
Abstract
Background:
Molecular testing of thyroid nodules is increasingly being utilized to guide clinical management decisions. RAS mutations are the most frequent mutations detected in the context of an indeterminate fine-needle aspiration (FNA) diagnosis. The term “noninvasive follicular thyroid neoplasm with papillary-like nuclear features” (NIFTP) was recently introduced to promote conservative management of tumors previously classified as noninvasive follicular variant of papillary thyroid carcinoma (FVPTC). This change in terminology was based on the indolent clinical behavior of these tumors and their molecular profile, which includes frequent RAS mutations. The aim of this study was to determine the percentage of RAS-mutant “carcinomas” that would now be classified as NIFTPs.
Methods:
A search was performed for cases with known activating RAS mutations in a database of 199 thyroid carcinomas that underwent molecular characterization as part of Profile:Oncopanel between July 2013 and July 2015. Cases of FVPTC were re-reviewed to identify tumors that now would be categorized as NIFTP. Preceding FNA diagnoses were recorded, and cases with an indeterminate FNA result (defined as a diagnosis of atypia/follicular lesion of undetermined significance, suspicious for follicular neoplasm, or suspicious for malignancy) were identified.
Results:
A total of 27 RAS-mutant thyroid tumors were identified. Fifteen (56%) cases had an NRAS mutation, nine (33%) had an HRAS mutation, and three (11%) had a KRAS mutation. Twenty-four (89%) cases had a preceding FNA, 19 (79%) of which had an indeterminate FNA diagnosis. The surgical resection specimen demonstrated FVPTC in 20 (74%) cases, classical type PTC in two (7%), solid variant of PTC in one (4%), and follicular thyroid carcinoma in four (15%). Of the 20 FVPTCs, 16 (80%) would now be classified as NIFTP. NIFTPs accounted for 59% of RAS-mutant carcinomas overall and 63% of RAS-mutant carcinomas with a prior indeterminate FNA diagnosis.
Conclusion:
NIFTPs accounted for more than half of RAS-mutant “carcinomas” in this cohort. In cases where clinical and sonographic data support a low-risk phenotype, these results suggest that a lobectomy should be considered as the initial surgical approach for a nodule with an indeterminate FNA diagnosis and a RAS mutation.
Introduction
A
The term “noninvasive follicular thyroid neoplasm with papillary-like nuclear features” (NIFTP) was recently introduced to recognize the indolent behavior of thyroid neoplasms previously classified as noninvasive follicular variant of papillary thyroid carcinoma (FVPTC) (7). The aim of this change in nomenclature is to decrease the overtreatment of indolent thyroid tumors and spare patients the anxiety of a cancer diagnosis (7 –10). NIFTPs, which have a very low metastatic potential and recurrence risk, predominantly harbor RAS mutations, though a smaller subset have been found to have the BRAFK601E mutation and PPARG and THADA fusions (7,9,11 –14). The majority of NIFTPs have been shown to be preceded by an indeterminate FNA result (15 –18). Based on the indolent behavior of NIFTPs, lobectomy instead of total thyroidectomy has been advocated (7,11). Lobectomy is required for NIFTPs both because NIFTP may be a precursor to more aggressive thyroid tumors and because histologic evaluation of the tumor is required to assess for infiltrative or invasive growth, that is, features that cannot be discerned on cytology and would exclude a diagnosis of NIFTP.
The extent of the initial surgery that should be performed for a nodule with an indeterminate cytologic diagnosis and a RAS mutation detected by molecular testing has not been established. In part, the decision is driven by the risk of malignancy associated with each Bethesda diagnostic category. In a recent publication by the American Thyroid Association (ATA) on the application of molecular profiling of thyroid nodules on perioperative decision making, the authors state that a nodule with a preceding AUS/FLUS, SFN, or SUS diagnosis on cytology and a molecular alteration found on molecular testing should usually prompt a single-stage total thyroidectomy due to the very high likelihood of malignancy, although lobectomy only may be appropriate for low-risk cancers (3). The emergence of NIFTP raises the question of whether detection of a RAS mutation should usually prompt lobectomy rather than total thyroidectomy as the initial surgical approach for nodules with low-risk clinical and radiologic features and an indeterminate FNA diagnosis. The aim of this study was to identify cases with known activating RAS mutations from a database of 199 thyroid carcinomas that underwent molecular characterization as part of Profile:Oncopanel to determine how many of these tumors would now be classified as NIFTPs.
Materials and Methods
Approval from the Brigham and Women's Hospital Investigation Review Board was obtained. A database of 199 thyroid carcinomas was reviewed from patients who underwent surgery and molecular characterization of their tumors as part of Profile:Oncopanel between July 2013 and July 2015. Oncopanel molecular testing was performed using formalin-fixed paraffin-embedded tissue or freshly frozen tissue. Tumor samples were digested in proteinase K overnight, and DNA was isolated according to the manufacturer's protocol (QIAamp DNA Mini Kit; QIAGEN, Gaithersburg, MD). DNA concentration was assessed using PicoGreen ds DNA detection (Life Technologies, Carlsbad, CA). All cases with at least 50 ng of DNA were subjected to NGS (HiSeq 2500; Illumina, San Diego, CA) performed on libraries prepared with custom-designed hybrid capture (Agilent SureSelect; Agilent Technologies, Santa Clara, CA) with baits of ∼5000 exons from 275 genes plus selected introns of 30 genes, as previously described (19 –21). Cases with known activating RAS mutations were identified, and the type of RAS mutation was recorded.
For each case with a RAS mutation, the cytology and surgical pathology reports and electronic medical records were reviewed, and clinicopathologic parameters and follow-up data were recorded. The FNA diagnoses were recorded from the pathology reports generated by staff cytopathologists using the Bethesda System for Reporting of Thyroid Cytopathology (22). For cases diagnosed histologically as FVPTC, tumor slides were re-reviewed by V.A.P. and J.A.B. to identify tumors that would now be classified as NIFTP. Tumors diagnosed as NIFTP had an entirely or nearly entirely follicular architecture (<1% papillae) and papillary-like nuclear features, including nuclear enlargement, elongation, contour irregularities, grooves, and clearing. NIFTPs included encapsulated tumors that had a complete fibrous capsule separating the tumor from the surrounding benign parenchyma and partially encapsulated/well-circumscribed tumors that had a partial capsule or entirely lacked a capsule yet had a sharp interface between the tumor and benign parenchyma. For all tumors, the entire tumor capsule/periphery had been submitted for histologic review at the time of the initial pathologic evaluation. Therefore, the entire tumor capsule/periphery could be histologically assessed in all cases in this study. Any tumor with nuclear features of PTC that had capsular penetration, lymphovascular invasion, or infiltrative growth was classified as invasive/infiltrative follicular variant of papillary thyroid carcinoma.
Fisher's exact test was used to evaluate the statistical significance of categorical variables, and an unpaired t-test was used to compare continuous variables. All p-values are two-sided, and a level of 0.05 was considered statistically significant. GraphPad Instat (GraphPad Software, San Diego, CA) was used to analyze the data.
Results
A total of 27 RAS-mutant thyroid tumors were identified, including 15 (56%) cases with an NRAS mutation, nine (33%) with an HRAS mutation, and three (11%) with a KRAS mutation. All RAS mutations were in codon 61, with the amino acid substitution Q61R accounting for the majority of constitutively activating mutations (n = 18; 67%) and the remainder had Q61K substitutions (n = 9; 33%). Although there were mutations detected in additional genes, the mutations were all characterized as variants of unknown significance. The nodules were from 8 men and 19 women, with a mean age of 51 years (range 29–69 years) at resection. The mean tumor size was 2.2 cm (range 0.7–5.4 cm). Ten (37%) patients underwent an initial lobectomy, 16 (59%) underwent an initial total thyroidectomy, and one (4%) underwent a completion thyroidectomy after a lobectomy 20 years prior. The surgical resection specimen demonstrated FVPTC in 20 (74%) cases, classical type PTC in two (7%), solid variant of PTC in one (4%), and follicular thyroid carcinoma in 4 (15%). Of the 20 FVPTCs, re-review of the slides showed that 16 (80%) would now be classified as NIFTP. NIFTPs accounted for 59% of RAS-mutant carcinomas overall. For the NIFTPs, there were 8 (50%) NRAS mutations, 7 (44%) HRAS mutations, and 1 (6%) KRAS mutation. There were no statistical differences in sex, patient age, tumor size, or extent of surgery between NIFTPs and FVPTCs with invasive or infiltrative growth. There were no lymph node metastases and no recurrences associated with either the NIFTPs or the infiltrative/invasive FVPTCs. The two classical PTCs with RAS mutations were predominantly follicular-patterned, with focal papillae comprising a small percentage of the tumor. Examples of NIFTPs with different RAS mutations and a classical type PTC with a RAS mutation are shown in Figure 1. The type of RAS mutations and final histologic diagnoses are summarized in Table 1.
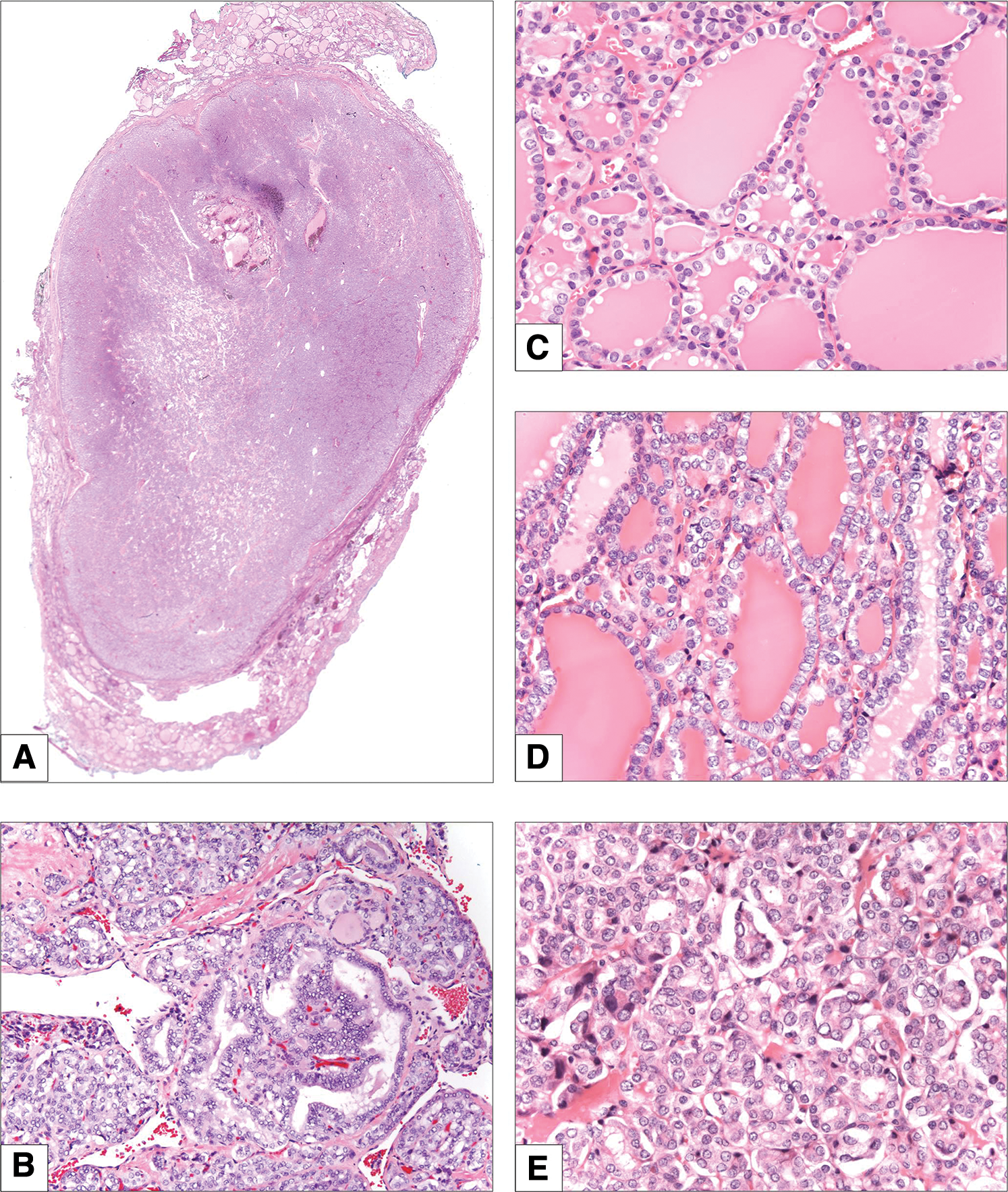
Examples of tumors with RAS mutations. (
AUS/FLUS, atypia/follicular lesion of undetermined significance; CPTC, classical type papillary thyroid carcinoma; FNA, fine-needle aspiration; FTC, follicular thyroid carcinoma; IFVPTC, invasive/infiltrative follicular variant of papillary thyroid carcinoma; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; SFN, suspicious for follicular neoplasm; SPTC, solid variant of papillary thyroid carcinoma; SUS, suspicious for malignancy.
Twenty-four (89%) cases had a preceding FNA. There were five (21%) cases with a previous malignant diagnosis on FNA, six (22%) cases with a diagnosis of SUS, five (19%) cases with a diagnosis of SFN, and eight (33%) cases with a diagnosis of AUS/FLUS. Overall, 19 (79%) of the cases with a prior FNA had an indeterminate FNA diagnosis. NIFTPs were preceded by a diagnosis of malignant in three (19%) cases, SUS in five (31%) cases, SFN in three (19%) cases, and AUS/FLUS in four (25%) cases. One (6%) NIFTP did not have a preceding FNA diagnosis. NIFTPs accounted for 63% of RAS-mutant carcinomas with a prior indeterminate FNA diagnosis in this cohort.
Discussion
Currently, molecular testing of nodules with an indeterminate FNA diagnosis has mainly been used to inform decisions regarding the need for surgical resection. In this rapidly evolving field, however, it appears that the type of molecular alteration may soon be used to guide extent of initial surgery. In fact, in a recent publication by the ATA on the application of molecular profiling of thyroid nodules on perioperative decision making, the authors indicate that as knowledge develops about genotype–phenotype correlations, gene-specific surgical recommendations may ensue (3). The aim of the current study was to evaluate the proportion of RAS-mutant tumors previously diagnosed as carcinoma that now would be classified as NIFTPs.
It was found that NIFTPs accounted for 59% of RAS-mutant “carcinomas” overall and 63% of RAS-mutant tumors with a prior indeterminate FNA diagnosis. The finding that NIFTPs comprised more than half of the tumors in this cohort is compatible with prior literature. Although molecular analysis was only performed on tumors with a histologic diagnosis of carcinoma, it is worth noting that not all RAS-mutant tumors are carcinomas (5,23 –26). The malignancy rate for RAS-mutant tumors varies widely between studies from 12% to 100% (5,6,23,24,26,27). This is likely due, in part, to differences in cohort characteristics, but it is also a result of differences in histologic evaluation of the tumors, that is, differences in assessment of nuclear features of PTC (in the case of FVPTC) and presence of capsular penetration (in the setting of follicular adenoma/follicular thyroid carcinoma). A study by Nikiforov et al. found that 85% of RAS-mutant tumors were carcinomas, with FVPTCs accounting for 85%, and follicular thyroid carcinoma and other PTC subtypes accounting for the remainder of the carcinomas (26). In a study by Medici et al., all RAS-mutant carcinomas in their cohort were FVPTCs without lymphovascular invasion, extrathyroidal extension, or lymph node metastases (25). Although the tumors in these cohorts were not characterized as NIFTPs due to the fact that these publications preceded the proposed NIFTP terminology, it is likely that many of the reported FVPTCs would now be classified as NIFTPs. Although most RAS-mutant tumors are low risk, it is important to note that not all are. In fact, approximately half of poorly differentiated thyroid carcinomas and roughly a quarter of anaplastic thyroid carcinomas harbor RAS mutations (28). Many of these aggressive tumors acquire additional mutations such as TERT promoter mutations, TP53 mutations, or molecular alterations in the PIK3CA-PTEN-AKT-mTOR pathway, SWI-SNF complex, histomethyltransferases, and mismatch repair genes (28). Therefore, a total thyroidectomy would likely be the appropriate initial surgery for a nodule found to have a RAS mutation along with a TP53 mutation, for example.
The downgrading of a subset of PTCs to NIFTP is expected to decrease the reported positive predictive value of current molecular tests for thyroid nodules. Nikiforov has estimated that it will result in a decrease in the positive predictive value of ThyroSeq v2 from 83% to 52% in FNA samples with a SFN diagnosis (29). This decrease is likely largely due to the decrease in percentage of RAS-mutant tumors diagnosed as carcinoma on resection. Along the same line, our group has recently shown that many of the tumors classified as suspicious by Afirma are NIFTPs (30). However, binary endpoints in the context of NIFTP have limitations because resection is the appropriate management for these tumors. Thus, it is appropriate that NIFTPs be resected regardless of terminology. Moreover, the finding that many of the carcinomas detected by tests such as ThyroSeq and the Afirma GEC are NIFTPs reflects the fact that these tests are being performed on nodules with a preceding indeterminate FNA result, which, compared with nodules with a preceding malignant FNA diagnosis, have been shown to demonstrate less aggressive histopathologic characteristics (31,32). In other words, carcinomas resected in the setting of an indeterminate FNA diagnosis have been shown most often to be FVPTCs without associated extrathyroidal extension or lymph node metastases (31,32). In fact, the emergence of NIFTP could make molecular testing of thyroid nodules with indeterminate FNA results even more important. Although it has been shown that cytologists can often accurately differentiate potential NIFTPs from classical PTCs (33), molecular testing could be used as an adjunct test to confirm the cytologist's impression. Finally, we have shown that many RAS-mutant “carcinomas” would now be classified as NIFTPs. However, potentially the same result would be found for other genetic alterations such as the BRAFK601E mutation and PPARG fusions that are also associated with NIFTP (14,34).
In conclusion, we report that more than half of “carcinomas” with a RAS mutation would currently be classified as NIFTPs. While all care should be individualized and include clinical and sonographic assessment, these results suggest that lobectomy as opposed to total thyroidectomy should be considered for nodules with a preceding indeterminate FNA result and a RAS mutation detected by molecular testing.
Footnotes
Author Disclosure Statement
E.A. is a consultant for Veracyte. No competing financial interests exist for the remaining authors.