
Abstract
Background:
Maternal thyroid disease may complicate pregnancy. A high frequency of abnormal thyroid function test results in pregnant women with known thyroid disease has been reported, but the frequency of unidentified thyroid dysfunction in women first clinically diagnosed with thyroid disease after a pregnancy is not known.
Methods:
This was a population-based study of pregnant women in the Danish National Birth Cohort (DNBC) who had a blood sample drawn in early pregnancy and terminated the pregnancy with a singleton live-birth in the period between 1997 and 2003. Participants were all women in the DNBC who had a registration of thyroid disease before and/or up to five years after the pregnancy in nationwide health registers (n = 2445) and a 12% random sample of all women in the cohort (n = 7624). Thyrotropin and free thyroxine were measured with an immunoassay in sera stored in the Danish National Biobank. Method- and pregnancy week-specific references ranges were used for classification of thyroid function test abnormalities.
Results:
The frequency of abnormal thyroid function in early pregnancy was 12.5% in the random sample and 35.7% among women clinically diagnosed with thyroid disease before or after blood sampling (55.7% among women on current treatment). One third of women clinically diagnosed with thyroid disease after blood sampling had unidentified thyroid dysfunction in the early pregnancy blood sample (most frequently [52.0%] unidentified hypothyroidism in women with a later diagnosis of hypothyroidism).
Conclusions:
More than 50% of Danish pregnant women on current treatment for thyroid disease had thyrotropin and/or free thyroxine outside the week-specific reference ranges, and the frequency of unidentified early pregnancy thyroid dysfunction in women clinically diagnosed after the pregnancy was also high.
Introduction
A
When a pregnancy is planned, the woman should optimally be euthyroid before getting pregnant, and changes in therapy may be indicated (7). During the pregnancy, physiological changes in thyroid function challenge the interpretation of thyroid function tests and may alter the required dose of thyroid medication (8). However, studies from different countries have indicated that women with known hypothyroidism are not always adequately treated by the time they become pregnant (9 –12). After termination of the pregnancy, the immune rebound may trigger the onset or relapse of autoimmune thyroid disease (13,14).
Another issue is the management of women with no known thyroid disease. Current guidance advocates selective testing for thyroid dysfunction to identify individuals with a high risk for thyroid disease, for example women with a family history of thyroid disease, women with other autoimmune diseases, and women living in a region with presumed iodine deficiency (1 –3). The benefits and risks of routine testing for thyroid disease in pregnancy are, however, still insecure (5,6).
The Danish nationwide registration of health data provides the opportunity to study all pregnancies in Denmark and to perform long-term follow-up on the children. Using these data, a higher frequency of pregnancy complications and neurobehavioral diseases in children born to mothers with hyper- or hypothyroidism was previously observed (15 –19). Notably, a high risk was observed when the mother was first clinically diagnosed with thyroid disease in the years following the pregnancy. The proposed hypothesis was that these women might have suffered from undiagnosed and untreated thyroid dysfunction in pregnancy, which could have influenced the pregnancy and perhaps even programmed the fetus to later development of disease, but more evidence is needed to expand the concept of fetal programming by maternal thyroid disease (20).
To explore the hypothesis of unidentified early pregnancy thyroid dysfunction in women with a later diagnosis of thyroid disease, this study used biobank sera from Danish pregnant women in the Danish National Birth Cohort (DNBC) to study biochemical thyroid function test abnormalities in early pregnancy. This evaluation was performed both in women with no registration of thyroid disease before, during, and in the five-year period after the pregnancy and in women with a registration of thyroid disease prior to pregnancy, in the pregnancy, or first time in the five-year period after the pregnancy.
Method and Materials
Study population and design
The DNBC is a Danish nationwide birth cohort, which was established in 1996 and which aimed to recruit about 100,000 pregnant women who lived in Denmark, spoke Danish well enough to participate in telephone interviews, and intended to carry their pregnancy to term (21). As previously described (22), all women included in the evaluation of maternal thyroid disease in pregnancy gave birth to a singleton live-born child between 1997 and 2003. If the woman participated in the DNBC with more than one pregnancy, only the woman's first pregnancy in the study period was included.
To be eligible for inclusion in the present study, the woman had to have a blood sample drawn in early pregnancy, which was stored in the Danish National Biobank at the time of inclusion (23). From the 71,706 pregnant women eligible for the study, a 12% random sample was drawn (Fig. 1). In addition, all women in the entire cohort with a registration of thyroid disease before, during, and up to five years after the pregnancy were included in this study (Fig. 1).
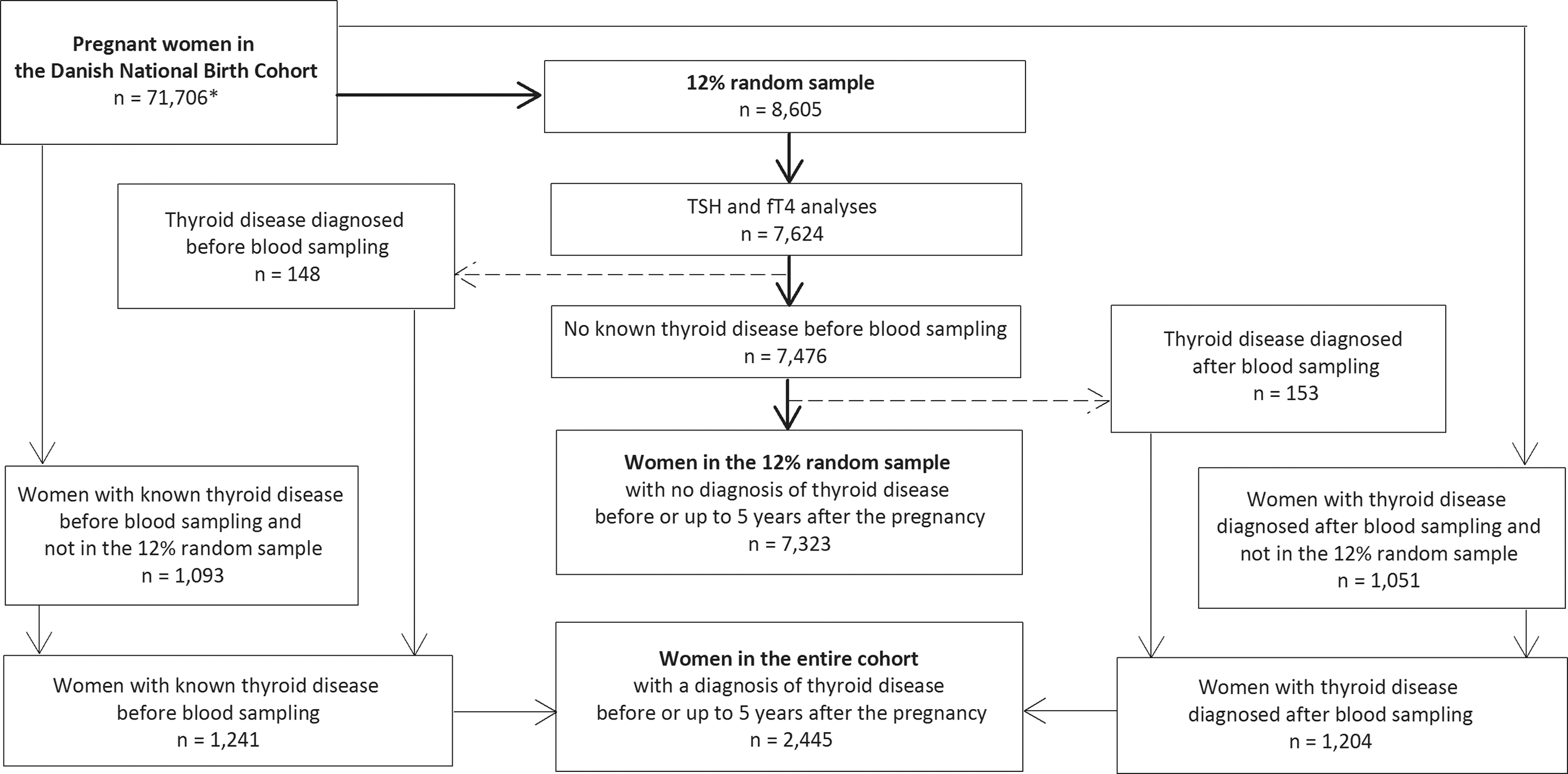
Flow chart illustrating the selection of women included in the present study from 71,706 Danish pregnant women (*) who were enrolled in the Danish National Birth Cohort (DNBC), gave birth to a singleton live-born child in Denmark between 1997 and 2003, had valid information on gestational age at birth of the child, and had a blood sample drawn in the early pregnancy, which was stored in the Danish National Biobank until measurement of thyrotropin (TSH) and free thyroxine (fT4). The women were either included as part of the random 12% sample and/or were included because they had been diagnosed with thyroid disease before, during, or in the five-year period after the pregnancy under study.
Information on maternal thyroid disease
As previously described in detail (22), information on hospital diagnosis and surgery of maternal thyroid disease was obtained from the Danish National Hospital Register, which includes diagnoses and surgery procedure codes for all inpatient visits in a Danish hospital since 1977 and also for all outpatient visits since 1995 (24). Information on the use of thyroid medication was obtained from the Danish National Prescription Register, which holds information on all redeemed prescriptions from Danish pharmacies since 1995 (25).
For each woman, any hospital diagnosis of thyroid dysfunction, benign goiter/nodules or thyroid cancer, as well as any registration of thyroid surgery or redeemed prescription of thyroid hormone or antithyroid drug (ATD) before, during, and up to five years after the pregnancy under study was identified. In addition, self-reported information was used on the use of thyroid medication at the time of blood sampling in early pregnancy, as well as self-reported information on thyroid disease at the telephone interview in early pregnancy.
Women were classified with known thyroid disease at the time of blood sampling if they reported to have thyroid disease diagnosed by a doctor or had taken thyroid medication in the pregnancy or if they had a registration of thyroid disease (hospital diagnosis, surgery, and/or medication) before the date the blood sample was drawn. Women with no self-report of thyroid disease and no registration prior to the date of blood sampling who had registrations in the period after the blood sampling and up to five years after the pregnancy were classified as diagnosed with thyroid disease after blood sampling.
The type of maternal thyroid disease (hyperthyroidism, hypothyroidism, benign goiter/nodules, thyroid cancer, other) was evaluated and specified as previously described in detail (22). For women with known thyroid disease at the time of blood sampling, the study examined if the women received current treatment for the disease in pregnancy. Current treatment was identified by self-reported use of thyroid medication at the time of blood sampling and/or redeemed prescription of thyroid medication in the period from three months before the pregnancy to the date of blood sampling.
Blood sampling in early pregnancy
Women included had a blood sample drawn at the time of the first pregnancy visit in general practice. The week of early pregnancy blood sampling ranged from the 5th to the 19th week of pregnancy (median 9th week of pregnancy). The blood sample was sent by regular mail for processing and stored in a −80°C freezer in the Danish National Biobank.
Thyrotropin (TSH) and free thyroxine (fT4) were measured by a Dimension Vista automated immunoassay (Siemens Healthcare Diagnostics, Germany) from January to August 2015, as previously described in detail (23). For both TSH and fT4, samples were measured blinded in random order, and internal/external controls were included.
Classification of thyroid function test abnormalities
For classification of maternal thyroid function test results, the method- and pregnancy week-specific reference ranges previously established and described for this cohort of women were used (23). For blood samples drawn in gestational weeks 5–14, the week-specific reference ranges were used. The number of blood samples drawn in gestational weeks 15–19 was limited (<100 samples per week), and therefore the combined reference ranges for weeks 15–19 were used (23). Overt hyperthyroidism was defined by TSH <2.5th percentile and fT4 > 97.5th percentile, and subclinical hyperthyroidism by TSH <2.5th percentile and fT4 within the reference ranges (three individuals had suppressed TSH and fT4 slightly below the lower reference range and were classified with subclinical hyperthyroidism). Overt hypothyroidism was defined by TSH >97.5th percentile and fT4 < 2.5th percentile, and subclinical hypothyroidism by TSH >97.5th percentile and fT4 within the reference ranges (five individuals had elevated TSH and fT4 slightly above the upper reference range and were classified with subclinical hypothyroidism). Furthermore, women were identified with isolated low fT4 and TSH within the reference ranges and with isolated high fT4 and TSH within the reference ranges.
Statistical analyses
Results are reported as the number of individuals (n) and the frequency (%) of thyroid function abnormalities in the random sample of women, as well as in women with known or later diagnosed thyroid disease. Furthermore, results were stratified by treatment and subtype of clinically detected thyroid disease.
Statistical analyses were performed using STATA v11 (Stata Corp., College Station, TX). Informed consent was signed at the time of enrollment in the DNBC. The study was approved by the Danish Data Protection Agency (J.nr. 2012-41-0046; J.nr. 2012-41-0171) and the Danish Ethics Committee (N-20130054).
Results
Abnormal maternal thyroid function in a random sample of pregnant women
Altogether, 7624 pregnant women (median age 30 years; range 16–47 years; 49.6% expecting their first child) in the 12% random sample had available measurements of TSH and fT4 in the early pregnancy blood sample (Fig. 1), and the overall frequency of abnormal thyroid function test results in this group of women was 12.5% (Table 1). Overt hyperthyroidism was more frequent than overt hypothyroidism, whereas subclinical hypothyroidism was more common than subclinical hyperthyroidism. The subsequent exclusion of women with known thyroid disease prior to blood sampling or later diagnosed thyroid disease did not considerably change these figures (Table 1).
See text for definition of subtypes of biochemical thyroid dysfunction.
Women in the random sample with no registration of thyroid disease (hospital diagnosis, redeemed prescription or self-reported disease) before the blood sample was drawn.
Women in the random sample with no registration of thyroid disease (hospital diagnosis, redeemed prescription or self-reported disease) before or after the blood sample was drawn in the pregnancy and in the five-year period after the pregnancy.
TSH, thyrotropin; fT4, free thyroxine.
Abnormal maternal thyroid function in women with known thyroid disease
Altogether, 1241 women were identified with known thyroid disease prior to blood sampling (Fig. 1). The frequency of biochemical thyroid function test abnormalities in early pregnancy in this group of women was 34.8% (Table 2) and was consequently almost three times higher than in the random sample. The majority of the women with known thyroid disease (n = 891) had been treated prior to the pregnancy alone, whereas 350 women received treatment for thyroid disease in the pregnancy prior to blood sampling (Table 2). The frequency of thyroid function test abnormalities was particularly high in women who received current treatment (55.7%).
See text for definition of subtypes of biochemical thyroid dysfunction.
Women who did not report any current treatment for thyroid disease at the time of blood sampling and who only had a registration of thyroid medication or thyroid surgery more than three months before the pregnancy under study.
Women who reported current treatment for thyroid disease at the time of blood sampling and/or had a registration of thyroid medication or surgery in the period ranging from three months before the start of the pregnancy under study to the date of blood sampling.
A small group (n = 13) of the 1241 women with known thyroid disease were newly diagnosed in the pregnancy prior to blood sampling. The frequency of abnormalities in thyroid function tests was high in this group (69.2%), including both hyperthyroidism and hypothyroidism.
Abnormal maternal thyroid function in women with later diagnosed thyroid disease
Altogether, 1204 women had no registration of thyroid disease before blood sampling but were first diagnosed with thyroid disease after the early pregnancy blood sampling or in in the five-year period after the pregnancy (Fig. 1). The overall frequency of thyroid function test abnormalities in early pregnancy in this group of women was 36.6% (Table 3), quite similar to the overall frequency in women with known thyroid disease (Table 2). A small group (n = 57) of the 1204 were newly diagnosed in the pregnancy after blood sampling. The frequency of abnormalities in thyroid function tests was high in this group (63.2%) and dominated by hyperthyroidism. Looking into which subtypes of thyroid disease the women were diagnosed with in or after the pregnancy (Table 3), the frequency of early pregnancy thyroid dysfunction was particularly high in women with a later diagnosis of hypothyroidism (57.5%).
Women with a later diagnosis of thyroid cancer, thyroiditis, or unspecified thyroid disease (n = 34) were not included in the diagnosis subtype columns. See text for definition of subtypes of biochemical thyroid dysfunction.
Women with a diagnosis of hyperthyroidism and/or redeemed prescription of antithyroid drugs.
Women with a diagnosis of hypothyroidism and/or redeemed prescription of thyroid hormone replacement and no registration of thyroid surgery, thyroid cancer, or hyperthyroidism.
Women with a diagnosis of benign goiter/nodules and/or a registration of thyroid surgery and no registration of hyperthyroidism or thyroid cancer.
Hyperthyroidism
Among women with a diagnosis of hyperthyroidism before or after blood sampling (upper part of Fig. 2), 359 women had been treated for hyperthyroidism before the pregnancy alone, 84 women received current ATD treatment in the pregnancy prior to blood sampling, and 484 women had no known hyperthyroidism at the time of blood sampling but were diagnosed later in the pregnancy or in the five-year period after birth of the child. The most frequent thyroid function abnormality in early pregnancy among these women was hyperthyroidism, and both subclinical and overt disease was much more frequent than in the random sample of women with no thyroid disease (upper part of Fig. 2). The highest frequency of early pregnancy hyperthyroidism was observed in women who received current treatment for hyperthyroidism (29.8%).
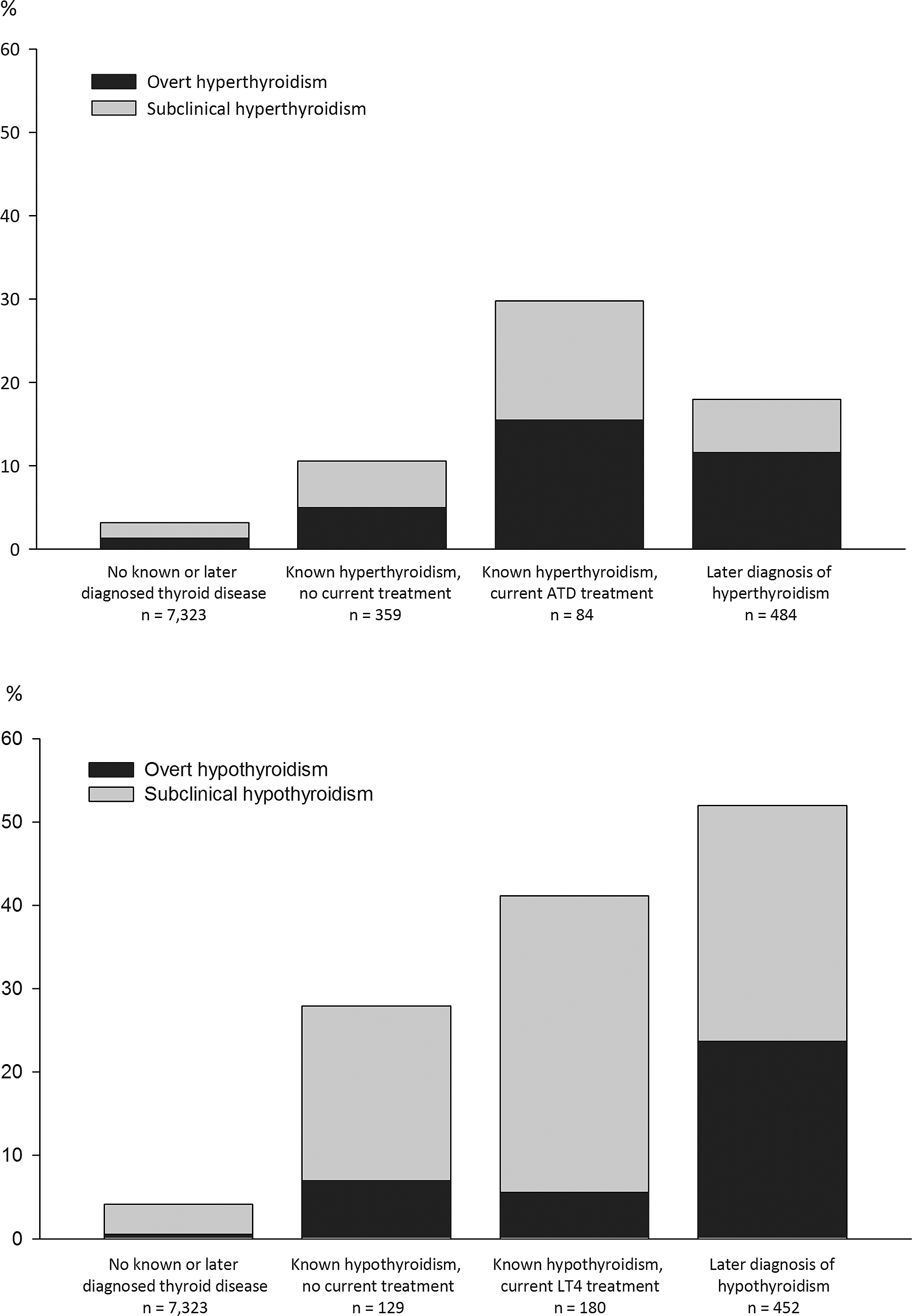
Frequency of overt and subclinical hyperthyroidism (upper figure) and hypothyroidism (lower figure) in an early pregnancy blood sample stored in the Danish National Biobank until measurement of TSH and fT4. The first column in each figure shows the frequency of disease in women with no registration of thyroid disease before or after the early pregnancy blood sampling. The middle columns show the frequency of disease in women with known thyroid disease who did or did not receive current treatment. The last column shows the frequency of disease in women first diagnosed with the disease after blood sampling had been performed and up to five years after the pregnancy. Women with known hyperthyroidism who received current replacement therapy (n = 58) or who underwent thyroid surgery in the early pregnancy (n = 1) are not shown.
A small group (n = 58) of women were not included in Figure 2 because they had previous hyperthyroidism but received current treatment for hypothyroidism in the early pregnancy. The most frequent early pregnancy thyroid function test abnormality in this group of women was hypothyroidism (39.7%). Furthermore, one woman with known hyperthyroidism underwent thyroid surgery in the early pregnancy before blood sampling. Her thyroid function in the biobank sera was normal.
Hypothyroidism
Among women with a diagnosis of hypothyroidism before or after blood sampling (lower part of Fig. 2) and no registration of thyroid surgery (non-surgical hypothyroidism), 129 women had been treated for hypothyroidism before the pregnancy alone, 180 women received current replacement therapy in the pregnancy prior to blood sampling, and 452 women had no known hypothyroidism at the time of blood sampling but were diagnosed later in the pregnancy or in the five-year period after the birth of the child. The most frequent thyroid function abnormality in early pregnancy among these women was hypothyroidism, and both subclinical and overt disease was much more frequent than in the random sample of women with no thyroid disease (lower part of Fig. 2). The highest frequency of early pregnancy hypothyroidism was observed in women who did not have known disease at the time of blood sampling but were later diagnosed with the disease (52.0%).
Benign goiter/nodules
Among women with a diagnosis of benign goiter or nodules (Fig. 3), 136 women were surgically treated prior to the pregnancy (hemithyroidectomy) and received no current treatment, whereas 240 women had a diagnosis of benign goiter or nodules but had not been surgically treated and received no current treatment in the pregnancy. The frequency of early pregnancy thyroid dysfunction was high in both groups (Fig. 3), but the dominant type of thyroid function abnormality differed. Women who were surgically treated prior to the pregnancy particularly suffered from subclinical hypothyroidism, whereas women who had not received treatment before or in the pregnancy mainly suffered from overt and subclinical hyperthyroidism.
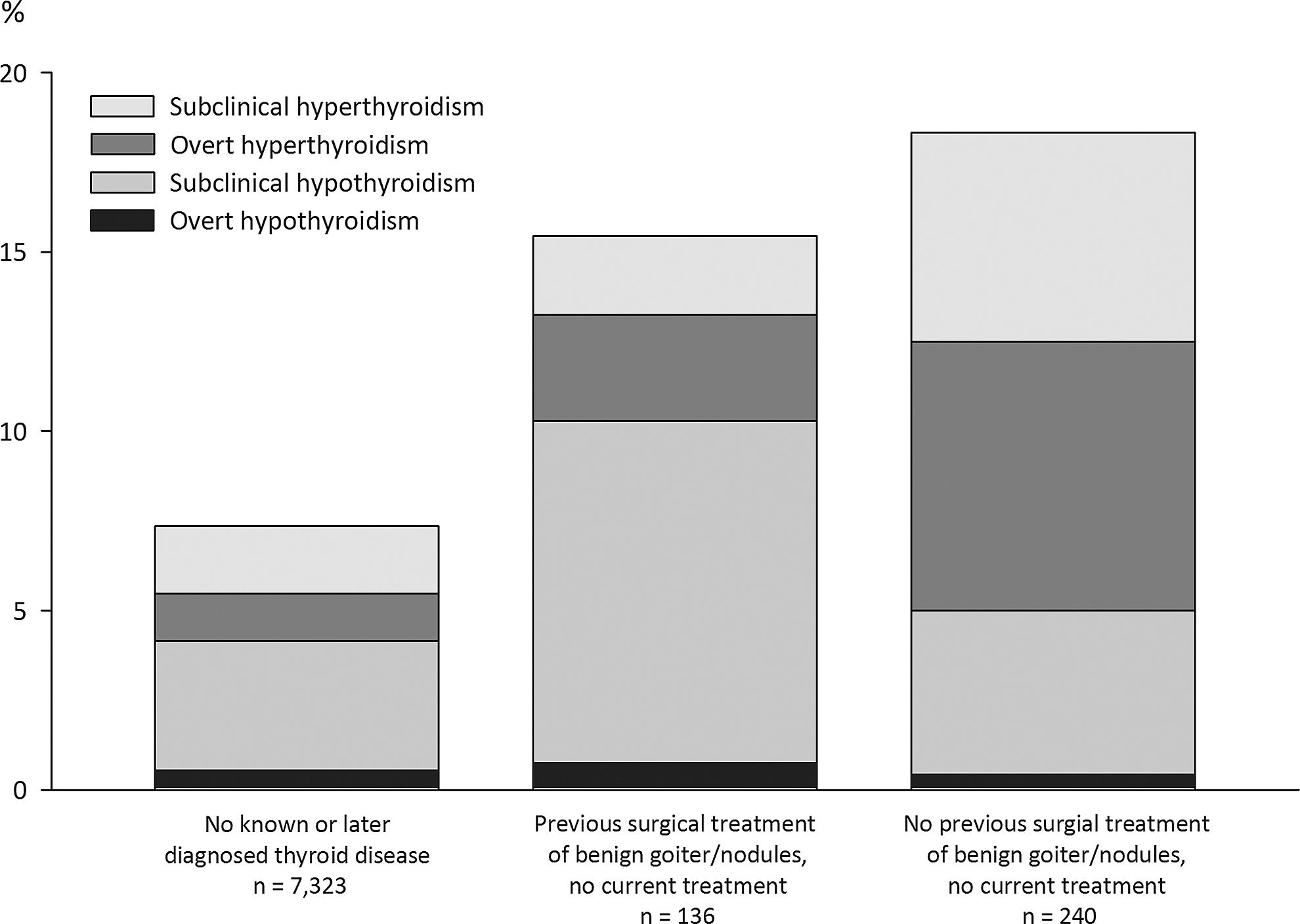
Frequency of overt and subclinical hyperthyroidism (upper figure) and hypothyroidism (lower figure) in the early pregnancy blood sample stored in the Danish National Biobank with performed measurement of TSH and fT4 years after the pregnancy. The first column shows the frequency of disease in women with no registration of thyroid disease before the early pregnancy blood sampling. The middle column shows the frequency of disease in women with known thyroid disease who were previously surgically treated but received no current medical treatment. The last column shows the frequency of disease in women who were not previously or currently treated for the disease. Women with known benign goiter/nodules who received current replacement therapy (n = 12) after previous thyroid surgery are not shown.
A small group (n = 12) of women were identified with benign goiter/nodules before the pregnancy and received current replacement therapy and were not part of Figure 3. In this group, four women had abnormalities in thyroid function tests (predominantly subclinical hypothyroidism). Furthermore, women with thyroid cancer (n = 35), thyroiditis (n = 31), or unspecified thyroid disease (n = 10) are not shown in Figures 2 and 3. The frequency of abnormalities in thyroid function tests among women with thyroid cancer (known or later diagnosed) was 34.3% and was dominated by overt hyperthyroidism.
Discussion
Principle findings
This is possibly the first study to illustrate the frequency of unidentified early pregnancy thyroid function test abnormalities in women with a later diagnosis of thyroid disease. This was made possible through the analysis of stored early pregnancy biobank sera and the linkage to Danish nationwide registers. Abnormal thyroid function test results in early pregnancy were common both in women with known thyroid disease and in women with undiagnosed disease that was clinically detected in the following years.
Early pregnancy thyroid function testing
The frequency of overt thyroid function test abnormalities in early pregnancy was ∼2% in this random sample of Danish pregnant women who gave birth to a live-born child between 1997 and 2003. On the other hand, subclinical thyroid function abnormalities, as well as isolated high or low fT4, were much more frequent. The prevalence of overt hypothyroidism was ∼0.5%, which is of the same magnitude as in other reports during the last decades on the frequency of unknown overt hypothyroidism detected by screening in early pregnancy (5). The prevalence of overt hyperthyroidism was higher than hypothyroidism in this study, which may be a consequence of the iodine status in Denmark around the time when the biobank sera were collected. The relation between iodine intake and thyroid disease in a population is U-shaped (26). Denmark was previously iodine deficient, but mandatory iodine fortification of salt was implemented in 2000 and this has increased iodine intake in the general Danish population and in pregnant women (27). Thus, the iodine fortification was initiated during the period when the biobank sera for the present study were collected, and the relative frequency of different subtypes of thyroid function test abnormalities may be different in recent years in line with the changes observed in the general Danish population after iodine fortification (27).
Management of women with known thyroid disease
Thyroid hormones are important developmental factors, and thyroid hormone receptors are present in the utero-placental unit and in the fetal brain beginning in early pregnancy (28,29). Thus, maternal thyroid hormones play an important role in the maintenance of a pregnancy and in the regulation of fetal brain development (28,29). Iodine is required for the synthesis of thyroid hormones, and in a recent pilot study (30), maternal iodine nutrition in pregnancy was associated with adverse cognitive development in the offspring independently of maternal thyroid status.
From a clinical viewpoint, thyroid dysfunction in a pregnant woman is a potential high-risk situation. Clinical guidance recommends that pregnant women with known thyroid disease should be carefully managed and controlled, and changes in therapy may already be considered when a pregnancy is planned (1 –4).
Studies from different countries have shown that women with known hypothyroidism may not be adequately treated by the time they become pregnant (9 –12). In these studies (9 –12), more than half of the pregnant women on current thyroid hormone replacement therapy had abnormal TSH in the first trimester of pregnancy. A similar high frequency of early pregnancy hypothyroidism was observed this study in women who received current levothyroxine treatment (∼40%), which was predominated by subclinical hypothyroidism. Notably, the present study evaluated the frequency of thyroid function test abnormalities in biobank sera that had been collected independent of the current management of the thyroid disease, whereas the previous studies (9 –12) addressed thyroid function in blood samples that were requested as part of the clinical management of the disease. A high frequency of abnormal thyroid function test results were also observed in this study in women with hyperthyroidism who received current treatment with ATD (∼30%), and this was characterized by both overt and subclinical hyperthyroidism. Furthermore, it was possible to distinguish women who had previously been diagnosed with and/or treated for a thyroid disease (hyper- and hypothyroidism as well as benign/goiter nodules) but who received no current treatment in the pregnancy. Notably, these groups of women also had a high frequency of abnormal thyroid function test results in the pregnancy.
These results stress the importance of careful management and control of pregnant women with current or previously treated thyroid disease. The high frequencies of thyroid function abnormalities observed in women who received current treatment may raise concern about the efficacy of the healthcare system. It should, however, be noted that evaluation was based on a single blood sample in early pregnancy, and the duration of thyroid abnormality in the pregnancy is unknown. Blood samples were drawn nearly two decades ago and may not apply to current practice, and there was no information available on patient-related factors (e.g., patient compliance).
A pertinent consideration is whether such thyroid abnormalities in women with known disease may influence the course of the pregnancy and the development of the fetus, as studies from Sweden (9) and the United Kingdom (11) have indicated. Further studies are needed on this important aspect.
Unidentified thyroid disease in pregnancy
As opposed to women with known thyroid disease, others will have no clinically detected thyroid disease at the time of pregnancy but may be diagnosed with thyroid disease in the years following the pregnancy. In Denmark, no universal routine testing for thyroid function in pregnant women is implemented, and the potential benefits and harms are debated worldwide (5,6).
Previously, the Danish nationwide registers were used to study all pregnancies in Denmark, and a higher risk of pregnancy complications and neurodevelopmental diseases were observed in the offspring when the mother had a diagnosis of thyroid disease (15 –19). This was particularly the case when the mother was first diagnosed and treated in the years following the pregnancy. It is speculated whether these women suffered from some degree of unidentified thyroid dysfunction in the pregnancy, which could have influenced the intrauterine environment and could have programmed the fetus to later development of neurobehavioral diseases (20). The proposed mechanism is that alterations in the supply of thyroid hormones to the developing fetal brain could lead to structural and/or functional developmental abnormalities in the brain, which in turn could predispose the offspring to onset of disease later in life (20). In general, the molecular mechanisms underlying in utero programming of disease are far from understood, but emerging evidence has focused on epigenetic modifications (31).
The present study observed a very high frequency of early pregnancy thyroid function test abnormalities in biobank sera from women diagnosed with thyroid disease in the five-year period after the pregnancy. In particular, a high frequency (∼50%) of early pregnancy hypothyroidism was observed in women with a later diagnosis of hypothyroidism. Symptoms of hypothyroidism are often unspecific, and the disease may be present for a period before the diagnosis is made (32). Furthermore, for the diagnosis of hypothyroidism in pregnant women, the symptoms may mimic pregnancy-related symptoms, which further challenges clinical detection.
The results of the present study strengthen the hypothesis that unidentified abnormalities in thyroid function are present in women with a later diagnosis of thyroid disease, but it remains to be elucidated whether the biochemical thyroid abnormalities are also associated with pregnancy outcomes and the long-term development of the child.
Methodological considerations
The study design provided the possibility of performing linkage to Danish nationwide registers for information on diagnosis and treatment of maternal thyroid disease before, during, and after the pregnancy. The validity of the Danish nationwide registers is in general considered high (24,25). Thyroid medications are sold solely as prescription drugs in Denmark, and the use of these drugs is limited to thyroid disease. Information was available in the registers on thyroid surgery but not on radioiodine treatment.
The blood samples were stored for years until analysis, but all samples were drawn and managed in the biobank and the laboratory without knowledge about maternal thyroid disease. The procedure is not considered to have affected the findings, but any potential misclassification related to the handling of the blood samples is considered non-differential. Classification of maternal thyroid disease was performed using the method- and pregnancy week-specific reference intervals established in this cohort (23). No information was available on thyroid autoantibodies, but the reference intervals were determined on “healthy” pregnant women, as previously described in detail (23).
All the women who participated in the present study were selected from participants in the DNBC. They all spoke Danish well enough to participate in a phone interview, and they gave birth to a live-born child. Thus, the figures presented in this study may not apply to pregnant women of non-Danish origin and may also differ in pregnancies terminating with pregnancy loss. The study conditioned on survival, which may introduce selection bias, but such bias is considered small.
Conclusion
The frequency of early pregnancy thyroid function test abnormalities was high in Danish pregnant women based on biobank sera collected in 1997–2003. More than 50% of Danish pregnant women with known thyroid disease had TSH and/or fT4 levels outside the week-specific reference ranges, and more than 50% of women with thyroid disease diagnosed after the pregnancy had unidentified thyroid dysfunction in the early pregnancy. Studies are needed to evaluate the potential consequences of such thyroid abnormalities.
Footnotes
Acknowledgments
We dedicate this manuscript to Professor Peter Laurberg, Department of Endocrinology, Aalborg, Denmark, who passed away on June 20, 2016. Professor Peter Laurberg made the study possible, participated in the design of the study, was responsible for the biochemical analyses, and participated in the analyses of the results.
This work was supported by the Obel Family Foundation. This research has been conducted using the Danish National Biobank resource. The Danish National Biobank is supported by the Novo Nordisk Foundation. The Danish National Research Foundation has established the Danish Epidemiology Science Centre that initiated and created the DNBC. The cohort is furthermore a result of a major grant from this Foundation. Additional support for the DNBC is obtained from the Pharmacy Foundation, the Egmont Foundation, the March of Dimes Birth Defects Foundation, the Augustinus Foundation, and the Health Foundation.
Author Disclosure Statement
No competing financial interests exist.