
Abstract
Background:
The programmed cell death-1 (PD-1) pathway is a novel therapeutic target in immune checkpoint therapy for cancer. It consists of the PD-1 receptor and its two ligands, programmed death-ligand 1 (PD-L1) and programmed death-ligand 2 (PD-L2). Nivolumab is an anti-PD-1 monoclonal antibody approved for malignant melanoma, advanced non–small cell lung cancer, and advanced renal cell carcinoma in Japan. Thyrotoxicosis and hypothyroidism have both been reported in international Phase 3 studies and national post-marketing surveillance of nivolumab in Japan.
Methods:
This study analyzed five consecutive cases with thyroid dysfunction associated with nivolumab therapy. Second, it examined the mRNA and protein expressions of PD-L1 and PD-L2 by reverse transcription polymerase chain reaction and Western blotting.
Results:
All patients were diagnosed with painless thyroiditis. Thyrotoxicosis developed within four weeks from the first administration of nivolumab and normalized within four weeks of onset in three of the five patients. Hypothyroidism after transient thyrotoxicosis developed in two patients, and preexisting hypothyroidism persisted in one patient. The other two patients were treated with glucocorticoids and discontinued nivolumab therapy for comorbid adverse events. One did not develop hypothyroidism, and the other developed mild, transient hypothyroidism. In addition, it was verified that normal thyroid tissue expresses PD-L1 and PD-L2 mRNA and those proteins.
Conclusions:
In the present cases, nivolumab-induced thyrotoxicosis seemed to be associated with painless thyroiditis, while no patient with Graves' disease was observed. A transient and rapid course with subsequent hypothyroidism was observed in nivolumab-induced thyroiditis. In addition, it was verified that PD-L1 and PD-L2 are expressed in normal thyroid tissue. This suggests that nivolumab therapy reduces immune tolerance, even in normal thyroid tissue, and leads to the development of thyroiditis. Treating thyrotoxicosis with only supportive care and considering levothyroxine replacement therapy once subsequent hypothyroidism occurs is proposed. Further investigations are required to confirm whether glucocorticoid therapy and discontinuation of nivolumab therapy prevent subsequent hypothyroidism.
Introduction
I
The first approved drug was ipilimumab, a mAb against CTLA-4. Ipilimumab induces several kinds of endocrine-related adverse events, including hypophysitis (8) and thyroid-related adverse events (9). In an international Phase 3 study for malignant melanoma, the frequency of hypopituitarism was 2.3%, hypophysitis was 1.5%, hypothyroidism was 1.5%, and thyrotoxicosis was not reported (10). In national post-marketing surveillance in Japan, the frequency of hypopituitarism was 2.0%, hypophysitis was 1.2%, and hypothyroidism was 1.6%. Thyrotoxicosis was not reported (11).
The PD-1 pathway was the next clinical target. It consists of the PD-1 receptor and its two ligands, programmed death-ligand 1 (PD-L1) (12) and programmed death-ligand 2 (PD-L2) (13). Nivolumab is a mAb against PD-1 that is approved to treat malignant melanoma, advanced non–small cell lung cancer, and advanced renal cell carcinoma in Japan as of August 31, 2016. Moreover, it was recently reported that nivolumab therapy is effective for patients with various other malignancies, such as Hodgkin's lymphoma (14) and squamous-cell carcinoma of the head and neck (15). In international Phase 3 studies for malignant melanoma (16) and non-squamous non–small cell lung cancer (17), the frequency of hypothyroidism was 5.6% and 6.6%, and thyrotoxicosis (described as hyperthyroidism in the literature) was 1.9% and 1.4%, respectively, while hypopituitarism and hypophysitis were not reported. In national post-marketing surveillance in Japan, the frequency of hypopituitarism was 0.2%, hypophysitis was 0.1%, hypothyroidism was 2.6%, and thyrotoxicosis (described as hyperthyroidism in the literature) was 1.3% (18). Pituitary-related adverse events occurred more frequently with ipilimumab than they did with nivolumab, but thyroid-related adverse events were more common with nivolumab. Moreover, thyrotoxicosis was only reported with nivolumab.
Orlov et al. reported that 6/10 patients who received anti-PD-1 mAb therapy developed transient thyrotoxicosis with subsequent hypothyroidism, and the other 4/10 patients developed only hypothyroidism (19). More recently, de Filette et al. observed 99 patients treated with pembrolizumab, anti-PD-1 mAb, of which 76 patients received prior ipilimumab therapy. In their cohort, thyrotoxicosis occurred in 12 patients, of which nine patients developed subsequent hypothyroidism (20). Interestingly, thyrotoxicosis was also reported in their study, and subsequent hypothyroidism was severe. However, regarding nivolumab in the clinical setting, data on thyroid-related adverse effect have been limited to three case reports (21 –23).
An association between the PD-1 pathway and thyroid cancer has been previously reported (24,25), but the role of PD-1 on the thyroid gland has not been clarified. To elucidate the role of PD-1 on the thyroid gland, findings from studies of PD-1 pathway blockade therapy are important. The present study reports a case series of nivolumab-associated thyroid dysfunction and the results on PD-L1 and PD-L2 mRNA and protein expression in normal thyroid tissue. It also discusses the clinical features and potential mechanisms.
Materials and Methods
Patients
The medical records were collected for five consecutive patients at the Department of Diabetes, Endocrinology, and Nutrition of Kyoto University Hospital who developed thyrotoxicosis during nivolumab therapy between September 2014 and May 2016. Their clinical course was examined from the first administration of nivolumab to 24 weeks afterwards.
Assays
Serum values of free triiodothyronine (fT3), free thyroxine (fT4), and thyrotropin (TSH) were measured using electrochemiluminescent immunoassays (Elecsys-FT3 II kit, Elecsys-FT4 kit, and Elecsys-TSH kit, respectively; Roche Diagnostics, Mannheim, Germany). The reference ranges were 2.33–4.00 pg/mL, 0.880–1.620 ng/dL, and 0.500–5.000 μIU/mL, respectively. Levels of antithyroid peroxidase antibodies (TPOAbs), antithyroglobulin antibodies (TgAbs), and antithyrotropin receptor antibodies (TRAbs) were also measured using electrochemiluminescent immunoassays (Elecsys Anti–TPO kit, Elecsys Anti–Tg kit, and Elecsys Anti–TSHR kit, respectively; Roche Diagnostics).
RNA extraction and reverse transcription polymerase chain reaction
Samples of normal thyroid tissue were obtained from thyroidectomy specimens for thyroid cancer. This study was approved by the Institutional Review Board and Ethics Committee of Kyoto University Graduate School of Medicine, and was conducted in accordance with the principles of the Declaration of Helsinki. Samples were stored at −80°C. Five samples of normal thyroid tissue derived from different donors were used. It was verified that TPOAb and TgAb were both negative in their sera, and that no lymphocyte infiltration was histopathologically observed in their thyroid tissues.
Three cell lines were used obtained from RIKEN BioResource Center (Ibaraki, Japan) through the National Bio-Resource Project of the Japanese Ministry of Education, Culture, Sports, Science, and Technology (Ibaraki, Japan): MCF7, derived from human breast carcinoma; HeLa, from human cervical carcinoma; and HTC/C3, from human thyroid undifferentiated carcinoma (26). All cells were authenticated with short tandem repeat profiling by RIKEN BioResource Center.
Total RNA was extracted using the RNeasy Mini kit plus RNase-free DNase Set (Qiagen, Venlo, Netherlands). Extracted total RNA was reverse transcribed with an oligo dT primer using SuperScriptIII First-Strand Synthesis SuperMix (Thermo Fisher Scientific, Waltham, MA). Concentrations of cDNA in each sample were measured with a Nanodrop-1000 spectrophotometer (Thermo Fisher Scientific).
Reverse transcription polymerase chain reaction (RT-PCR) was performed to verify gene expression of PD-L1 and PD-L2 using GAPDH as endogenous control. The Emerald Amp MAX PCR master mix was used (Takara Bio, Kusatsu, Japan) with 100 ng of cDNA as a template and 0.5 nM of primers (PD-L1 forward: 5′-GGC ATT CCA GAA AGA TGA GG-3′; PD-L1 reverse: 5′-GTC TTA CCA CTC AGG ACT TGA TG-3′; PD-L2 forward: 5′-CTC CTG CTA ATG TTG AGC CTG-3′; PD-L2 reverse: 5′-CAG GAA CGC TGA CGT TTG-3′; GAPDH forward: 5′-ACC ACA GTC CAT GCC ATC AC-3′; and GAPDH reverse: 5′-TCC ACC ACC CTG TTG CTG TA-3′). PCR was performed with 40 cycles of denaturation for 10 s at 98°C, annealing for 30 s at 58°C, and extension for 30 s at 72°C. Electrophoresis of PCR products was performed with 2% agarose gels.
Protein extraction and Western blotting
A protein lysate of normal thyroid tissue was obtained from BioChain (Newark, CA). MCF7, HeLa, and HTC/C3 cells were lysed in 100 μL radioimmunoprecipitation assay buffer (Nacalai Tesque, Kyoto, Japan), which contained 50 mM of Tris, 150 mM of sodium chloride, 1% Nonidet P40, 0.5% sodium deoxycholate, 0.1% sodium dodecyl sulfate, and protease inhibitor cocktail. Cell lysates were incubated for 30 min on ice, and centrifuged at 10,000 g for 10 min at 4 °C. The supernatant was collected as the sample containing whole cell protein. The protein concentration was evaluated using a Qubit 2.0 Fluorometer (Thermo Fisher Scientific).
Ten micrograms/lane of protein samples was electrophoresed in Bolt 4–12% Bis-Tris Plus Gels (Thermo Fisher Scientific), and the protein samples were transferred onto polyvinylidene difluoride membranes with iBlot Dry Blotting System (Thermo Fisher Scientific), according to the manufacturer's instructions.
The membranes were blocked with Blocking One (Nacalai Tesque), incubated with primary antibody overnight at 4°C, and then incubated with secondary antibody for 2 h at room temperature. All antibodies were diluted in Can Get Signal Immunoreaction Enhancer Solution (Toyobo, Osaka, Japan). The primary antibodies used were mouse monoclonal antibodies against PD-L1 and PD-L2 (catalog numbers 14-5983 and 14-5888, respectively; eBioscience, San Diego, CA), and a rabbit polyclonal antibody against β-actin (4967; Cell Signaling Technology, Danvers, MA). The secondary antibody used was a horseradish-peroxidase-conjugated goat anti-mouse IgG1 and a goat anti-rabbit IgG (1070-05 and 4030-05, respectively; Southern Biotech, Cambridge, United Kingdom).
The antibody–antigen complexes were detected by a chemiluminescent method with Chemi-Lumi One Super (Nacalai Tesque) in ImageQuant LAS 4000 (GE Healthcare, Chicago, IL).
Results
Case series
The characteristics of the five patients are shown in Table 1. Three patients had malignant melanoma, one had lung cancer, and one had breast cancer. (The patient with breast cancer requested nivolumab therapy, which was approved by the Institutional Review Board and Ethics Committee of the Kyoto University Graduate School of Medicine.) The patients received nivolumab at 2 mg/kg every three weeks (for malignant melanoma and breast cancer) or 3 mg/kg every two weeks (for lung cancer) by intravenous infusion. No patient had received prior treatment with other immune checkpoint inhibitors.
NA, not available; TPOAb, antithyroid peroxidase antibody; TgAb, antithyroglobulin antibody; TRAb, antithyrotropin receptor antibody; DAV-feron, dacarbazine, nimustine, vincristine, and interferon-β; UFT, tegafur + uracil; CDGP + GEM, nedaplatin + gemcitabine; CBDCA + PAC, carboplatin + paclitaxel; S-1, tegafur + gimeracil + oteracil.
All patients were diagnosed with painless thyroiditis; the thyrotoxicosis phase was transient, and TRAb test results at the onset of thyrotoxicosis were negative (patient 5 was not tested). The results of TPOAb and TgAb tests at the onset of thyrotoxicosis were double-positive in three patients and double-negative in one patient (patient 5 was not tested). The onset of thyrotoxicosis occurred from 12 to 119 days after the first administration of nivolumab; three patients developed thyrotoxicosis within four weeks. Normalization of thyroid function was confirmed 13–57 days after the onset of thyrotoxicosis, and three patients improved within four weeks. Subsequent hypothyroidism occurred 24–42 days after the onset of thyrotoxicosis in four patients (patient 2 did not develop hypothyroidism).
The clinical course, including thyroid function test results and details about levothyroxine (LT4) replacement therapy, is summarized below and in Figure 1.
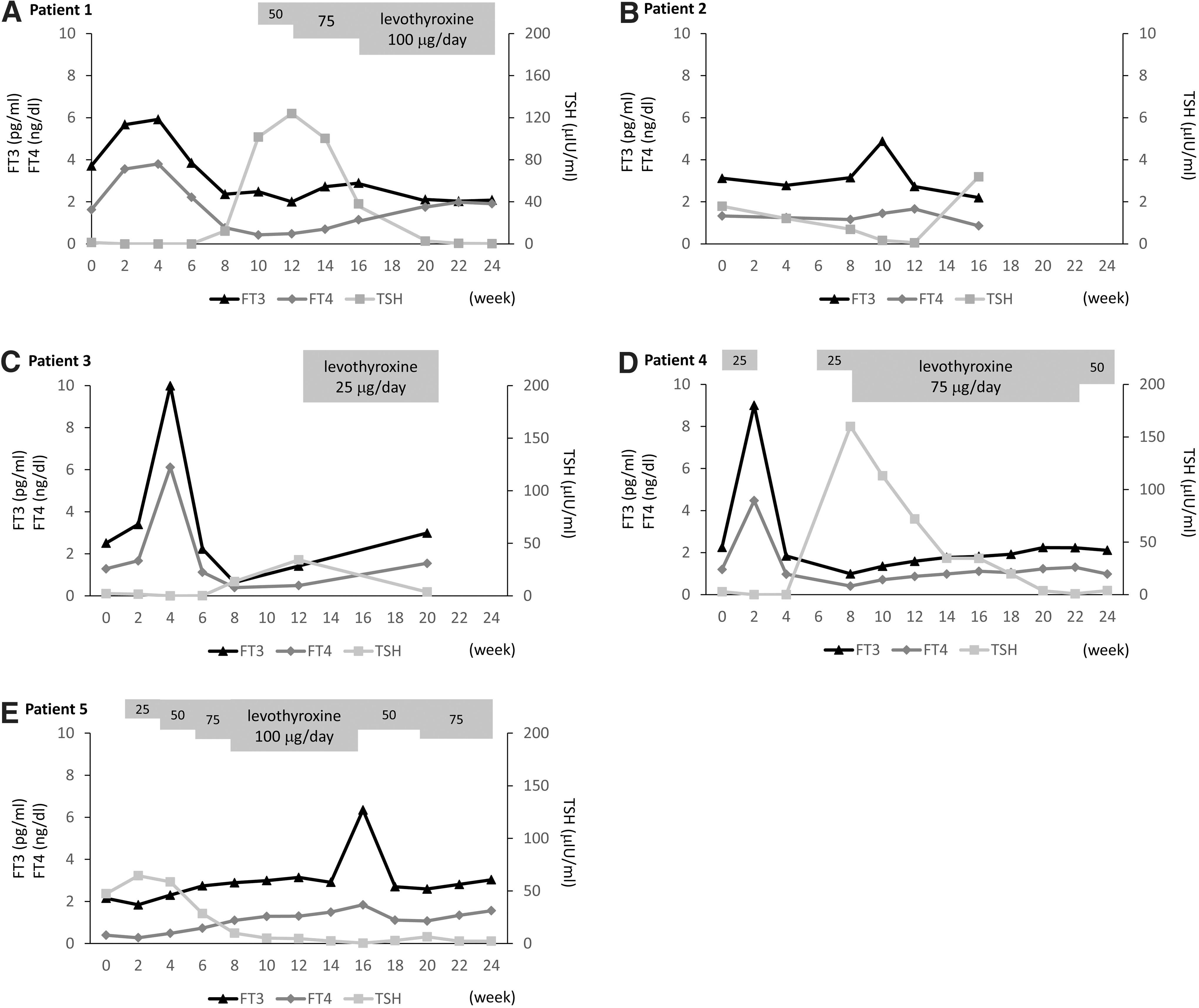
Clinical courses of patients 1–5
Patient 1: 61-year-old woman
Before nivolumab therapy, her serum fT3 was 3.71 pg/mL, fT4 was 1.630 ng/dL, and TSH was 1.360 μIU/mL. Asymptomatic thyrotoxicosis developed two weeks after the first administration, and peaked at four weeks. At four weeks, fT3 was 5.92 pg/mL, fT4 was 3.800 ng/dL, and TSH was 0.013 μIU/mL. fT3 and fT4 normalized at six weeks, and then TSH levels increased. LT4 replacement therapy was initiated at 12 weeks. The dose was gradually increased to 100 μg/day. Nivolumab therapy had been continued during the entire period.
Patient 2: 72-year-old man
Before nivolumab therapy, his serum fT3 was 3.12 pg/mL, fT4 was 1.330 ng/dL, and TSH was 1.790 μIU/mL. Thyrotoxicosis developed and peaked at 10 weeks. At that time, fT3 was 4.88 pg/mL, fT4 was 1.450 ng/dL, and TSH was 0.165 μIU/mL. He had hypotension and QT prolongation at 10 weeks and developed shock at 13 weeks. He was promptly diagnosed with isolated ACTH deficiency through laboratory testing. He was treated with 300 mg/day of hydrocortisone for the first three days and 20–30 mg/day of prednisolone for the next two weeks. He required maintenance therapy consisting of 10 mg/day of hydrocortisone and 0.25 mg/day of dexamethasone. Nivolumab therapy was discontinued at 10 weeks. Despite treatment, TSH levels did not increase, and LT4 replacement was not required. His thyroid function was stable at 16 weeks. He was subsequently transferred to another hospital for continuing supportive care.
Patient 3: 79-year-old woman
Before nivolumab therapy, her serum fT3 was 2.51 pg/mL, fT4 was 1.290 ng/dL, and TSH was 2.180 μIU/mL. Asymptomatic thyrotoxicosis developed and peaked at four weeks. At that time, fT3 was 9.99 pg/mL, fT4 was 6.120 ng/dL, and TSH was 0.022 μIU/mL. fT3 and fT4 normalized at six weeks, and then TSH levels increased. She developed idiopathic thrombocytopenic purpura at six weeks, for which she received glucocorticoids (125–250 mg/day of methylprednisolone for the first two days and 40 mg/day of prednisolone for the next three weeks), intravenous immunoglobulins, and romiplostim. Nivolumab therapy was discontinued at four weeks, and glucocorticoids were tapered off after four months. LT4 replacement was initiated at 12 weeks. The maintenance dose was 25 μg/day. Subsequently, she stopped LT4 replacement at 20 weeks and was euthyroid for more than eight months.
Patient 4: 66-year-old woman
This patient had taken 25 μg/day of LT4 for 20 years to treat Hashimoto's disease. Before nivolumab therapy, her serum fT3 was 2.25 pg/mL, fT4 was 1.200 ng/dL, TSH was 2.820 μIU/mL, TPOAb level was 29 IU/mL, and TgAb level was 182 IU/mL. Asymptomatic thyrotoxicosis developed and peaked at two weeks. At that time, fT3 was 9.00 pg/mL, fT4 was 4.470 ng/dL, and TSH was 0.013 μIU/mL. The TPOAb level increased to 258.0 IU/mL, and the TgAb level increased to 390.1 IU/mL. LT4 replacement was immediately discontinued. fT3 and fT4 normalized at four weeks, and then TSH levels increased. LT4 replacement was resumed at six weeks. The dose was gradually increased to 50–75 μg/day. Nivolumab therapy had been continued during the entire period.
Patient 5: 63-year-old man
Before nivolumab therapy, his serum fT3 was 2.15 pg/mL, fT4 was 0.393 ng/dL, TSH was 47.320 μIU/mL, and TPOAbs and TgAbs were both negative. His hypothyroidism was attributed to cervical irradiation therapy for lymph node metastasis from lung cancer one year ago. Nivolumab and LT4 replacement were initiated simultaneously. The dose of LT4 was gradually increased to 100 μg/day. While his thyroid function and general condition were stable, nevertheless asymptomatic thyrotoxicosis developed and peaked at 16 weeks. At that time, fT3 was 6.35 pg/mL, fT4 was 1.840 ng/dL, and TSH was 0.374 μIU/mL. The LT4 dose was temporarily decreased to 50 μg/day. fT3 and fT4 normalized at 18 weeks, and LT4 was subsequently increased to 75 μg/day. Nivolumab therapy had been continued during the entire period.
PD-L1 and PD-L2 expression in the thyroid gland
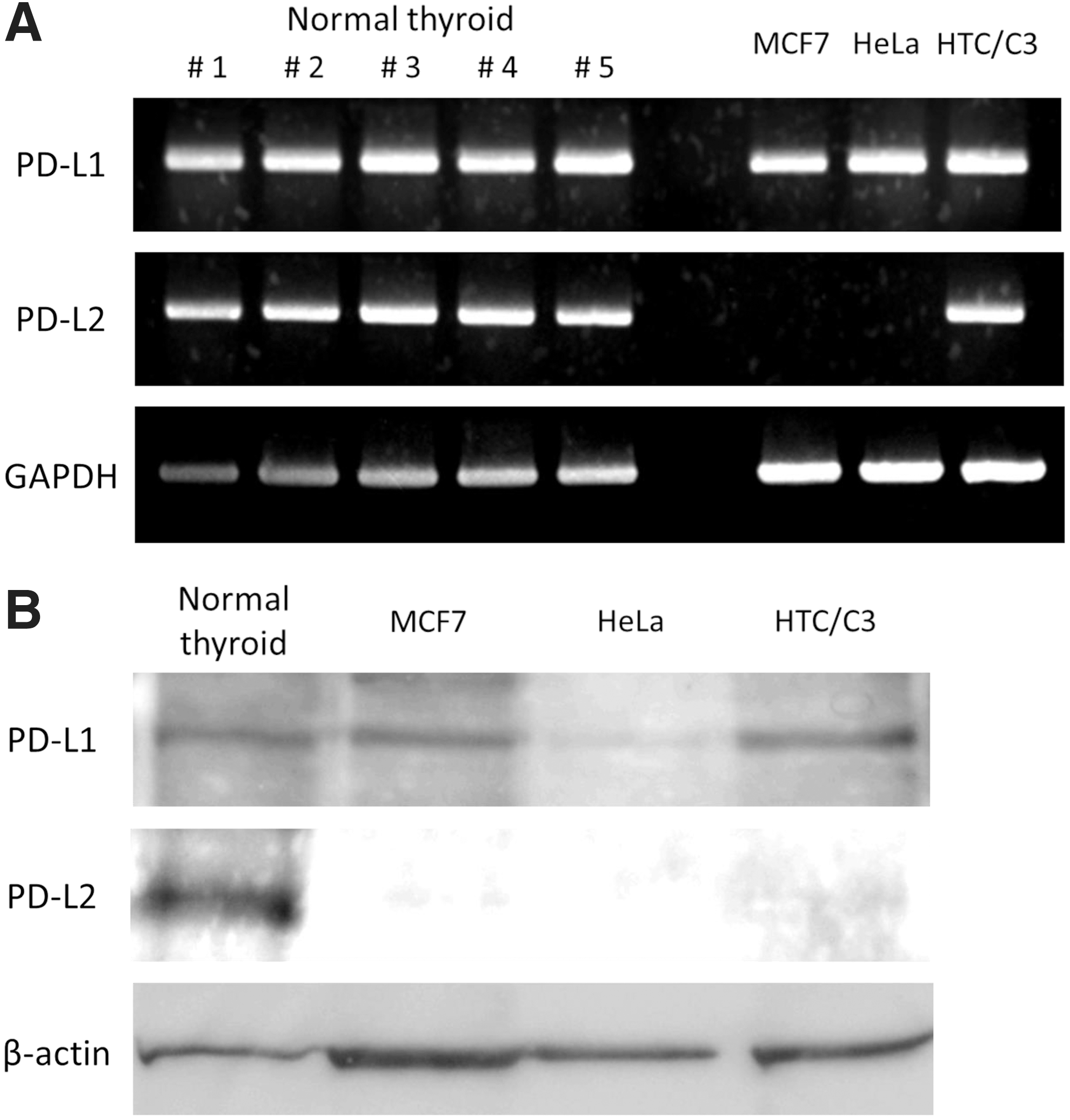
This study investigated PD-L1 and PD-L2 gene expression in normal thyroid tissue using RT-PCR. Five samples of normal thyroid tissue were used derived from different donors, MCF7 and HeLa as positive controls of PD-L1 (13, 27), and HTC/C3 as a model of the thyroid gland. The RT-PCR results showed that normal thyroid tissue and HTC/C3 expressed both PD-L1 and PD-L2 mRNA. PD-L1 mRNA was also expressed in MCF7 and HeLa, while PD-L2 mRNA expression was not observed (Fig. 2A).
(
The immunoblots showed that normal thyroid tissue, MCF7 cells, and HTC/C3 cells showed equivalent expression of PD-L1 protein, but HeLa cells showed relatively low expression as previously reported (27). The PD-L2 protein was expressed in normal thyroid tissue and weakly in HTC/C3 cells but not in MCF7 cells and HeLa cells (Fig. 2B).
Discussion
The present case series demonstrates that thyrotoxicosis induced by nivolumab is caused by painless thyroiditis in all cases. The thyrotoxic phase was transient in all five patients, and the TRAb results were negative in the four tested patients, which supports the diagnosis of painless thyroiditis. It is noteworthy that the patients tended to have a rapid course of the thyrotoxic phase. Thyrotoxicosis developed within four weeks of the first administration of nivolumab and normalized within four weeks of onset in three of five patients. Hypothyroidism after transient thyrotoxicosis developed in patients 1 and 4, and preexisting hypothyroidism persisted in patient 5. Hypothyroidism did not develop in patient 2, and patient 3 had mild, transient hypothyroidism. Notably, both patients 2 and 3 were treated with glucocorticoids, and nivolumab therapy was discontinued for comorbid adverse events.
Orlov et al. and de Filette et al. described thyrotoxicosis with subsequent hypothyroidism in their case series (19,20). Tanaka et al. reported two cases of thyrotoxicosis induced by nivolumab. One patient developed thyrotoxicosis with subsequent hypothyroidism. The other patient, who was treated with glucocorticoids and discontinuation of nivolumab, developed thyrotoxicosis but did not develop subsequent hypothyroidism (23). Taken together, these reports and the present cases suggest that the clinical features of nivolumab-induced thyrotoxicosis include the following characteristics: (i) it is appears to be caused by painless thyroiditis, whereas Graves' disease is not likely; (ii) the thyrotoxicosis can progress rapidly (weeks); and (iii) hypothyroidism commonly develops after thyrotoxicosis. In addition, severe subsequent hypothyroidism was not observed in patients in the present study who received glucocorticoid therapy or if nivolumab was discontinued, a finding that needs to be confirmed by further observations.
To investigate possible mechanisms underlying nivolumab-induced thyrotoxicosis, the study examined whether normal thyroid tissue expresses PD-L1 and/or PD-L2 mRNA and protein. PD-1 expression was not verified in the present study because PD-1 is the receptor expressed on lymphocytes (28), and no lymphocytic infiltration was histopathologically confirmed in the studied samples. PD-L1 mRNA and its protein were expressed in all tested samples, which is consistent with previous reports that a variety of organs express PD-L1 (29,30). PD-L2 protein expression was also detected in normal thyroid tissue and less in HTC/C3 cells. The result in HTC/C3 cells is supported by a report that anaplastic thyroid cancer expresses PD-L1 and PD-L2 (25) because HTC/C3 cells are derived from an undifferentiated human thyroid carcinoma. The level of PD-L2 expression in normal thyroid tissue appears to be relatively high.
To date, findings regarding the PD-1 pathway in the thyroid have been limited to malignant tumors (24,25,31) and the detection of a polymorphism in PD-L1 in Japanese patients with Graves' disease (32). To the best of the authors' knowledge, this is the first report showing that normal thyroid tissue expresses PD-L1 and PD-L2. Inoue et al. reported that high expression levels of PD-L1 and PD-L2 correlate with the response to nivolumab therapy in patients with malignant melanoma (33). In other words, blockade of the PD-1 pathway in tissues expressing PD-L1 and PD-L2 could enhance local immune activity. Thus, the present results on PD-L1 and PD-L2 expression suggest that nivolumab therapy reduces immune tolerance, even in normal thyroid tissue, and leads to the development of thyroiditis.
Painless thyroiditis often does not require permanent hormone replacement therapy. For example, overt hypothyroidism was only observed in 16.6% of patients with postpartum thyroiditis (34,35). Interestingly, nivolumab-induced thyroiditis commonly involves subsequent hypothyroidism, which is similar to other nivolumab-induced endocrinopathies, such as autoimmune diabetes (36) and ACTH deficiency (37,38), with regards to severity and persistency of the deficiency.
TPOAbs and TgAbs were positive in three of four patients tested. Their levels increased after nivolumab therapy in patient 4. These findings suggest that an abnormality in the PD-1 pathway is a possible mechanism contributing to the pathogenesis of Hashimoto's disease. It may be worthwhile investigating whether the PD-1 pathway is implicated in Hashimoto's disease requiring permanent hormone replacement therapy.
One strength of the present study is the short interval between thyroid function tests; thyroid function tests were performed almost every two weeks. Limitations include the inability to determine the incidence of thyroiditis and hypothyroidism induced by nivolumab because a sufficient number of cases could not be collected at the authors' institution, and the fact that the patients were all seen in the authors' department.
In conclusion, these cases suggest that nivolumab-induced thyrotoxicosis appears to be caused by painless thyroiditis, not by Graves' disease. A transient and rapid course with subsequent hypothyroidism was observed in nivolumab-induced thyroiditis. Treating thyrotoxicosis with supportive care is recommended, and levothyroxine should be administered once hypothyroidism is documented. Whether glucocorticoid therapy and discontinuation of nivolumab therapy prevent subsequent hypothyroidism needs to be confirmed by further observations.
Footnotes
Acknowledgments
We thank the medical staff in our department for providing clinical experience.
Author Disclosure Statement
The authors have nothing to disclose.