
Abstract
Background:
The 2015 American Thyroid Association guidelines acknowledged that “an active surveillance management approach can be considered as an alternative to immediate surgery” in patients with low-risk papillary thyroid carcinoma (PTC). The aim of this study was to determine the proportion of PTC that would meet the criteria for active surveillance and the surgeries and complications that could have been avoided.
Methods:
A total of 681 patients with thyroid cancer who underwent thyroid surgery from 2003 to 2012 were retrospectively reviewed. A decision-making framework for active surveillance was applied to patients with PTC in nodules measuring ≤1.5 cm on ultrasound. Patients were identified as suitable for active surveillance based on imaging and patient characteristics. These patients were reviewed for management and outcomes.
Results:
PTC was diagnosed based on fine-needle aspiration histology of Bethesda V or VI in thyroid nodules in 243 patients. Of these, 77 patients had nodules measuring ≤1.5 cm on ultrasound, and 56/77 (23%) patients met the criteria for surveillance: 15/243 (6%) patients met the criteria with a ≤1 cm size threshold, and 41/243 (17%) met the criteria with a 1.1–1.5 cm threshold. Of the 56 patients who met the criteria for active surveillance, 52 underwent total thyroidectomy, and four had a lobectomy. Forty-five (80%) patients had elective central nodal dissection, and 14 had nodal metastases on pathology (all <4 mm). Three patients had permanent complications from surgery, including vocal cord paralysis, hypoparathyroidism, and a chipped tooth from intubation. No patients died or had recurrent disease.
Conclusion:
Future programs in the United States should consider increasing the size threshold for active surveillance of PTC to 1.5 cm, since this will allow up to one quarter of patients to be eligible instead of only 6% with a 1 cm size threshold. Without an active surveillance program, the majority of patients with low-risk cancers have thyroidectomy and carry a small risk of permanent complications.
Introduction
P
The standard treatment for thyroid cancer is thyroid surgery. Serious and permanent surgical complications—hypoparathyroidism and vocal cord paralysis—are rare, but they are more common in surgeries performed by low-volume surgeons. Patients who have thyroid surgery may also require lifelong thyroid-replacement therapy and regular blood level monitoring. Given the risks of surgery and the potential indolent behavior, active surveillance has evolved as an alternative management for patients with small PTCs (5,6). A Japanese study compared 1179 patients with subcentimeter PTC on active surveillance with 974 patients after immediate surgery (7). In the active surveillance group, 2% of patients experienced tumor enlargement (>3 mm), and 0.5% had novel lymph node metastases. Recurrence was no higher in the surveillance group than it was in the immediate surgery group, and all cases were successfully treated. None of the patients had distant metastases, and none died of the disease. Given the safety of an active surveillance strategy, the 2015 American Thyroid Association guidelines acknowledged that “an active surveillance management approach can be considered as an alternative to immediate surgery” in patients with low-risk PTC (8).
A recommendation supporting the option of active surveillance is a radical shift in the field of thyroid cancer in the United States. However, the extent to which this recommendation will impact practice and potentially lead to a decrease in the number of thyroid surgeries for patients carrying small PTCs in the United States is unclear. To this end, the aim of this study was to determine, retrospectively, the proportion of thyroid cancers that would meet the criteria for active surveillance and the number of surgeries and complications that could have been avoided.
Methods
Study population
This is a retrospective study of 681 patients with thyroid cancer that underwent surgery over a decade between January 2003 and December 2012 at a tertiary care center in the United States. The medical records were reviewed to identify patients who would be eligible for active surveillance according to the Memorial Sloan Kettering Cancer Center (MSKCC) risk-stratified clinical decision-making framework (6). This study was approved by the Institutional Review Board and was compliant with the Health Insurance Portability and Accountability Act.
Risk-stratification categories
The criteria for the risk-stratified clinical decision-making framework are outlined in Table 1. Patients were classified as “ideal,” “appropriate,” or “inappropriate” candidates based on three sets of criteria: (i) tumor and ultrasound characteristics (size ≤1 cm, location of the tumor, suspicious cervical lymph nodes, molecular profile); (ii) patient characteristics (demographics, family history, willingness to participate); and (iii) medical team characteristics (experience and expertise of treating clinician and multidisciplinary team). For the purposes of this study, it was assumed that the cancers met the medical team treatment criteria and that eligible patients were willing to participate in surveillance if they were classified as either ideal or appropriate for surveillance.
Reference (6).
US, ultrasound; RLN, recurrent laryngeal nerve; FDG, fludeoxyglucose; PMC, papillary microcarcinoma; FNA, fine-needle aspiration.
Patients who would be considered for active surveillance were identified by excluding patients with histologies other than PTC, incidental cancers on pathology (not associated with a nodule on ultrasound), patients who did not have a preoperative thyroid cancer diagnosis on cytology (Bethesda I–IV), and patients with thyroid nodules on ultrasound >1.5 cm (Fig. 1). Although the published risk-stratification system only applies to size ≤1 cm to be eligible, the number of patients who would be eligible if size thresholds increased to 1.5 cm was also of interest because this size threshold was used in a study from Memorial Sloan Kettering Cancer Center (9).
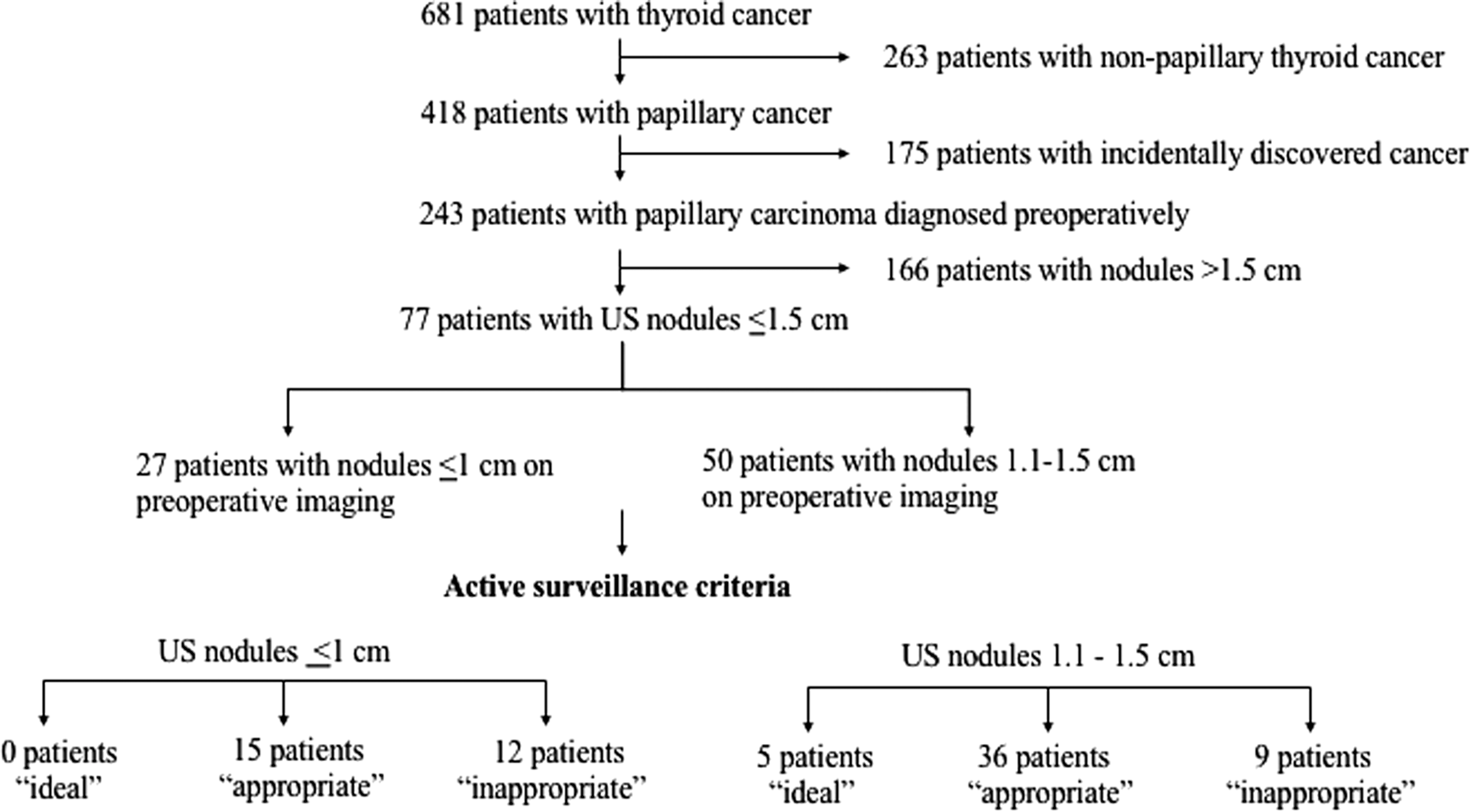
Flow chart of active surveillance criteria inclusion and exclusion.
From the eligible cohort, a radiologist reviewed available thyroid ultrasound images for size, subcapsular location adjacent to recurrent laryngeal nerve, extrathyroidal extension, and abnormal cervical lymph nodes. Finally, medical records were reviewed again for personal and family history of thyroid cancer and molecular profile (when available). Patients who met the age and ultrasound criteria for observation were then classified as either “ideal” or “appropriate” candidates.
Outcome measures and statistical analysis
The primary outcome of interest was the proportion of patients with thyroid nodules measuring ≤1 cm and 1.1–1.5 cm who would meet the criteria for active surveillance according to the risk-stratified clinical decision-making framework. Other outcomes of interest were the staging, treatment, and complications for patients who met the criteria for active surveillance. This provided insight into outcomes that could have been avoided without surgery.
Results
Study population
Of 681 patients with thyroid cancer, 418 (61%) had PTC at pathology (Fig. 1). Of these, 243/418 (58%) patients were diagnosed with thyroid cancer preoperatively based on fine-needle aspiration (FNA) histology of Bethesda V or VI in thyroid nodules. Of the 243 patients with a preoperative diagnosis of PTC, 77 (32%) had nodules measuring ≤1.5 cm on preoperative ultrasound, 27 (11%) had nodules ≤1 cm, and 50 (21%) had nodules measuring 1.1–1.5 cm.
Risk-stratification categories
Of the 27 patients with PTC measuring ≤1 cm on ultrasound, 12 patients were “inappropriate” for surveillance because of suspicious lymph nodes on ultrasound (n = 10) or a personal history of thyroid cancer (n = 2). Of the remaining 15 patients, none were “ideal” and 15 were “appropriate” for active surveillance. These patients represent 6% (15/243) of patients with PTC on cytology.
Among the 50 patients with nodules measuring 1.1–1.5 cm on ultrasound, nine patients were “inappropriate” for surveillance because of suspicious lymph nodes on ultrasound (n = 8) and subcapsular location (n = 1). Of the remaining 41 patients, five were “ideal” and 36 were “appropriate” for active surveillance. Thus, increasing the size threshold from 1 cm to 1.5 cm would allow an additional 16% (41/243) of patients with PTC on cytology to undergo active surveillance.
Treatment and outcomes
The treatment and outcomes for patients with PTC ≤1 cm on ultrasound who met the criteria for active surveillance are shown in Table 2. Total thyroidectomy with central lymph node dissection was performed in 13/15 (87%) patients. No patients had nodal metastases at surgery. Ultrasound underestimated tumor size in four (27%) patients, but the largest size discrepancy was only 2 mm, and the largest tumor on pathology was only 1.2 cm. There were no cases of death or recurrence, but one patient suffered a chipped tooth during intubation and developed a right breast hematoma from positioning during the procedure.
RAI, radioactive iodine.
The treatment and outcomes for patients with PTC measuring 1.1–1.5 cm on ultrasound who met the criteria for active surveillance are shown in Table 2. Total thyroidectomy was performed in 39/41 (95%) patients. Thirty-three (80%) patients had elective central lymph node dissections, which found 14 (34%) patients to have nodal metastases. The largest node was 4 mm. No patients had lateral neck nodes. Ultrasound underestimated tumor size in 11 (27%) patients. The largest size discrepancy was 6 mm, and the largest tumor on pathology was 2 cm. There were no cases of death or recurrence, but one patient had permanent vocal-cord paralysis, and one patient had permanent hypoparathyroidism.
Eighteen patients were excluded from active surveillance from both groups because of suspicious lymph nodes. Of the 10 patients with PTC ≤1 cm on ultrasound who were excluded, seven had metastatic disease at pathology. Of the eight patients with PTC measuring 1.1–1.5 cm on ultrasound, all eight had metastatic disease at pathology.
Discussion
Concerns of overdiagnosis and overtreatment have led to an approach of active surveillance management for patients with low-risk PTC as an alternative to immediate surgery. Active surveillance has been acknowledged as a possibility in the American Thyroid Association guidelines, and several institutions in the United States now offer it for select patients with small PTC (8). Despite the promise of this recommendation to tailor treatment intensity to the tumor prognosis for patients with small PTC, it was found that only 6% of patients with subcentimeter PTC on cytology would meet the criteria for active surveillance. When the threshold increased to 1.5 cm, one in four patients would be eligible. Without an active surveillance program, the majority of the patients had total thyroidectomy with a small risk of permanent complications.
There are three studies that recruited patients with low-risk PTC for active surveillance (9 –11). The two Japanese studies used a 1 cm size threshold and similar exclusion criteria. Sugitani et al. enrolled 230 patients over 17 years, and the group from Kuma Hospital enrolled 1235 patients over eight years (10,11). In contrast, the present study found that a 1 cm threshold would only have allowed 27 patients to be eligible for active surveillance in 10 years of thyroid cancer surgery. This is largely due to the fact that thyroid nodules <1 cm rarely undergo biopsy in the United States, as recommended by the American Thyroid Association and the Society of Radiologists in Ultrasound (8,12). For this reason, an abstract describing active surveillance at MKSCC used a tumor size of <1.5 cm to enroll 97 patients over 18 months (9). The present study shows that increasing the size threshold to 1.5 cm significantly increases eligible patients to one in four patients with cytology results showing PTC. Since the 10-year relative survival for thyroid cancers measuring 0.5–0.9 cm and 1.0–1.9 cm are the same after surgery (99.8%), 1.5 cm can be safely considered as the new size threshold for inclusion of future active surveillance trials (13).
The 2015 ATA guidelines have proposed performing a lobectomy instead of total thyroidectomy in patients with localized thyroid cancer measuring <1 cm, and that lobectomy is an option for cancers measuring between >1 cm and <4 cm (8). Almost all patients in the present study (52/56 measuring ≤1.5 cm) underwent total thyroidectomy. Permanent complications were seen in three (5%) patients, which included vocal-cord paralysis, hypoparathyroidism, and a chipped tooth from intubation. Similar complication rates were seen in 974 patients who chose immediate surgery over active surveillance (7). The immediate surgery group had two (0.2%) patients with permanent vocal-cord paralysis and eight (1.6%) patients with permanent hypoparathyroidism. There were also problems with postsurgical hematoma (0.5%) and surgical scar (8%). Limiting the surgery to partial thyroidectomy will reduce the rate of surgical complications and need for lifelong thyroid replacement. However, a surveillance program could avoid surgery and its risks and costs altogether.
The final decision of active surveillance versus surgery relies on what fits the patient's values and context. It is important that all patients with small PTC be offered the option of active surveillance head-to-head with surgery. Those who oppose active surveillance raise concerns about ultrasound underestimating the size of the tumor, missed nodal metastases, and the cost of surveillance. The present study found that ultrasound and pathology sizes of tumor differed by only several millimeters. Despite the majority of patients having elective central nodal dissection, only a quarter of patients had nodal metastases on pathology. Furthermore, the nodal metastases were micro-metastases (maximum size 4 mm). Finally, it has been argued that it is more cost-effective to perform a thyroidectomy upfront when the tumor is first detected, rather performing surveillance on patients who will ultimately require thyroidectomy (14). However, surgical complications and continued monitoring for recurrent disease should both be considered in cost-effective analyses. Currently, there are no such studies for small PTC in the United States, but a cost analysis considering the Japanese Health Care Insurance System found that the 10-year total cost of immediate surgery was 4.1 times more expensive than active surveillance (15).
There are several limitations to this study. First, this was a retrospective study that only included patients who had surgery. Although the authors' institution does not have a formal surveillance program, there could have been some patients who were observed for medical reasons. A larger proportion of patients with tumors 1.1–1.5 cm met the criteria for surveillance than did those with ≤1 cm tumors. This is not because smaller tumors are more aggressive, but because these small nodules are less likely to be biopsied unless there were other suspicious features such as abnormal lymph nodes. More than one third of subcentimeter PTC were excluded for suspicious lymphadenopathy. It was the presentations with abnormal lymph nodes that ultimately drove the decision to perform a FNA. Practices that biopsy subcentimeter thyroid nodules based on other criteria may have a higher proportion of subcentimeter PTCs meeting the criteria for observation. Finally, eligible patients may be may be underestimated by assuming that all patients were agreeable and that all medical teams were experienced with active surveillance.
In conclusion, active surveillance for patients with low-risk thyroid PTC is becoming an accepted option, given the problem of thyroid cancer overdiagnosis and overtreatment. Future programs in the United States should consider increasing the size threshold to 1.5 cm, since this will allow up to one quarter of patients to be eligible instead of only 6% with a 1 cm size threshold. Without an active surveillance program, the majority of patients with low-risk cancers undergo total thyroidectomy and carry a small risk of permanent complications.
Footnotes
Author Disclosure Statement
None of the authors has any financial disclosures.