
Abstract
Background:
While there is a clear consensus for defining radioiodine-refractory differentiated thyroid cancer (RR-DTC), it is unknown whether these criteria are equally valid for determining when radioiodine (RAI) therapy is no longer beneficial and systemic treatment should be considered. Lenvatinib, a multikinase inhibitor, significantly prolonged progression-free survival (PFS) compared to placebo in a Phase 3 trial in RR-DTC (SELECT; hazard ratio [HR]: 0.21 [99% confidence interval (CI) 0.14–0.31]; p < 0.001). This sub-analysis compared clinical outcomes of lenvatinib-treated patients in SELECT stratified by RR-DTC inclusion criteria.
Methods:
In SELECT, patients with measurable RR-DTC and radiologic evidence of disease progression ≤13 months prior to study entry were randomized 2:1 to lenvatinib (24 mg/day; 28-day cycle) or placebo. In this analysis, patients were stratified based on the following RR-DTC inclusion criteria: no RAI uptake, disease progression within 12 months of RAI therapy despite RAI avidity at the time of treatment, and extensive (>600 mCi) cumulative RAI exposure. All had disease progression as an inclusion criterion for SELECT.
Results:
Of 392 patients (261 lenvatinib; 131 placebo) enrolled, 275, 235, and 73 patients met the inclusion criteria for no RAI uptake, disease progression despite RAI avidity, and extensive RAI exposure, respectively. There was significant overlap between the patient groups, with 167 (42.6%) patients meeting more than one inclusion criterion. Lenvatinib improved median PFS compared to placebo in all groups (“no RAI uptake”: lenvatinib not quantifiable [NQ; CI 14.8–NQ] vs. placebo, 3.7 months [CI 2.5–5.3]; “disease progression despite RAI avidity”: lenvatinib 16.5 months [CI 12.8–NQ] vs. placebo, 3.7 months [CI 1.9–5.4]; “extensive RAI exposure”: lenvatinib 18.7 months [CI 10.7–NQ] vs. placebo, 3.6 months [CI 1.9–5.5]). Objective response rates were 71.8%, 60.0%, and 56.0% for patients with no RAI uptake, disease progression despite RAI avidity, and extensive RAI exposure, respectively. Lenvatinib-related adverse events were similar across groups.
Conclusions:
Comparable efficacy and safety profiles were observed in lenvatinib-treated patients regardless of RR-DTC criteria, possibly because of a large overlap among patients fulfilling each criterion. However, differing definitions for RR-DTC may be equally valid because both lenvatinib and placebo arms exhibited similar PFS outcomes across groups.
Introduction
A
Patients with RR-DTC have few options if further treatment is needed for metastatic disease, and novel therapeutic strategies are therefore required (3). Tyrosine kinase inhibitors (TKIs) have demonstrated promising results in the treatment of RR-DTC (3,5). Lenvatinib is an oral multikinase inhibitor that targets vascular endothelial growth factor receptors 1–3, fibroblast growth factor receptors (FGFR) 1–4, platelet-derived growth factor receptor-alpha, and RET and KIT proto-oncogenes (6 –8). Lenvatinib has been approved for the treatment of patients with RR-DTC in Japan, Europe, and the United States (9), based on the results of the randomized, double-blind, multicenter, Phase 3 Study of (E7080) LEnvatinib in Differentiated Cancer of the Thyroid (SELECT) trial, in which lenvatinib significantly increased progression-free survival (PFS) in patients with RR-DTC compared to placebo (hazard ratio [HR] = 0.21 [99% confidence interval (CI) 0.14–0.31]; p < 0.001) (10).
Patients with RR-DTC often present with clinically heterogeneous lesions (5,10 –12). Based on clinical presentation and tumor imaging scans, most patients with RR-DTC fall into one or more of the following categories (13,14): those with metastatic disease that does not take up RAI at the time of initial treatment; those with tumors that have previously taken up RAI but have lost the ability to do so; those with tumors that retain RAI uptake in only some lesions; those with metastatic disease that progresses despite substantial RAI uptake; and those with disease progression despite receiving >600 mCi (22.3 GBq) of RAI.
In clinical studies in accordance with the prescribed criteria for RR-DTC, TKIs showed efficacy, but the correlation between each of these categories of RR-DTC and a patient's response to RAI therapy is unclear. Therefore, establishing a common definition for RR-DTC has become increasingly important because clinicians need to recognize the point at which RAI therapy is no longer beneficial to a patient and when to initiate the use of emerging systemic treatment options for this disease setting. This analysis examines the efficacy and safety of lenvatinib in patients with RR-DTC according to the three definitions of RR-DTC used as inclusion criteria in SELECT.
Materials and Methods
Study design
The full details of SELECT (
For the current analysis, patients in SELECT were stratified according to the three RR-DTC inclusion criteria. Patients with one or more measurable lesion that did not demonstrate RAI uptake on any RAI scan were included in the “no RAI uptake” group. Patients with measurable lesions that had progressed within 12 months of RAI therapy per Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST v1.1) (15) despite demonstration of RAI avidity at the time of treatment by pretreatment or posttreatment scanning (these patients were not eligible for possible curative surgical therapy) were included in the “disease progression despite RAI avidity” group. Finally, patients who had received a cumulative activity of RAI >600 mCi (22 GBq), with the last treatment administered less than six months prior to study entry were included in the “extensive RAI exposure” group (10). It is important to note that patients could be included in multiple categories, and this could obscure differences among the three RR-DTC inclusion criteria groups.
Endpoints and assessments
The primary endpoint of SELECT was PFS determined by independent radiologic review in the intent-to-treat population. Secondary endpoints included the objective response rate (ORR) comprising complete or partial response according to RECIST v1.1, and overall survival (OS). Survival endpoints were calculated using Kaplan–Meier product-limit estimates and a stratified log-rank test. Calculation of HRs and associated CIs used a Cox proportional hazards regression model stratified by the randomization factors. Response rates were compared using stratified Cochran–Mantel–Haenszel tests at a two-sided alpha level of 0.05 (10).
Adverse events (AEs) were recorded and assessed according to the National Cancer Institute Common Terminology Criteria for Adverse Events version 4.0 (16). Other safety assessments included symptom and vital signs reporting, hematologic and biochemical laboratory testing, urinalysis, electrocardiography, and echocardiography (including left ventricular ejection fraction) (10).
Results
SELECT enrolled 392 eligible patients from 21 countries (the Americas, Europe, Asia, and Australia) between August 2011 and October 2012 (10,17). The cutoff date for the primary data analysis was November 15, 2013. The median follow-up at this time was 17.1 months for patients who received lenvatinib and 17.4 months for patients on placebo.
Patient groups and characteristics
Of the 392 patients enrolled in SELECT (261 lenvatinib, 131 placebo), 275 patients met the inclusion criteria for “no RAI uptake,” 235 for “disease progression despite RAI avidity,” and 73 for “extensive RAI exposure” (Table 1). All patients had disease progression as an inclusion criterion in SELECT. Baseline characteristics were similar across groups, with the exception of median RAI activity received, which was higher in the “extensive RAI exposure” group (Table 1). A total of 167 (42.6%) patients met more than one RR-DTC criterion and were therefore included in multiple groups (Fig. 1). The greatest overlap was in the “no RAI uptake” and “disease progression despite RAI avidity” groups, in which 117 (29.8%) patients qualified for both groups. There was only minor overlap between the “no RAI uptake” and “extensive RAI exposure” groups (n = 6; 1.5%). The number of patients categorized into both the “disease progression despite RAI avidity” and “extensive RAI exposure” groups was slightly higher (n = 19; 4.8%). There were 25 (6.4%) patients who met all three RR-DTC group criteria. Of the patients enrolled, 224 (57.1%) met only one RR-DTC inclusion criterion. For the 106 total lenvatinib-treated patients across all groups, 65 (61.3%) were ≤65 years old, 59 (55.7%) had papillary histology, 47 (44.3%) had follicular histology, 27 (25.5%) had disease progression or death within six months of randomization, and the median tumor size at baseline was 60.9 mm (range 15.1–331.2 mm). For the 61 total placebo-treated patients, 39 (63.9%) were ≤65 years old, 48 (78.7%) had papillary histology, 13 (21.3%) had follicular histology, 41 (67.2%) had disease progression or death within six months of randomization, and the median tumor size at baseline was 59.9 mm (range 15.2–236.1 mm).

Venn diagram of patients in SELECT by RR-DTC criteria group. Information is not available for one patient. RAI, radioiodine; RR-DTC, radioiodine-refractory differentiated thyroid cancer; SELECT, Study of (E7080) LEnvatinib in Differentiated Cancer of the Thyroid.
Asia including Japan, Republic of Korea, and Thailand.
Data available for 162 patients.
Data available for 96 patients.
Data available for 154 patients.
Data available for 79 patients.
ECOG PS, Eastern Cooperative Oncology Group performance status; GBq, gigabecquerel (1 GBq = 27.0 mCi); RAI, radioiodine; RR-DTC, radioiodine-refractory differentiated thyroid cancer; TSH, thyrotropin; VEGF, vascular endothelial growth factor.
Efficacy
The efficacy of lenvatinib was maintained in all three groups regardless of the RR-DTC criteria used, with lenvatinib treatment resulting in significantly longer PFS compared to placebo in all three RR-DTC criteria groups (Figs. 2A–C). Notably, in the placebo arms, PFS was similar regardless of RR-DTC inclusion criteria. Median PFS, in months, in the “no RAI uptake” group was not quantifiable (NQ [CI 14.8–NQ]) versus 3.7 months [CI 2.5–5.3] in the lenvatinib and placebo arms, respectively. In the “disease progression despite RAI avidity” group, median PFS was 16.5 months [CI 12.8–NQ] for lenvatinib versus 3.7 months [CI 1.9–5.4] for placebo. The median PFS in the “extensive RAI exposure” group also favored lenvatinib (18.7 months [CI 10.7–NQ]) compared to placebo (3.6 months [CI 1.9–5.5]).
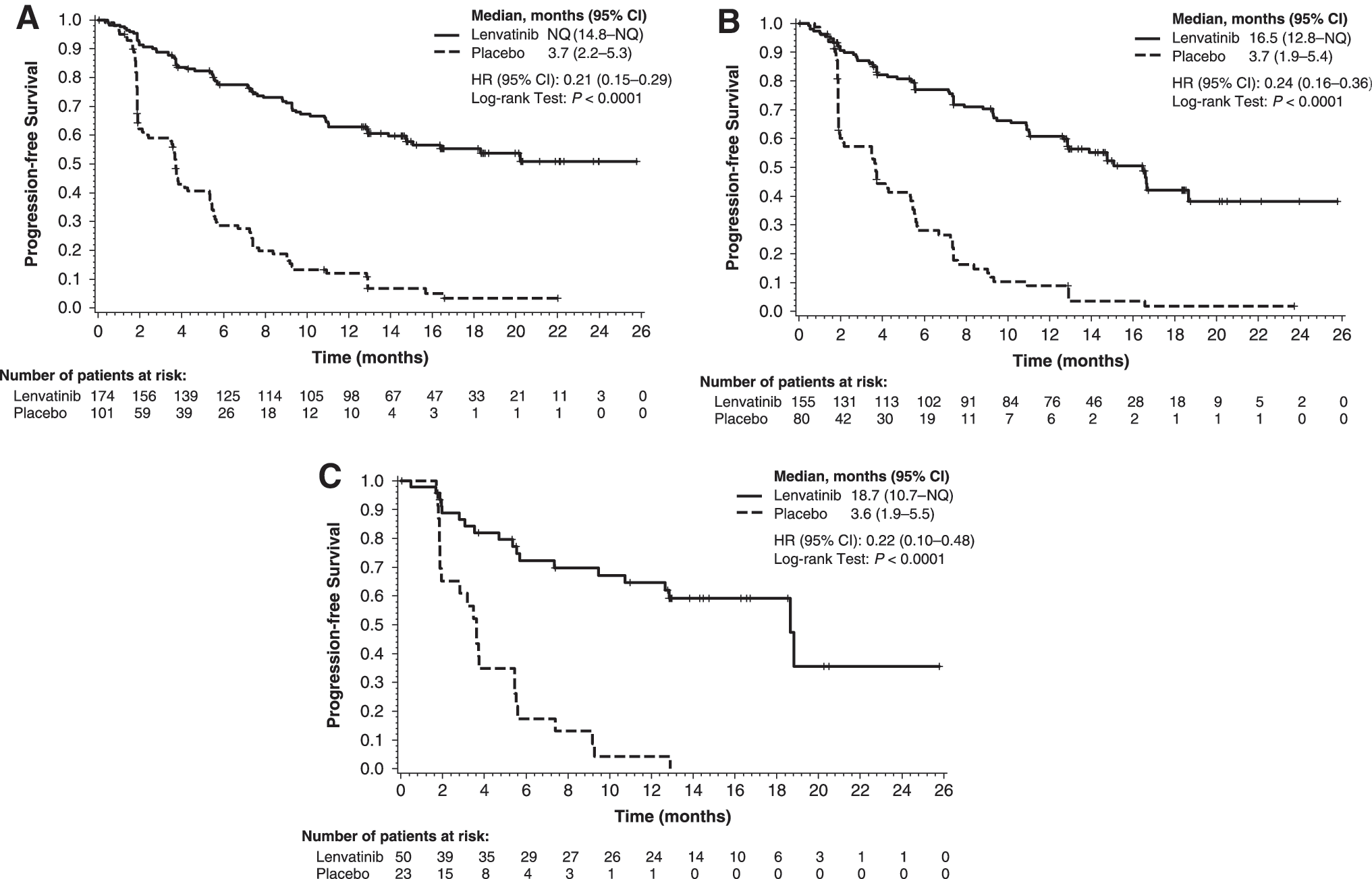
Kaplan–Meier estimates of progression-free survival by RR-DTC inclusion criteria: (
The ORRs were 71.8%, 60.0%, and 56.0% for patients receiving lenvatinib in the “no RAI uptake,” “disease progression despite RAI avidity,” and “extensive RAI exposure” groups, respectively, compared to 2.0%, 1.3%, and 0%, respectively, for patients receiving placebo (Table 2). Complete responses were reported for three patients in the “no RAI uptake” group and two patients in the “disease progression, despite RAI avidity” group. No patients receiving placebo reported a complete response (Table 2). At data cutoff, median OS was NQ for any group.
ORR, objective response rate.
Safety
Patients in all three overlapping RR-DTC criteria groups received comparable numbers of cycles of lenvatinib treatment (range 14–16 cycles). Dose intensity and duration of lenvatinib treatment were also similar across groups (Table 3). The safety profiles were generally comparable between the three RR-DTC criteria groups (Table 4). Almost all patients (>96%) experienced a lenvatinib-related treatment-emergent adverse event (TEAE) in each criteria group. The proportions of patients who experienced lenvatinib-related TEAEs of grade ≥3 were also similar across groups, ranging from 73.6% in the “no RAI uptake” group to 76.0% in the “extensive RAI exposure” group. Likewise, the proportion of patients who required lenvatinib dose reductions because of TEAEs was comparable between groups at 69.0% in the “no RAI uptake” group, 63.9% in the “disease progression despite RAI avidity” group, and 56.0% in the “extensive RAI exposure” group. Serious AEs were experienced by 44.3% of patients in the “no RAI uptake” group, 54.2% of patients in the “disease progression despite RAI avidity” group, and 58.0% of patients in the “extensive RAI exposure” group. Fatal treatment-related AEs occurred in 1.1% of patients in the “no RAI uptake” group, 1.3% of patients in the “disease progression despite RAI avidity” group, and 2.0% of patients in the “extensive RAI exposure” group.
TEAE, treatment-emergent adverse event.
Discussion
This analysis demonstrates that the efficacy and safety of lenvatinib was similar regardless of the RR-DTC criteria used to select patients for enrollment in SELECT. PFS, the primary efficacy measure in the original trial, was significantly longer in patients receiving lenvatinib compared to placebo in all three RR-DTC criteria groups. The comparable outcomes observed among the RR-DTC criteria groups suggest that lenvatinib may be effective in treating RR-DTC, irrespective of the criteria used to define the parameters of the radioiodine refractoriness. Likewise, patients in all three groups were similarly tolerant of the treatment, with little variation in the safety outcomes between the three RR-DTC groups. It is important to note that there was a large number of patients who satisfied the criteria for more than one RR-DTC group, including nearly 30% of patients who fulfilled both the “no RAI uptake” and “disease progression despite RAI avidity” criteria, which likely influenced the comparable efficacy and safety profiles between RR-DTC criteria groups. In addition, all patients in SELECT had disease progression, and this is a major confounding factor in this analysis.
The three RR-DTC criteria used in this study have been used in a number of other studies (11,14,18). However, the criteria have been considered unsatisfactory by some researchers, as the RAI activity given per treatment has often been undefined in studies, leading to uncertainty as to whether the activity was truly in the therapeutic range or if, in fact, radioiodine-refractory properties were defined based on lack of response to sub-therapeutic RAI activity (19). The maximum cumulative RAI activity (600 mCi or 22 GBq) is somewhat arbitrary and is based on studies that showed that cumulative activity >600 mCi increased the risk of secondary cancers but was unlikely to be associated with complete responses (4,14,19). It is possible that a patient classified with RR-DTC using these criteria may in fact not be refractory to RAI at all, and some authors have argued that the total cumulative RAI activity should be based on toxicity and efficacy in individual patients rather than on broad guidelines (20).
Disease progression, despite RAI treatment, has been identified as an important indication for starting a patient on a TKI, as differentiated thyroid cancer follows a generally indolent path (5). Initiation of treatment with a TKI should be done in order to achieve a specific patient-related outcome, such as tumor response or symptom control, and with due consideration of toxicity risks (5). Notably, lenvatinib also demonstrated activity in patients who had already progressed after receiving a different TKI, possibly because of lenvatinib inhibiting a unique set of kinase receptors, including FGFRs (10). The present analysis suggests that lenvatinib may also be effective, irrespective of the RR-DTC criteria used to identify radioiodine-refractory patients who showed disease progression within the previous 13 months. This disease progression requirement for inclusion in the study may also contribute to similarities in PFS among patients treated with lenvatinib presented here.
In conclusion, this analysis demonstrates that lenvatinib-treated patients experience comparable efficacy and safety profiles regardless of RR-DTC criteria used. These results may indicate that differing definitions for RR-DTC are equally valid for selection for lenvatinib therapy.
Footnotes
Acknowledgments
The authors thank the patients, their families, the investigators, and the teams who participated in this trial. This study was funded by Eisai, Inc. Editorial assistance was provided by Oxford PharmaGenesis, Inc., and was funded by Eisai, Inc. This article was previously presented in part at the 18th European Cancer Congress (ECC) Annual Meeting, Vienna, Austria, September 25–29, 2015.
Author Disclosure Statement
N.K. received honoraria and grant support from Eisai, Inc., and received research funding from ONO, and Boehringer-Ingelheim Japan. B.R. served as an advisory board member for Eisai, Inc. M.S. received grants from Exelixis, Eisai, Inc., Bayer. A.O.H. received research funding from Eisai, Inc. M.H.T. received consulting/honoraria from Eisai, Inc., and ONYX. D.L. is an employee of Eisai, Inc. C.E.D. is an employee of Eisai, Inc. E.K.L. served as an advisory board member for Eisai, Inc. S.-B.K. received research funding from Novartis, Kyowha Kirin. M.T. received grants/fees from Eisai, Inc., Boehringher-Ingelheim, and honoraria from Merck-Serono, and BMS.