
Abstract
Objective:
The aim of this study was to validate the American Thyroid Association (ATA) sonographic risk assessment of thyroid nodules.
Methods:
The ATA sonographic risk assessment was prospectively applied to 206 thyroid nodules selected for ultrasound-guided fine-needle aspiration (US-FNA), and analyzed with The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC), as well as surgical pathology for the subset undergoing surgical excision.
Results:
The analysis included 206 thyroid nodules averaging 2.4 cm (range 1–7 cm; standard error of the mean 0.07). Using the ATA US pattern risk assessment, nodules were classified as high (4%), intermediate (31%), low (38%), and very low (26%) risk of malignancy. Nodule size was inversely correlated with sonographic risk assessment, as lower risk nodules were larger on average (p < 0.0001). Malignancy rates determined by cytology/surgical pathology were high 100%, intermediate 11%, low 8%, and very low 2%, which were closely aligned with ATA malignancy risk estimates (high 70–90%, intermediate 10–20%, low 5–10%, and very low 3%). ATA US pattern risk assessment also appropriately predicted the proportion of nodules classified as malignant or suspicious for malignancy through TBSRTC classification—high (77%), intermediate (6%), low (1%), and very low 0%—as well as benign TBSRTC classification—high (0%), intermediate (47%), low (61%), and very low (70%) (p < 0.0001). Malignancy rates of surgically excised, cytologically indeterminate nodules followed ATA sonographic risk stratification (high 100%, intermediate 21%, low 17%, and very low 12%; p = 0.003).
Conclusion:
This prospective study supports the new ATA sonographic pattern risk assessment for selection of thyroid nodules for US-FNA based upon TBSRTC and surgical pathology results. In the setting of indeterminate cytopathology, nodules categorized as atypia of undetermined significance/follicular lesion of undetermined significance with ATA high-risk sonographic patterns have a high likelihood of being malignant.
Introduction
T
Sonographic features of thyroid nodules that have been frequently associated with malignancy include microcalcifications, taller-than-wide shape, marked hypoechogenicity, and irregular margins, while those that have a high specificity for benignity include simple cysts and spongiform appearance. Previous US classifications (i.e., Thyroid Imaging Reporting and Data Systems) have been proposed to facilitate predicting cancer risk. However, no consistent system is widely used in clinical practice. A meaningful and concise picture chart was provided in the ATA guidelines and gave an estimated malignancy risk for each pattern category demonstrating high (70–90%), intermediate (10–20%), low (5–10%), and very low (<3%) suspicion and benign (<1%) patterns (Fig. 1). Specific malignancy risk assessment for each US group was derived from a task force of specialists with complementary expertise (including endocrinology, surgery, radiology, pathology, oncology, and epidemiology) from the ATA (1).
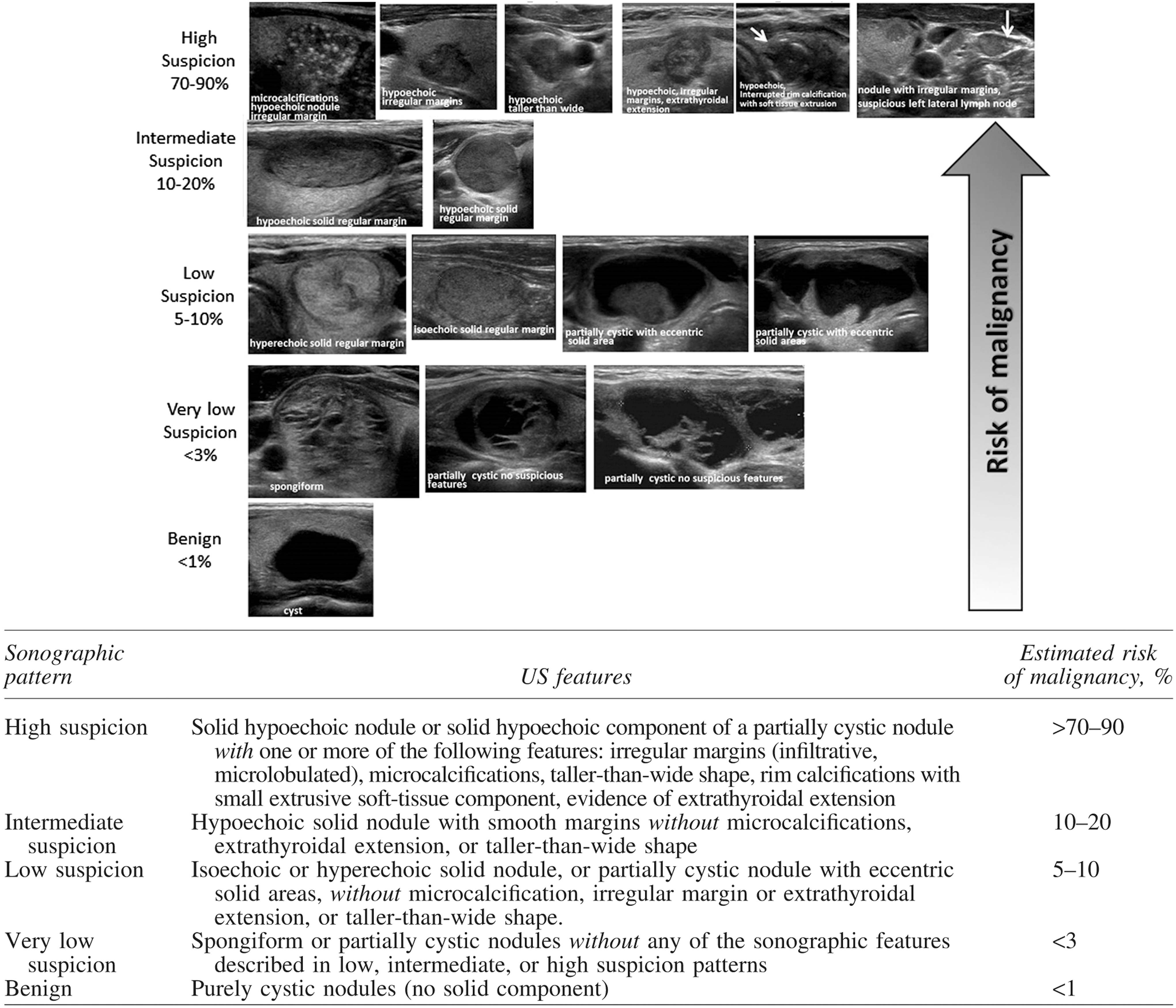
American Thyroid Association nodule sonographic patterns and risk of malignancy. From the 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer (1), with permission.
This study sought to investigate sonographic risk-pattern estimates in a prospective manner to bolster confidence in the ATA recommendations among practicing clinicians and to investigate its utility specifically in the subset of cytological indeterminate nodules.
Methods
This prospective study was approved by the Institutional Review Board (IRB) of the University of Cincinnati. All patients provided informed consent.
Patients
From March 2015 to May 2016, 199 consecutive patients with thyroid nodules consented to US-FNA and study inclusion. Patients were included in this prospective study if they had a dominant or suspicious nodule seen on office US and were recommended to undergo US-FNA. Exclusion criteria included patients with known thyroid malignancy or previous benign biopsy and those who did not meet the criteria for biopsy.
US and FNAB
Patients underwent an office US using a high resolution machine (GE Logiq e; GE Healthcare, Chicago, IL). Real-time US was performed by the senior author (D.L.S.), and nodules were stratified using sonographic patterns, as described and published in the 2015 ATA guidelines (Fig. 1) (1). Nodules were classified into the best fit category of high, intermediate, low, very low, or benign based on specific sonographic patterns as described (Fig. 1). US-FNA was performed of the target nodule by the same clinician using three to four separate passes with a 22- to 25-gauge needle utilizing capillary and aspiration techniques. First-pass samples (capillary) were immediately placed on glass slides and alcohol fixed. Remaining aspirate samples were placed into ThinPrep® CytoLyt® solution for liquid preparation.
Cytology results were reported based upon The Bethesda System for Reporting Thyroid Cytopathology (BSRTC; i.e. benign, atypia of undetermined significance/follicular lesion of undetermined significance (AUS/FLUS), follicular neoplasm/Hürthle cell neoplasm (FN/HN), suspicious for malignancy (SFM), malignant, and mon-diagnostic) and reported by trained cytopathologists at the authors' institution (1).
Surgery
Sixty-four patients with cytology deemed malignant, indeterminate, or benign with large nodules underwent surgical excision with subsequent permanent final histological diagnosis. The index nodule(s) undergoing US-FNA was/were specifically assessed as benign or malignant in these cases.
Data and statistical analysis
The frequency distribution in the different sonographic risk categories was compared using a chi-square test. Analysis was performed using JMP-SAS (SAS Institute, Cary, NC). The significance level was set at p < 0.05. A malignant or benign diagnosis was made on FNA cytology or surgical pathology. Data without a clear diagnosis of malignant or benign (i.e. AUS/FLUS, FN/HN) were excluded from determining malignancy rates.
Results
In total, 199 patients (157 female) were included in the study. From the 199 patients, 211 nodules were seen and evaluated further with US and biopsy. Five nodules were excluded due to incomplete data, withdrawal of consent, or lack of follow-up. Of the remaining 206 nodules, the nodule size ranged from 1 to 7 cm, with a mean size of 2.4 ± 1.1 cm (Table 1). There was an inverse correlation between the size of the nodule and the ATA sonographic risk assessment category (p < 0.0001) such that nodules that were stratified in the lower risk of malignancy categories were larger on average (Table 1).
p < 0.0001.
ATA, American Thyroid Association; SFM, suspicious for malignancy; AUS, atypia of undetermined significance; FLUS, follicular lesion of undetermined significance; FN, follicular neoplasm; HN, Hürthle cell neoplasm; Non-DX, non-diagnostic.
The distribution of nodules classified by ATA sonographic risk pattern were: high (4%), intermediate (31%), low (38%), very low (26%), and benign (0%; Table 1). The distribution of TBSRTC classification varied significantly by ATA sonographic risk assessment (p < 0.0001; Table 1). The proportion of cytological malignant or SFM correlated with sonographic risk pattern—high (77%), intermediate (6%), low (1%), and very low 0%—or cytological benign—high (0%), intermediate (47%), low (61%), and very low (70%) suspicion (Table 1).
There were 65 nodules that were surgically removed and used for analysis (Table 2). Of the nodules removed for permanent pathology, 44 were diagnosed as benign, 13 were classic papillary thyroid carcinoma (PTC), five were follicular variant PTC (FvPTC), one was a Hürthle cell variant PTC, one was a follicular carcinoma, and one was a renal cell carcinoma (Table 3). There were a total of 21 malignant nodules, resulting in a malignancy rate of 32% (21/65). The malignancy rates determined by cytology and/or permanent pathology (malignant vs. benign) varied by risk-assessment category: high 100%, intermediate 11%, low 8%, and very low 2% (p < 0.0001; Table 4). These were closely aligned with the ATA estimated risk of malignancy: high (70–90%), intermediate (10–20%), low (5–10%), and very low (<3%) suspicion (Table 4).
FvPTC, follicular variant papillary thyroid carcinoma; HPTC, Hürthle cell variant papillary thyroid carcinoma; PTC, classic papillary thyroid carcinoma; FTC, follicular thyroid carcinoma; RCC, renal cell carcinoma.
Indeterminate nodules include cytologic diagnosis of AUS/FLUS, FN/HN, and SFM.
There were 71 nodules that were cytologically indeterminate (AUS/FLUS, FN/HN, or SFM). Of these, 52 nodules were surgically excised for pathologic diagnosis (AUS 39, FLUS 1, FN/HN 6, and SFM 5), the majority of which were AUS/FLUS (Table 4). The malignancy rates of the surgically excised indeterminate nodules according to the sonographic risk assessment category were high 100%, intermediate 21%, low 17%, and very low 12% (p = 0.003; Table 4). Of the 40 nodules in the AUS/FLUS subgroup, seven nodules were malignant (7/40; 18%). The malignancy rates of the surgically excised AUS/FLUS nodules according to the sonographic risk assessment category were high 100%, intermediate 14%, low 13%, and very low 12% (p = 0.003; Table 4). Of the 19 indeterminate nodules that were not surgically excised, one nodule was high, five were intermediate, four were low, and nine were very low suspicion on US.
Discussion
Overall malignancy rates determined from cytology or surgical pathology were closely aligned with the ATA estimated risks of malignancy based upon sonographic patterns defined in the 2015 ATA guidelines (1). ATA sonographic suspicion patterns stratified appropriately. The majority of high suspicion pattern nodules were classified as malignant or SFM, and the majority of low and very low suspicion pattern nodules were classified as benign. Additionally, high-risk suspicion patterns in cytological indeterminate nodules were highly predictive of malignancy.
The reported findings must be interpreted with known limitations. One of the main limitations of this study is that all patients were seen and sonographically stratified by one physician, potentially limiting the generalizability of the results. Recent meta-analysis confirmed that operator experience is correlated with accurate evaluation of sonographic interpretation (5). Furthermore, the results show that the diagnosis of AUS/FLUS category appears evenly distributed at 22–30% across all ATA sonographic risk patterns studied, which is higher than the recommended usage of this category of 7% (6). The high rate of AUS/FLUS diagnosis in our study may limit the reproducibility of these results in future studies. There is evidence that suggests that the AUS/FLUS cytologic category has marked variability in incidence (0.7–18%) (7). After the implementation of TBSRTC in 2009, there has been a noted increase in the diagnosis of AUS/FLUS (8,9). This could partially explain why we observed a high proportion of AUS/FLUS in the low and very low categories. Finally, the risks prospectively calculated were for those patients who underwent FNA and did not include patients who underwent sonography with observation only, limiting applicability to an entire population.
In this study, malignancy rates were within or close to the given range described in the ATA guidelines for each sonographic risk category. In the high-risk category, the ATA guidelines predicted a malignancy risk of 70–90%, an estimated figure derived from high-volume outcome studies and previous classification systems (1,3,4,10). Multiple retrospective studies have established that the presence of marked hypoechogenicity, irregular margins, microcalcifications, and a taller-than-wide shape are frequently associated with malignancy (3,10 –12). A recent study reported that even in sub-centimeter thyroid nodules, the presence of microcalcifications and a taller-than-wide shape were independent predictors of aggressive behaviors such as extrathyroidal extension and lymph node metastasis (13). Using combinations of these US features was predictive of malignancy in this study.
In the intermediate suspicion group, the malignancy rate was 11%, which is within the ATA estimated range of 10–20%. This figure is similar to a study by Ito et al. reporting a 16.8% malignancy rate for nodules that were described as “borderline” on US (i.e., hypoechoic solid and regular-shaped without the presence of microcalcifications, extrathyroidal extension, and taller-than-wide shape) (14). The low suspicion group malignancy rate was 8%, which is within the estimated 5–10% range in the guidelines. This group included hyperechoic/isoechoic solid or partially cystic nodules. The ATA malignancy estimates were in part derived from a study by Lee et al. that reported a 5.4% malignancy rate for partially cystic nodules (15). Specifically, the authors were able to report that the eccentric positioning of the solid component in partially cystic nodules was an indicator of malignancy, which is a detail that is included in the ATA guidelines (Fig. 1). Partially cystic nodules without suspicious features or an eccentric solid component are downgraded to a <3% very low suspicion group. The very low suspicion group includes nodules that can also appear spongiform, which is a pattern of benignity supported by many investigators (3,15,16). Following these guidelines, this study showed that nodules placed in the very low risk category had a malignancy risk of 2%, validating the estimate provided by ATA guidelines of <3%.
Categories for sonographic patterns were correlated with TBSRTC diagnosis. The majority of the low and very low suspicion patterns were associated with benign cytology, whereas the majority of nodules that were high suspicion were SFM or malignant on cytopathology. Nodules that fell in the intermediate suspicion group had representation from all six TBSRTC diagnoses (Table 1). Overall, these results are congruent with a recent study by Lee et al. that compared US diagnosis to cytological diagnosis (17). The authors found a high correspondence between US categories (“benign,” “probably benign,” and “malignant”) and cytologic diagnosis using TBSRTC. Similarly, their intermediate suspicion group had cytologic diagnoses from five of the six TBSRTC categories, and their high-risk US diagnosis was mostly associated with SFM or malignant cytology (17).
The findings in this study demonstrate that high and intermediate suspicion patterns appear most commonly associated with classical PTC, especially when microcalcifications are present (Table 3) (1,11,12,18). This is in concordance with Kim et al., who showed that high-risk appearances on US were characteristic of PTC (11). The authors further noted that tiny, punctate microcalcifications were correlated with psammoma bodies, which are often seen on histopathology of classical PTC. High and intermediate suspicion patterns may also be commonly associated with non-encapsulated, partially encapsulated, or invasive encapsulated FvPTC (19,20). The presence of high-risk US features (i.e., taller-than-wide shape, infiltrative margin, marked hypoechogenicity, and microcalcifications) in some FvPTC can suggest more aggressive behavior than the same histopathologic tumors without high-risk patterns (19,20). However, most follicular pattern cancers (FvPTC and FTC) have low and intermediate suspicion patterns (20 –22). It is suspected that some intermediate risk patterns can represent encapsulated minimally invasive or noninvasive FvPTC (NIFTP), which is often cytologically categorized as AUS, FN, or SFM (19,20,23 –25). Hahn et al. specifically evaluated NIFTP nodules and found common US features of NIFTP to be solid, well circumscribed, and absent of microcalcifications. This fits into the category of intermediate suspicion (23).
Cytologically indeterminate nodules can have an estimated malignancy rate that ranges from 14% to 70% (1,26 –30). Sonography can help subcategorize nodules with indeterminate cytology for decision making and surgical planning (2,3,31 –33). It was found that high suspicion patterns in cytologically indeterminate nodules were highly predictive of malignancy. This is consistent with other studies showing a high positive predictive value of US in this cytological subset (27 –29,32) and furthermore supports triage to surgical excision in accordance with the ATA guidelines (1). Previous reports have found that AUS/FLUS diagnosed nodules that exhibited high-risk suspicion patterns (specifically taller-than-wide shape and markedly hypoechoic) were found to be malignant after surgery (27,28). Similarly, Moon et al. demonstrated that nodules with a FNA diagnosis of SFM combined with suspicious sonographic features had a malignancy rate of 94.9% (32). Incorporating the findings of this study and the supporting literature, in the setting of indeterminate nodules, the presence of sonographic high suspicion patterns may obviate the need for molecular testing, given the elevated pretest risk of malignancy.
This study validates the estimated likelihood of malignancy for each of the established sonographic risk groups published in the 2015 ATA guidelines. It was prospectively found that the sonographically estimated risk of malignancy for nodules undergoing US-FNA was closely aligned with the actual risk. Of particular interest, in setting of an AUS/FLUS indeterminate cytologic diagnosis, a high suspicion sonographic pattern predicted a high likelihood of malignancy and therefore supports surgical management. Results from this study are important for clinicians who wish to adopt the risk assessment from the ATA guidelines based on sonographic findings and can facilitate counseling and decision making in a clinical setting. Future directions of research should encompass inclusion of a higher number of nodules to determine if sonographic suspicious features can predict histopathologic subgroups (i.e., cancer variants) and behavior of specific tumors.
Footnotes
Author Disclosure Statement
No competing financial interests exist.