8). No randomized trials have been conducted. Although most literature reviews (8) and clinical guidelines (3) have concluded that there is insufficient evidence to support the use of these drugs in MTC, several studies (6,7,9) have reported a benefit in some patients. Consequently, at present, the available evidence is inconclusive.
In this context, an unusual case is presented of a patient with metastatic MTC involving the adrenal gland, duodenum, and pancreas, who achieved a sustained response after 11 months of administration of Lanreotide Autogel. The patient remained in remission for more than four years after the initial recurrence and nearly three-and-a-half years from initiation of somatostatin analogue treatment.
Patient
A 64-year-old male patient was diagnosed with MTC in January 2010. After diagnosis, the patient underwent a total thyroidectomy with neck dissection (stage IVA, pT2pN1bM0, R1) followed by adjuvant locoregional radiotherapy. He was negative for a REarranged during Transfection (RET) proto-oncogene germline mutation, but was found to have a somatic RET gene mutation (C611Y). Follow-up was performed according to standard clinical protocols.
In January 2012, two years after his initial diagnosis, elevated calcitonin levels (calcitonin 507 pg/mL) were detected on a routine blood test. A bone scan performed in February was negative for bone metastases, but a contrast-enhanced computed tomography (CT) of the neck, chest, and abdomen in March revealed a suspicious 23 mm nodule in the right adrenal gland (35 Hounsfield units). Although no symptoms of pheochromocytoma were present, a 24 h urine metanephrine (MN) and normetanephrine (NMN) analysis was performed to rule this out, with negative findings. The suspected diagnosis was adrenal metastasis, although no biopsy was performed. A positron emission tomography (PET)-CT scan performed in June showed no evidence of malignancy. However, a subsequent Octreoscan® showed uptake in both the right adrenal gland and pancreatic head, at which time, a diagnosis of recurrent MTC with suspected tumor metastasis was made. This was further confirmed by elevated carcinoembryonic antigen (CEA) levels and higher calcitonin levels (calcitonin 5967 pg/mL), although the patient continued to be asymptomatic.
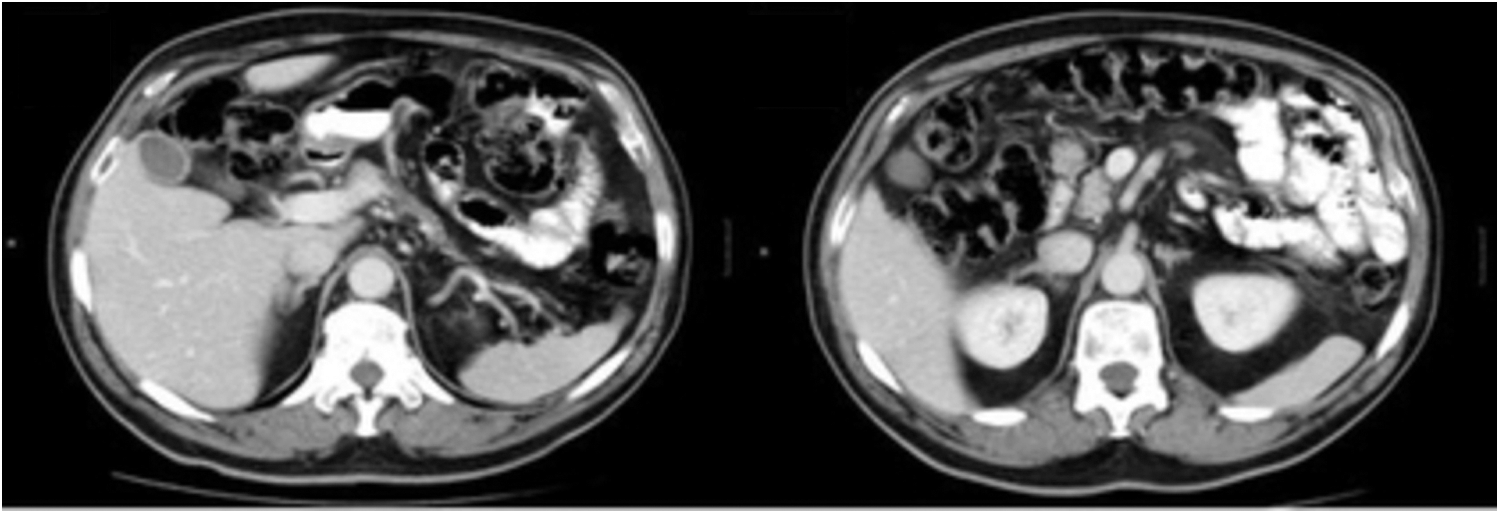
In July 2012, a thoraco-abdominal CT scan revealed several metastases (Fig. 1, from left to right): a right adrenal mass (30 mm × 28 mm), a 24 mm lesion on the lower wall of the duodenal bulb, and two pancreatic lesions of 21 mm (pancreatic body) and 30 mm (uncinate process) in size.

July 2012 computed tomography (CT) scan showing recurrent disease in the pancreas, duodenum, and right adrenal gland.
The multidisciplinary gastrointestinal tumor board ruled out salvage surgery due to the risk associated with surgery of the pancreas and the adrenal lesions, although the presence of a pheochromocytoma was deemed to be unlikely based on the biochemical results. The patient had been consistently asymptomatic since diagnosis, which is why treatment with vandetanib or cabozantinib was not initiated at any point. Given that an Octreoscan was positive for expression of somatostatin receptors in all of the lesions, the decision was made to initiate treatment with Somatuline Autogel® (120 mg subcutaneously [s.c.] every 28 days) in September 2012 (Fig. 2).
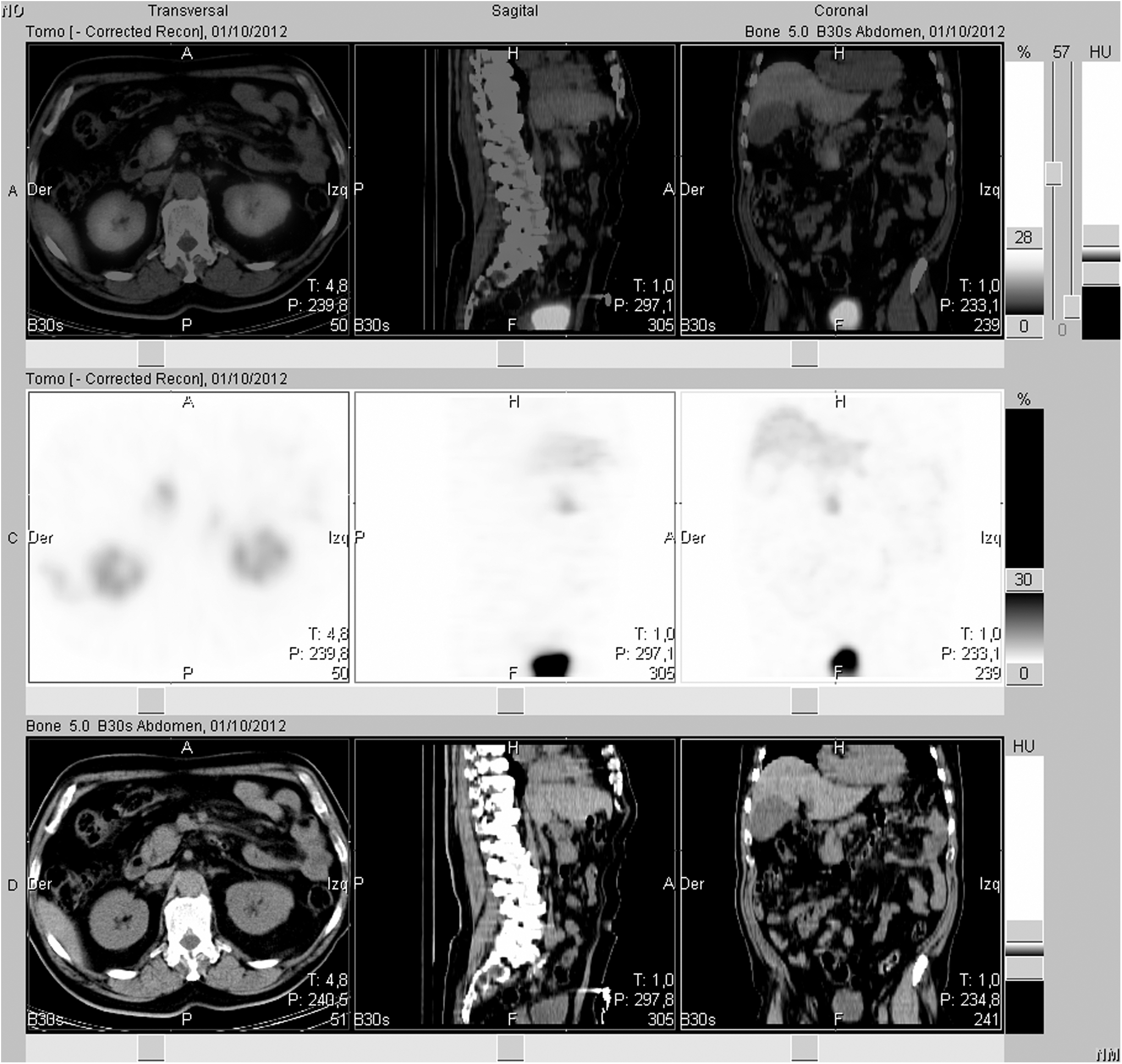
September 2012 Octreoscan® with positive findings in the abdomen.
An endoscopic ultrasound on November 14, 2012, showed a rounded, well-delimited 25 mm lesion at the junction of the pancreatic neck and body. Two other rounded lesions were also seen in the pancreatic head and the uncinate process (30 mm and 8 mm, respectively). Fine-needle aspiration biopsy confirmed metastatic MTC in all three lesions.
A contrast-enhanced CT scan performed in late November revealed a small (<5 mm) lung nodule. In addition, the adrenal mass had increased slightly in size (to 37 mm), while the mass in the pancreatic head showed a suspicious increase in volume. Calcitonin levels were 7253 pg/mL. Nevertheless, the patient remained asymptomatic with an excellent quality of life.
In December 2012, the patient was again presented to the multidisciplinary tumor board, which decided to continue with somatostatin analogue treatment and re-evaluate in three months. A subsequent cervico-thoraco-abdominal CT scan with intravenous contrast in February 2013 showed that the existing masses (lung, adrenal gland, and pancreas) were stable. No evidence of bone metastases was seen. An Octreoscan performed in April confirmed these lesions and detected a new lesion on the posterior arch of the fifth right rib.
In August 2013, 11 months after initiation of treatment with somatostatin analogues, blood tests showed that levels of serum calcitonin and CEA had both normalized (Table 1). Similarly, a contrast-enhanced CT scan (Fig. 3) revealed that the lung nodule was no longer evident, the pancreatic lesions had disappeared, and the right adrenal mass was barely visible, with the only finding being a minimal thickening of the right adrenal gland. An Octreoscan performed in January 2014 (Fig. 4) and a repeat contrast-enhanced CT in February 2014 showed complete tumor response. Another CT scan performed later that year (September 2014) confirmed a persistent complete tumor response, a finding that was reconfirmed in an Octreoscan in November 2014. Analysis for the presence of KRAS and NRAS mutations in the initial diagnostic biopsy revealed wild-type results; HRAS was not analyzed.
August 2013 CT scan showing complete tumor response.

January 2014 Octreoscan showing complete tumor response.
CEA, carcinoembryonic antigen; s.c., subcutaneous.
In April 2015, a contrast-enhanced neck, chest, and abdominal CT scan confirmed a complete, sustained tumor response. In September 2015, the patient was in excellent condition, with good tolerance to somatostatin treatment. As of February 2016, the patient had been taking Somatuline Autogel (120 mg s.c./28 days) for a total of three years and four months. However, a new Octreoscan revealed recurrent disease in the right adrenal gland, a nodule in the right upper pulmonary lobe, and nodal disease at the celiac trunk. Blood tests and CEA levels were both normal, but calcitonin levels had risen slightly (to 47 pg/mL). The patient was completely asymptomatic at the last consultation, and the decision was made to maintain Somatuline Autogel treatment (120 mg s.c./28 days) as monotherapy. Considering that the patient remains asymptomatic, the current treatment plan is to continue with somatostatin analogue treatment until the patient becomes symptomatic or disease progression requires more aggressive treatment.
Discussion
Evidence to support the anticancer effect of somatostatin analogues in MTC is scant, and the data that are available seem to suggest that these medications generally lack effectiveness in MTC (3,6 –9). However, in the case report presented here, a patient is described who achieved a complete response of recurrent MTC with multiple metastases. After 11 months of treatment with Somatuline Autogel, all of the metastatic lesions disappeared. To the authors' knowledge, this is the first such case reported in the literature, and these findings suggest that it may be premature to rule out an anticancer effect of somatostatin analogues definitively in patients with MTC.
At present, clinical guidelines and literature reviews do not recommend treatment with the use of somatostatin analogues for advanced MTC due to the scant evidence for its efficacy, even in patients with positive Octreoscan (3,4,8). Nevertheless, the present case demonstrates the potential effect of these drugs, at least in this single patient. Given the limited treatment options for patients with recurrent metastatic disease, the results presented here cannot be easily disregarded, especially considering the low level of current evidence, which consists of case reports and small case series but does not include randomized controlled studies. For these reasons, and in the context of the findings reported here (admittedly, only a single case report), the jury is still out regarding the potential anticancer effects of somatostatin analogues in patients with MTC.
The first study to report a benefit for these drugs in MTC was published in 1990 (6). In that study, Mahler et al. described three patients with metastatic MTC who received daily treatment with escalating doses of octreotide (1.0, 1.5, or 2.0 mg daily) delivered using a s.c. pump. In two patients (both with MEN2A), calcitonin levels decreased substantially and remained at normal levels for 15 and 17 months, and those two patients also experienced an improvement in symptoms. Unfortunately, those positive results have not been confirmed in subsequent studies. Modigliani et al. (10) found that treatment with octreotide (14 patients) was not associated with a sustained decrease in calcitonin and did not achieve tumor stabilization or regression.
In another small study, Díez et al. (9) evaluated the effects of somatostatin analogues on calcitonin and CEA levels in patients with advanced MTC. In that study, five patients with postoperative recurrent MTC were treated with somatostatin analogues for 12 weeks. One patient with very advanced disease died shortly after the start of treatment. Of the other four patients, one responded well to therapy (normalization of calcitonin and CEA levels), but no clinically relevant changes (calcitonin or CEA levels) were observed in the other three patients. However, it is worth mentioning that positive uptake detected prior to treatment was not detectable post treatment in one patient. Overall, although improvement was noted in a few patients, this was not sustained at 12 weeks, and the authors concluded that somatostatin analogues do not appear to modify serum concentrations of calcitonin and CEA in patients with recurrent MTC. Note, however, that the doses administered by Díez et al. were markedly lower than those in our case, as was the treatment duration.
In 2004, Vainas et al. (7) reported results from a small trial (22 patients) with advanced MTC treated with either octreotide or octreotide LAR. Nine patients received only somatostatin analogues, while the other 13 also received chemotherapy (n = 6), external beam radiotherapy (n = 2), or a combination of the two (n = 5). In these 13 patients, 12 presented a tumor response—five partial responses and seven stabilizations. By contrast, in the nine patients treated only with somatostatin analogues, six showed a tumor response. There were no significant differences in overall survival between the two groups. Again, it should be noted that the doses used in that study were much lower (daily doses of 0.4–1.0 mg octreotide s.c., or monthly doses of 20–30 mg of long-acting octreotide intramuscularly) than the ones used in the present case. Moreover, the treatment was administered for periods as short as three months—a time period that may be far too short based on the authors' experience, especially when combined with low-dose treatment.
In 2009, Duntas et al. (8) conducted a review of the studies that had evaluated somatostatin analogues in MTC, finding that only a total of 55 patients had been assessed. Nonetheless, the authors found that partial remission was observed in 25–33% of MTC patients in those studies. Similarly, somatostatin analogues (administered at doses ranging from 200 to 1500 μg daily) achieved an initial decrease in calcitonin and/or CEA levels of up to 68% from baseline levels, although a rebound occurred within a few weeks in most cases. According to those authors, the most notable effect of somatostatin therapy was the improvement in clinical symptoms, notably diarrhea, malaise, and weight loss.
The general consensus (3,4,8) about the value of somatostatin analogues in the treatment of MTC seems to be that these drugs are ineffective in controlling tumor growth in MTC, although they may relieve certain symptoms in a subset of patients. Nevertheless, although anecdotal, the excellent outcome in the present patient contrasts with this notion. This is consistent with the favorable outcomes reported by Mahler et al. (6), who also used prolonged administration. Although no definitive conclusions can be reached based on a single case report, there are two key factors that may partially explain the excellent outcome in the present case versus those reported by most other authors: (i) the dose (Somatuline Autogel 120 mg s.c./28 days), which was higher than reported in other case series; and (ii) the use of prolonged administration. Doses and treatment duration vary highly from study to study but are generally lower and shorter than in the present case. It is worth emphasizing that calcitonin and CEA levels in the present patient (see Table 1) remained elevated for many months after somatostatin analogue treatment was started and did not normalize until after 11 months of treatment. To the authors' knowledge, none of the previous studies administered the drug for such an extended period, with the exception of Mahler et al. (6). Another mechanism of response in the present case could be related to or depend on the molecular or genetic profile of the tumor (RET mutation, RAS wild type), although obviously this would need to be tested in a formal way.
The current findings suggest that in asymptomatic patients with stable or slowly progressive indolent disease and positive uptake on the Octreoscan, somatostatin analogues may have an anti-proliferative effect in select patients. Thus, an important potential benefit of extended treatment with these drugs is that they could postpone the need for oral kinase inhibitors, thus avoiding (or at least delaying) the potential serious adverse side effects and major toxicity associated with these drugs (11,12).
Conclusion
The case presented here is one of the few described in the literature in which long-term treatment with Somatuline Autogel 120 mg s.c./28 days resulted in a sustained tumor response in a patient with recurrent metastatic MTC following surgery with a curative intent. Other reported cases evaluated the role of somatostatin mostly in the context of very advanced disease using low doses and a short treatment period. The findings in the present case raise the possibility that in asymptomatic cases with a low tumor burden and a positive Octreoscan following recurrence, prolonged treatment with somatostatin analogues may be beneficial.
Although understanding of the genetic and molecular alterations involved in MTC has increased tremendously in recent years, with several investigational drugs currently in Phase III clinical trials, treatment options remain limited. Based on the outcomes of this case, somatostatin analogues may have a potential role, although more data are needed from studies with larger sample sizes to confirm the findings observed in this case.
Footnotes
Acknowledgments
The authors wish to thank Bradley Londres for his assistance in translating and editing the text, and Ipsen Pharma S.A. for providing funding for these services.
Author Disclosure Statement
The translation and editing of this manuscript was funded by Ipsen Pharma S.A., who also paid for the article processing charges related to publication. No competing financial interests exist.