
Abstract
Background:
Fatigue is common among cancer survivors, but fatigue in thyroid cancer (TC) survivors may be under-appreciated. This study investigated the severity and prevalence of moderate and severe fatigue in TC survivors. Potential predictive factors, including physical activity, were explored.
Methods:
A cross-sectional, written, self-administered TC patient survey and retrospective chart review were performed in an outpatient academic Endocrinology clinic in Toronto, Canada. The primary outcome measure was the global fatigue score measured by the Brief Fatigue Inventory (BFI). Physical activity was evaluated using the International Physical Activity Questionnaire—7 day (IPAQ-7). Predictors of BFI global fatigue score were explored in univariate analyses and a multivariable linear regression model.
Results:
The response rate was 63.1% (205/325). Three-quarters of the respondents were women (152/205). The mean age was 52.5 years, and the mean time since first TC surgery was 6.8 years. The mean global BFI score was 3.5 (standard deviation 2.4) out of 10 (10 is worst). The prevalence of moderate-severe fatigue (global BFI score 4.1–10 out of 10) was 41.4% (84/203). Individuals who were unemployed or unable to work due to disability reported significantly higher levels of fatigue compared to the rest of the study population, in uni-and multivariable analyses. Furthermore, increased physical activity was associated with reduced fatigue in uni- and multivariable analyses. Other socio-demographic, disease, or biochemical variables were not significantly associated with fatigue in the multivariable model.
Conclusions:
Moderate or severe fatigue was reported in about 4/10 TC survivors. Independent predictors of worse fatigue included unemployment and reduced physical activity.
Introduction
A
One of the most distressing but prevalent symptoms of cancer survivors is fatigue, which may be present during and after active treatment (4). Persistent post-treatment fatigue has also been commonly reported among TC survivors (5). The level of fatigue experienced among TC survivors has been reported to be greater than that of age- and sex-matched normative populations from Europe and Asia, respectively (6,7). Furthermore, the prevalence of fatigue among TC survivors appears to be relatively comparable (and not lower) than that experienced by many other types of cancer survivors (8). However, the severity of fatigue among TC survivors is not well understood, particularly in relation to other socio-demographic, clinical, or life-style variables. The primary objective of this exploratory study was to describe severity and prevalence of moderate and severe fatigue among TC patients attending an academic endocrinology clinic in Toronto, Canada. A secondary analysis was performed, examining predictors of fatigue in this population, including demographic, disease, treatment, and biochemical characteristics, as well as physical activity. The rationale for examining the relationship between physical activity and fatigue is that increased physical activity is well-established in significantly reducing fatigue in cancer survivors (9 –11). The primary hypothesis, based on a prior scoping literature review (5), was that significant fatigue would not be uncommon (i.e., affecting approximately a quarter to close to half of the population). A secondary hypothesis was that TC survivors reporting more physical activity would experience reduced fatigue, given the beneficial effect of exercise in other cancer survivors (9 –11).
Materials and Methods
Study design and the eligibility criteria for the study population
The design of this study was a cross-sectional, self-administered written survey of TC patients, performed in parallel with a retrospective chart review of paper and electronic medical records of the study population. The study population consisted of TC patients who were followed in an academic outpatient endocrinology clinic in Toronto and who had a valid mailing address. Patients were eligible for the study at any time point in the disease treatment or survivorship follow-up trajectory and are herein referred to interchangeably as either patients or survivors. The patients were identified by a TC diagnosis code on MedBASE billing software between January 1, 2012, and November 1, 2015, and the diagnosis was verified by medical record review.
The survey was written in English. The survey was mailed to eligible patients in December 2015, with a second mailing to non-responders three weeks later. A self-addressed, postage-paid envelope was provided for return of the survey, and patient consent was implied by return of the completed questionnaire. Patients were not reimbursed for their participation. The study was approved by the University Health Network Research Ethics Board. The study was funded by the University Health Network Thyroid Cancer Endowment Fund.
Description of the questionnaires and outcomes
The survey included the following components: demographic questions (e.g., marital status, education, employment, having children), the Brief Fatigue Inventory (BFI) (12), and the International Physical Activity Questionnaire—7 day (IPAQ-7) (13 –15) to evaluate self-reported physical activity volume. The permission of developers was obtained for use of questionnaires where relevant (i.e., BFI), and all questionnaires were scored as per the developers' instructions.
The primary outcome measure was the Global Fatigue Index from the BFI questionnaire, which has well-established score categories for symptom severity (12). The BFI questionnaire was chosen, as in a systematic review and critical appraisal of questionnaires on fatigue in cancer survivors, it scored the highest on a total score of quality criteria (including appraisal of internal consistency, construct validity, interpretability, reproducibility, responsiveness, and floor and ceiling effects; top score tied with the FACIT fatigue questionnaire and the Fatigue Symptom Inventory) (16). Furthermore, it scored highest among uni- or multidimensional fatigue questionnaires for being user-friendly (16). Moreover, the BFI was reported to have highest psychometric quality criteria score of any fatigue questionnaire intended for cancer survivors, when both quality criteria and being user-friendly were incorporated in the total quality score (16). The BFI questionnaire has been previously utilized in TC survivors (7,17). Lee et al. reported that the BFI global fatigue score was significantly worse in disease-free TC survivors compared to the general population (7). The face validity of the BFI questionnaire was considered reasonable in the context of fatigue in TC survivors by a panel of experts, including an endocrinologist (A.M.S.), cancer fatigue expert (J.M.J.), head and neck surgeon (D.P.G.), radiation oncologist (J.B.), and cancer rehabilitation specialist with experience in care of TC patients (E.K.G.). The Global Fatigue Index of the BFI questionnaire is calculated by the mean the non-missing results of nine Likert-scale items (if more than half of responses are available for analysis) (12). The Likert scale ranged from 0 = “no fatigue severity/no impact” to 10 = “highest fatigue severity/highest adverse impact” (12). The BFI Global Fatigue severity was categorized as follows: mild = global BFI score ≤4), moderate = global BFI score 4.1–6.9, and severe fatigue = global BFI score ≥7 (12). The BFI questionnaire also includes one dichotomous (yes/no) question inquiring about feeling unusually tired last week, and the study reported on the prevalence of this outcome among respondents.
A secondary outcome measure was self-reported physical activity, as assessed by the IPAQ-7 questionnaire (13 –15). Participants were asked to report the number of days and duration of various levels of physical activity over the past week (e.g., vigorous, moderate, walking). The number of weekly minutes of each type of physical activity was respectively calculated. The metabolic equivalent minutes (MET minutes) were then estimated for each respective type of physical activity by multiplying the number of weekly minutes by the following constants: 3.3 for walking, 4.0 for moderate activity, and 8.0 for vigorous activity (12,13). The IPAQ-7 questionnaire was scored as per developers' instructions, including cleaning the data for missing and out-of-range values and truncating values as per pre-specified criteria (13,14). Physical activity scoring was independently verified by an expert in physical activity (D.S.M.).
Data collected from the medical record review also included demographic characteristics (e.g., age, sex), clinicopathologic features of disease (2009 American Thyroid Association [ATA] Risk of Recurrence initial disease stage) (18), current and previous TC treatments (e.g., surgery, radioactive iodine, thyroid hormone), recurrence status, and most recent thyroid-related biochemistry results. The time since initial TC surgery was also recorded. At the authors' institution, the thyrotropin (TSH), free thyroxine (fT4), and free triiodothyronine (fT3) concentrations were measured by a chemiluminescent immunoassay performed on the Abbott Architect i2000 analyzer (Abbott Diagnostics, Lake Forest, IL).
Data entry and analysis
A research assistant entered data from the questionnaires and chart review electronically in a spreadsheet (Microsoft® Excel). A subset of the completed survey data (69/205; 33.7%) and retrospective chart review data (33/205; 16.1%) was independently collected and verified by another staff member as a quality assurance check. Descriptive data were summarized as means and standard deviations or confidence intervals (or medians and interquartile ranges) for continuous data or as a number and percentage for nominal data. Spearman correlation statistics were calculated to evaluate associations between continuous outcome measures. In univariate analyses, means of continuous measures were compared between categorical variable groups using unpaired Student's t-tests (where variables with multiple categories were re-categorized in two grouped categories to simplify the analysis and interpretation of the results). A post hoc multivariable linear regression analysis was performed to explore for variables independently associated with BFI global fatigue score. The variables included in the multivariable analysis included those for which the p-value was <0.10 in the univariate analyses. The unstandardized regression coefficients were reported for all variables in the analysis, such that the change in BFI score was reported for any unit increase/change of each respective variable. The criterion for statistical significance was set at alpha = 0.050 for all analyses. Statistical analyses were performed using PASW Statistics for Windows v18.0 (SPSS, Inc., Chicago, IL).
Results
Response rate and characteristics of the study population
The survey response rate was 63.1% (205/325; Fig. 1). Approximately three-quarters of the responders (152/205) were women, which is in keeping with the expected sex distribution of TC. The mean age was 52.5 years (range 19–81 years), and mean time since first TC surgery was 6.8 years (range 1–38 years). The clinical and demographic characteristics of the responders are shown in Table 1. The majority of patients (95.1%; 195/204) were diagnosed with differentiated TC (DTC; with no other concurrent thyroid malignancy). Most patients had undergone a total thyroidectomy (completed in one or two stages) with or without neck nodal dissection (89.3%; 183/205). In the subgroup of 195 DTC patients, the respective prevalence of various ATA risk of recurrence categories was as follows: low risk, 59.8% (116/194); intermediate risk, 36.1% (70/194); and high risk, 4.1% (8/194; initial staging information not available for one patient). Furthermore, the prevalence rate of history of structural disease recurrence (or persistence) among the various ATA risk categories was as follows: low risk 3.4% (4/116), intermediate risk 17.1% (12/70), and high risk 37.5% (3/8). For the entire study population, the prevalence rates of various degrees of current TSH suppression were as follows: TSH <0.1 mIU/L, 25.4% (52/205); TSH 0.1–0.49 mIU/L, 31.7% (65/205); and TSH ≥0.5 mIU/L, 42.9% (88/205; all based on the most recent available measurements).
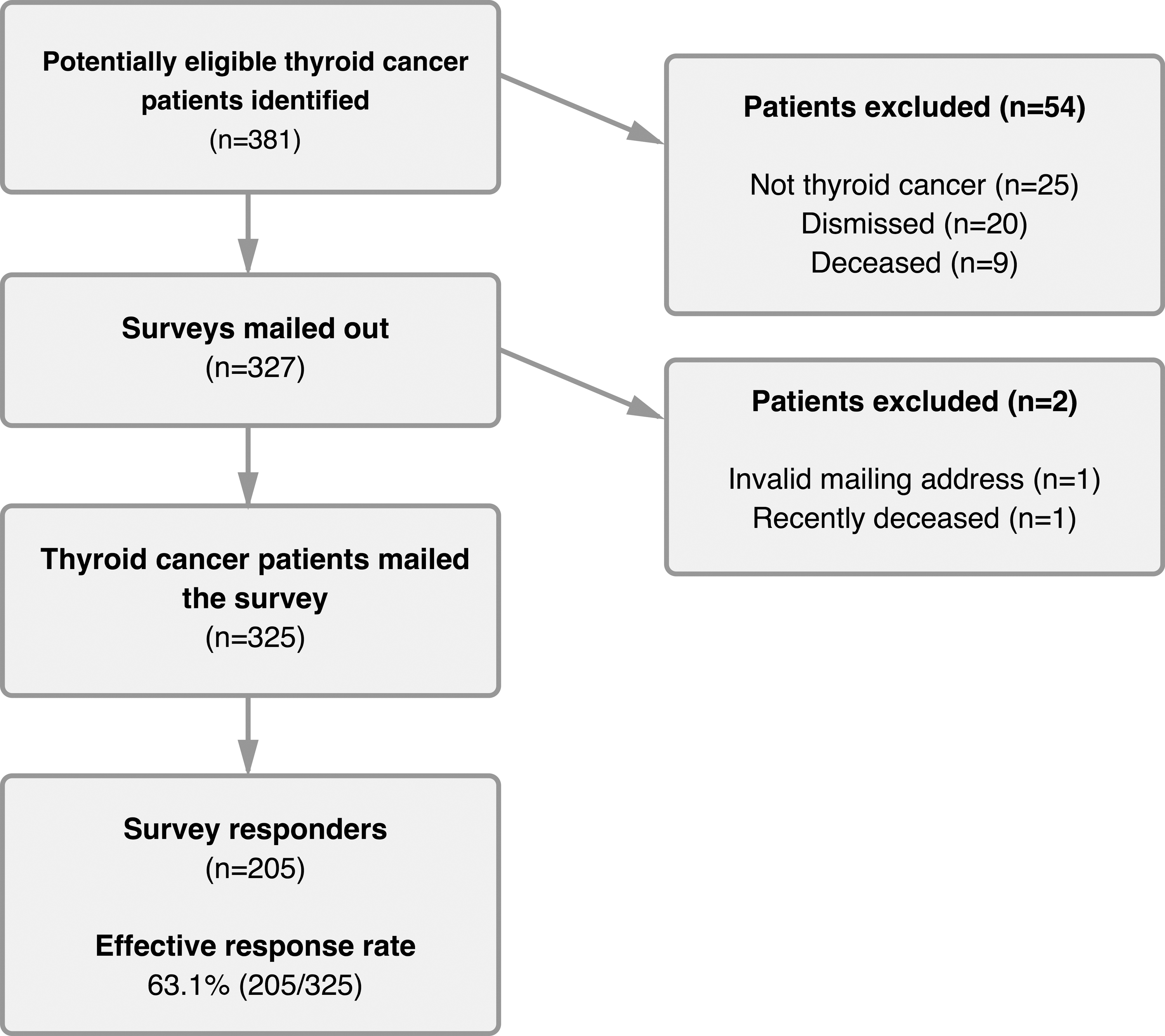
Flow of participants in the study.
American Thyroid Association Risk of Recurrence Classification for Differentiated Thyroid Cancer (2009 version).
There were 21 cases with recurrent or persistent disease (15 recurred in the neck, three were distant, and three were distant and in the neck).
SD, standard deviation; ATA, American Thyroid Association; TSH, thyrotropin; fT4, free thyroxine; fT3, free triiodothyronine.
Fatigue
The BFI global fatigue score was available for 99.0% (203/205) of respondents. The results of the responses to each of the individual questions on the BFI are shown in Figure 2. More than half of the responders (52.5%) reported feeling unusually fatigued in the past week. The mean BFI global fatigue score was 3.5 (standard deviation [SD] 2.4 [confidence interval (CI) 3.2–3.8]). The prevalence of mild, moderate, and severe fatigue was as follows: mild, 58.6% (120/203); moderate, 30.9% (63/203); and severe 10.3% (21/203), respectively. Only 7.4% (15/203) had a BFI global fatigue score of 0/10, which would represent no fatigue. Furthermore, among the 84 respondents with moderate or severe fatigue, the mean BFI global fatigue score was 5.9 (SD = 1.2).
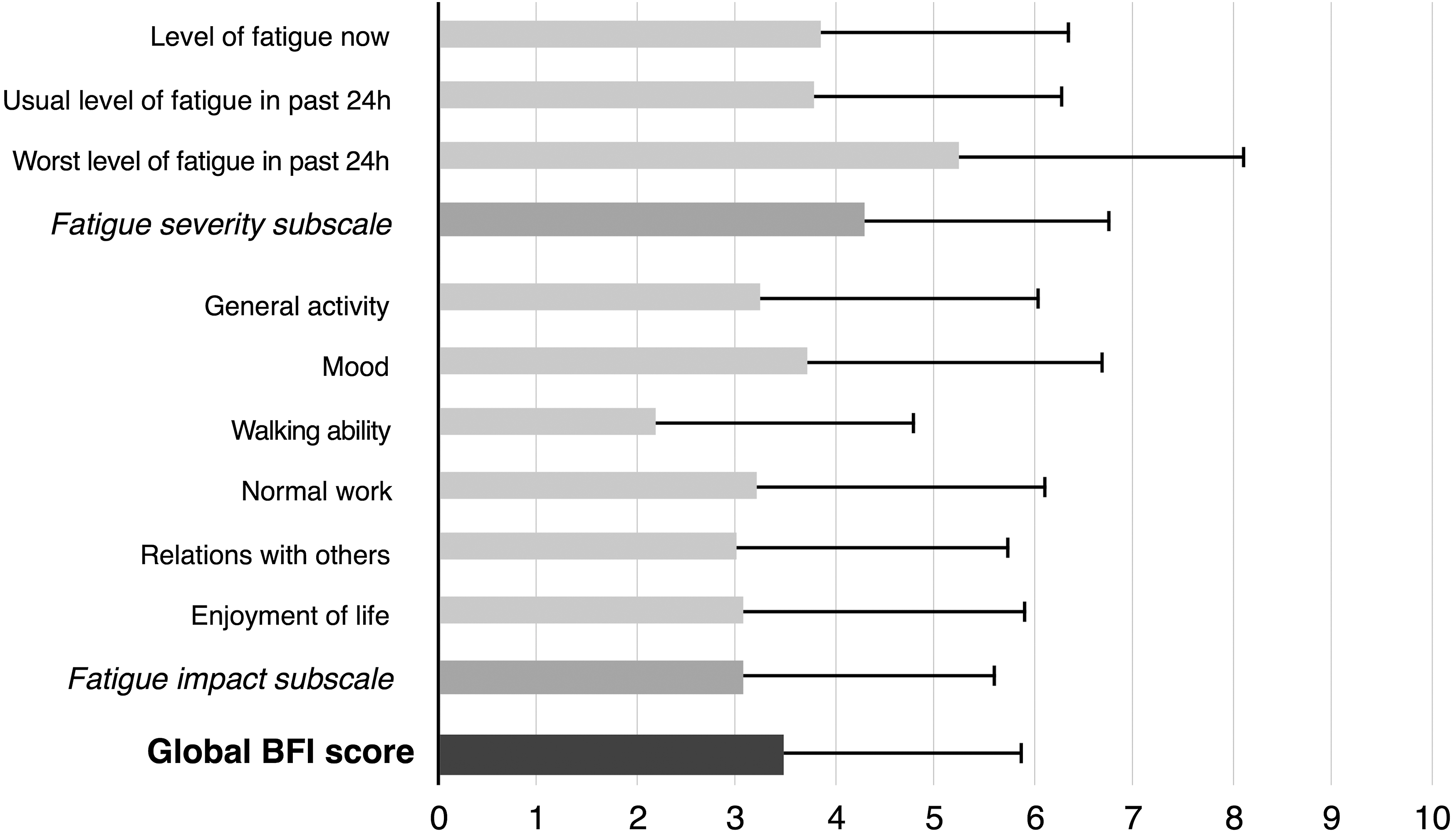
Results of responses to the Brief Fatigue Inventory Questionnaire (including fatigue severity and life impact of fatigue subscales).
Physical activity
All of the 205 participants provided physical activity data for the IPAQ-7 questionnaire, and the median (and interquartile range) of weekly minutes spent performing various types of activity were as follows: vigorous, 0 (0–180); moderate, 60 (0–240); and walking, 210 (90–840). However, in calculating the total weekly MET minutes of physical activity, one of the individuals was excluded in following the outlier exclusion rules of the IPAQ-7 developers (13,17). The mean total weekly MET minutes of moderate, vigorous, and walking physical activity were 3250 (SD = 3411; median 2330, interquartile range 751–4320; n = 204).
Exploratory analyses examining potential associations with fatigue
The following Spearman correlation statistics were observed for various variables in comparison with BFI global fatigue score: age, r = −0.145 (p = 0.039, n = 203); number of years since first TC surgery, r = −0.143 (p = 0.041, n = 203); TSH level (mIU/L), r = −0.098 (p = 0.166, n = 203); fT4 level (ng/dL), r = 0.132 (p = 0.060, n = 203); and fT3 level (pg/dL), r = −0.084 (p = 0.234, n = 203). In univariate comparisons of BFI fatigue scores, fatigue was significantly worse in women compared to men (t = 3.052, degrees of freedom [df] = 98, p = 0.003, n = 203), and significantly worse in individuals who were unemployed or unable to work due to disability compared to others (i.e., others including those who were employed, students, retirees, and full-time homemakers or caregivers; t = 3.996, df = 29, p < 0.001, n = 203), but it was not significantly associated with education level above high school (compared to high school or lower; t = 0.893, df = 74, p = 0.375, n = 201), ATA intermediate or high risk level for DTC (compared to low risk DTC; t = 1.667, df = 177, p = 0.097, n = 192), total thyroidectomy compared to hemithyroidectomy (t = 1.217, df = 29, p = 0.233, n = 203), or history of radioactive iodine treatment for TC (t = 0.676, df = 183, p = 0.500, n = 203). In examining the relationship between fatigue and self-reported physical activity, it was found that the BFI global fatigue score significantly was inversely correlated with weekly MET minutes of physical activity (r = −0.264, p < 0.001, n = 204).
In an exploratory multivariable linear regression analysis, including age (per decade increase), female sex (compared to male), being unemployed or unable to work due to disability (compared to employed individuals, students, retirees, homemakers, or caregivers), ATA intermediate or high risk level for DTC (compared to low-risk disease), fT4 level (ng/dL), duration of five or more years since first TC surgery (compared to shorter periods), and physical activity level (per increment of 500 MET minutes), it was found that increased physical activity was significantly independently associated with reduction of fatigue (i.e., for every increase in physical activity by 500 MET minutes per week, BFI global fatigue score was reduced by 0.08 points [CI −0.12 to −0.03], p = 0.002; Table 2). The only other variable that was significantly associated with worsening fatigue was being unemployed/on disability such that the BFI global fatigue score was 1.81 points higher ([CI 0.82–2.80], p < 0.001) in such individuals compared to those who were not unemployed (e.g., employed individuals, students, retirees, homemakers, or caregivers). However, age (by decade increase), female sex, ATA intermediate or high risk level of DTC, fT4 level, and five or more years since first TC surgery were not significantly independently associated with change in BFI global fatigue score (Table 2). Given the striking association between unemployment/inability to work due to disability and fatigue, a post hoc exploratory Student's t-test was conducted, comparing the responses to the BFI question specifically focusing on the degree to which fatigue interfered with normal work (including both work outside the home and daily chores) in the last 24 hours for the unemployed/disabled group compared to all others. It was found that the unemployed/disabled group reported significantly more interference with work attributed to fatigue compared to other individuals (mean score = 5.74/10 [SD = 2.8] in 23 individuals in the unemployed/disabled group compared to 2.89/10 [SD = 2.8] in the other 180 individuals; t = −4.65, df = 28, p < 0.001).
The final model r-value is 0.420, and the r 2 is 0.177. The total sample size included in this analysis is 191 individuals. The unstandardized regression coefficient reflects the change in BFI global fatigue score, relative to a one unit increase in respective continuous or ordinal variables, or bivariate comparator (e.g., female sex compared to males; unemployed or unable to work due to disability compared to individuals who are employed, full-time homemakers or caregivers, students, or retirees; individuals surveyed ≥5 years after their initial thyroid cancer survey compared to those whose surgery was <5 years prior).
The increment of weekly metabolic equivalent minutes of physical activity was chosen to be 500, as this is a clinically meaningful increment (i.e., equivalent to about half an hour of walking for 5 days per week).
Discussion
This study found that moderate or severe fatigue was reported by a substantial proportion of TC survivors (affecting approximately 4/10 individuals). Furthermore, in this study, the mean global fatigue score (measured by the BFI) was of 3.5 (SD = 2.4). Individuals who were unemployed or unable to work due to disability had significantly worse fatigue than others (e.g., employed individuals, homemakers/caregivers, students, retirees). However, it was not possible to ascertain the cause and effect of this finding definitively. Yet, the unemployed/disabled individuals reported significantly more interference with normal work due to fatigue compared to other individuals. It is possible that TC survivors with fatigue may be at risk for loss of employment due to this symptom, or that they may suffer from other comorbidities resulting in both fatigue and inability to work, or that the lack of employment may in part contribute to fatigue by loss of life structure, worsening emotional and financial distress, or other factors. The findings complement those of a recently published survey study from the Netherlands, in which Tamminga et al. reported that a higher level of fatigue was independently predictive of unemployment in long-term TC survivors (19). In examining the relationship between prior TC treatments and fatigue, no significant difference was observed in level of fatigue in individuals previously treated with radioactive iodine or not. Similarly, Drabe et al. observed no significant relationship of fatigue with this treatment variable (17). Moreover, statistically significant associations were not found between fatigue and TSH, fT4, or fT3 levels. Similarly, Drabe et al. (17) and Massolt et al. (20) also respectively reported no significant association between fatigue and these thyroid biochemical indexes in TC survivors. Taken together, these data suggest that fatigue in TC survivors may not be strictly explained by prior radioactive iodine treatment or thyroid biochemistry. More research is needed to understand the nature, etiology, and life consequences of fatigue better in TC survivors, which may include quantitative studies incorporating multidimensional measures of fatigue, more detailed measures of life impact, as well as in-depth qualitative research.
A relatively novel finding of the present study was that fatigue in TC survivors was significantly independently inversely associated with volume of self-reported physical activity, after adjustment for socio-demographic factors, disease stage, time since initial TC surgery, and thyroid biochemistry. In a randomized controlled trial of TC survivors, Vigário et al. reported that a 12-week program of supervised exercise (60 minutes of aerobic activity on a treadmill accompanied by stretching twice weekly) significantly improved fatigue (21) as well as quality of life (22) in this population. The benefit of physical activity on fatigue has been established in multiple systematic reviews of randomized controlled trials of various populations of cancer survivors (9 –11). The mechanism of fatigue in cancer survivors, including those who may be symptomatic many years after initial treatment, is not completely understood, but it is thought to involve multiple potential pathways, such as chronic inflammation, autonomic nervous system dysfunction (e.g., reflected by reduced resting heart rate variability), hypothalamic–pituitary–adrenal axis dysregulation (e.g., altered diurnal cortisol secretion or alteration in cortisol levels), sarcopenia, or psychological impairment (23). Mechanisms by which exercise may reduce fatigue in cancer survivors are thought to include improvement in psychological well-being and training-induced gains in physical fitness, anti-inflammatory effects (including reduction of neuro-inflammation), and improvement in autonomic function (e.g., as reflected by greater heart rate variability) (23). It is not known to what extent such mechanisms may contribute to fatigue and its observed amelioration with physical activity in TC survivors. Yet, given the benefits of physical activity in cancer survivors, the American College of Sports Medicine recommends that all cancer survivors who are physically able to do so follow physical activity guidelines for the general public, which includes 150 minutes of moderate-intensity or 75 minutes of vigorous-intensity physical activity (or equivalent combination) each week (24). Furthermore, the American College of Sports Medicine generally recommends that cancer survivors supplement aerobic physical activity with resistance and flexibility training (24). However, there is some limited evidence suggesting that TC survivors may not necessarily be receiving sufficient advice about physical activity from their healthcare providers, as reflected by a recent survey study in which 23% of low-risk DTC survivors reported that their physical activity information needs were not met (25).
Another barrier to physical activity of TC survivors may be a sense of isolation from other cancer survivors and cancer support services (26). This problem was revealed in a recent qualitative study that reported on a young adult TC survivor who contacted a local cancer support group for an exercise program but perceived “I don't know, there's part of me that feels like … I'm not worthy… I just have thyroid cancer … Am I deserving of this [support]?” (26). Thus, lack of information and encouragement from healthcare providers, as well as isolation from other cancer survivors and related support services, may be some of the barriers to increasing physical activity in TC survivors. Furthermore, in a recent systematic review of unmet information and support needs of TC survivors, it was recently reported that there were high unmet information and support needs during aftercare, including management of any symptoms related to the diagnosis of TC or its treatment (27). Moreover, recent oncology/psycho-oncology clinical practice guidelines (28) and adaptations of clinical practice guidelines (29) have strongly recommended encouragement/education of increased physical activity in the management of fatigue of all cancer survivors. It is not known to what extent physicians and surgeons caring for TC patients may be familiar with such guidelines, given that they have been sponsored by organizations outside of the traditional thyroid societies. One could argue that certainly more clinical trials of physical activity interventions in TC survivors are indicated to confirm the benefits in this population, as well as to identify the type, quantity, and intensity of physical activity that may be optimal for this group. Furthermore, strategies for successful long-term maintenance of physical activity need to be better defined for TC and other cancer survivors. However, pending such research, given the weight of indirect evidence in other cancer survivors (9 –11,24,28,29), limited but supportive randomized controlled trial evidence in TC survivors (21), as well as prevailing expert opinions on symptom management in cancer survivors (24,28,29), physical activity should be encouraged for all TC survivors (as for any other malignancy survivors), especially for individuals significantly affected by fatigue. Furthermore, TC survivors should be allowed access to supportive care, rehabilitation and exercise oncology programs/experts providing assistance with implementation of increased physical activity, as well as other strategies for management of fatigue.
The strengths of this study include the use of validated questionnaires, a reasonable response rate for an unreimbursed study, and few missing responses to most questions. Another strength is the execution of formal medical record reviews to ascertain disease status, pathology findings, treatment history, and biochemistry. Some limitations of this study include the lack of an age-and sex-matched population control group, the lack of data on physical or mental health comorbidities, potential response bias, a lack of prospectively collected repeated measures of fatigue, physical activity, employment status, and other variables before and after TC treatment, and lack of in-depth qualitative analysis. The small number of TC patients and survivors with subtypes other than DTC, high-risk disease, or those treated with hemi-thyroidectomy is another limitation of this study, limiting the extrapolation of the findings to those populations. The exploratory analyses are hypothesis generating. However, the findings suggesting a significant inverse relationship between physical activity and fatigue are confirmatory of extensive literature in general oncology populations (9 –11) and a small randomized controlled trial in TC survivors (21).
In conclusion, fatigue is a common complaint among TC survivors and is associated with being unemployed or being unable to work due to disability. Fatigue severity in this population does not appear to be related to thyroid hormone biochemical indexes but appears to be associated with reduced physical activity. Management of fatigue should be an essential component of TC survivorship care. More research is needed to understand the possible causes of fatigue and its optimal management better. The best available indirect and direct evidence from randomized controlled trials and systematic reviews suggests that physical activity may be beneficial in reducing fatigue in TC survivors, and so physical activity should be encouraged in this population.
Footnotes
Acknowledgments
The authors would like to thank Ms. Asima Naeem (research associate) and Mrs. Coreen Marino (research administrative assistant) for their work on this project. We are also very grateful to the study participants for completing our survey. This study was funded by the University Health Network Thyroid Cancer Endowment Fund. A.M.S. holds a University of Toronto Department of Medicine Clinician Scientist Merit Award. This work was presented in part at the 86th Annual Meeting of the American Thyroid Association in Denver, Colorado, on September 22, 2016.
Author Disclosure Statement
The authors have no commercial disclosures.