
Abstract
Background:
Severe iodine deficiency during pregnancy results in neurodevelopmental disorders in children, while the consequences of mild to moderate iodine deficiency (MMID) are uncertain. The concentration of iodine in the thyroid is the most accurate indicator of iodine nutrition. This study aimed to evaluate whether the iodine stores in the thyroid cover the needs of the mother and the fetus in iodine-sufficient and MMID conditions by inductively coupled plasma-mass spectrometry.
Methods:
One hundred four-week-old female Wistar rats were randomly divided into MMID (low iodine intake [L]) and normal (normal iodine intake [N]) groups. The rats were fed for the next three months, and after pregnancy they were further divided into two subgroups, respectively: low iodine pregnancy (LP) and low iodine pregnancy with iodine supplement (LP+), and normal iodine intake pregnancy (NP) and normal iodine intake pregnancy with iodine supplement (NP+). The iodine intake of pregnant rats in the NP+ and LP+ groups was twice as much as in the NP and LP groups. The rats were sacrificed on gestational day 15 and postnatal day 7. The iodine concentration in the thyroid of the maternal and newborn rats, maternal serum, placenta, and amniotic fluid were determined by inductively coupled plasma-mass spectrometry.
Results:
The concentration of iodine in the thyroid of the N group was significantly higher than that in the L group before pregnancy. The concentration of iodine in the maternal thyroids of the LP group decreased during pregnancy, whereas that of the NP group did not change significantly. There was no significant difference in the iodine concentration in the thyroid of mothers and offspring between the NP and NP+ groups, but it was significant between LP and LP+ groups. The concentration of iodine in amniotic fluid was significantly different between the four groups.
Conclusion:
There is sufficient iodine storage in the thyroid of maternal rats with normal iodine intake during pregnancy, and there is no need for iodine supplementation. However, iodine stores are insufficient in rats with MMID. Iodine supplementation can increase the iodine concentration in the thyroid of maternal rats with MMID and their offspring, as well as in the amniotic fluid during pregnancy.
Introduction
I
It is generally believed that iodine intake should be increased during pregnancy, even in iodine-sufficient areas. However, there is a lack of clear evidence supporting this claim. The iodine concentration in the thyroid is the most accurate indicator of iodine nutrition. This study aimed at measuring the iodine store and metabolism in pregnant rats with a normal iodine intake and MMID in order to assess the necessity of iodine supplementation during pregnancy.
Animals and Methods
Animals
One hundred four-week-old specific pathogen-free (SPF) female Wistar rats (90–110 g) were purchased from Vital River Laboratories (Beijing, China). Rats were raised in standard cages in SPF conditions at 24 ± 2°C, with relative humidity of 45–55% under a 12 h/12 h light–dark cycle. All the animals and experimental procedures were approved by the Animal Research Committee of China Medical University, China. The experiments and procedures were carried out in accordance with the Guide for the Care and Use of Laboratory Animals, National Institutes of Health.
Feeding and grouping
After one week of adaptive feeding, the 100 rats were randomly divided into two groups: the MMID (low iodine intake [L]) group and the normal (normal iodine intake [N]) group. The rats were all fed a low-iodine diet and drinking water containing different concentrations of potassium iodide for the next three months. Water consumption and diet were recorded and calculated during the experiment. The low-iodine diet was obtained from iodine-deficient foods and was supplemented with inorganic salts and trace elements based on the standard American Institute of Nutrition (AIN)-93G diet (3). With the exception of iodine, the food was nutritionally complete. The iodine content of the diet was 30–40 μg/kg. Potassium iodide dissolved in deionized water was administered to both groups: 50 μg/L in the L group, and 130 μg/L in the N group. Twenty grams of food and 30 mL of water per day per rat were taken into consideration. The predicted iodine intake in the L and N groups were 2 μg/day and 4.5 μg/day, respectively.
After three months, 10 rats from the L and N groups were anesthetized and sacrificed. The remaining 40 rats from each group were randomly divided into two subgroups: low iodine pregnancy (LP) and low iodine pregnancy with iodine supplement (LP+), and normal iodine intake pregnancy (NP) and normal iodine intake pregnancy with iodine supplement (NP+), respectively (n = 20 in each group; Fig. 1). The female rats were mated with normal male Wistar rats (250–300 g, purchased from Vital River Laboratories), and the following day, a vaginal smear was obtained and analyzed under the microscope to confirm the presence of spermatozoa. Rats that were positive for spermatozoa were considered as mated, and the time was recorded as gestational day (GD) 0. From GD0, the LP+ and NP+ groups were administered drinking water containing 130 μg/L and 300 μg/L potassium iodide, respectively. The predicted iodine intake in the LP+ and NP+ groups was 4.5 μg/day and 9 μg/day, respectively. The LP and NP groups were administered the same drinking water as before until the end of the study. The day of birth was designated as postnatal day (PND) 0. Ten maternal rats from the NP and NP+ and LP and LP+ groups were sacrificed on GD15 and PND7, respectively, and 10 offspring rats from the NP and NP and LP and LP+ groups were sacrificed on PND7. All the rats were anesthetized with pentobarbital (40 mg/kg, intraperitoneally), bled, and perfused with buffered saline. Plasma was centrifuged and kept frozen at −20°C. After perfusion, the thyroid and placenta were dissected and stored at −80°C.
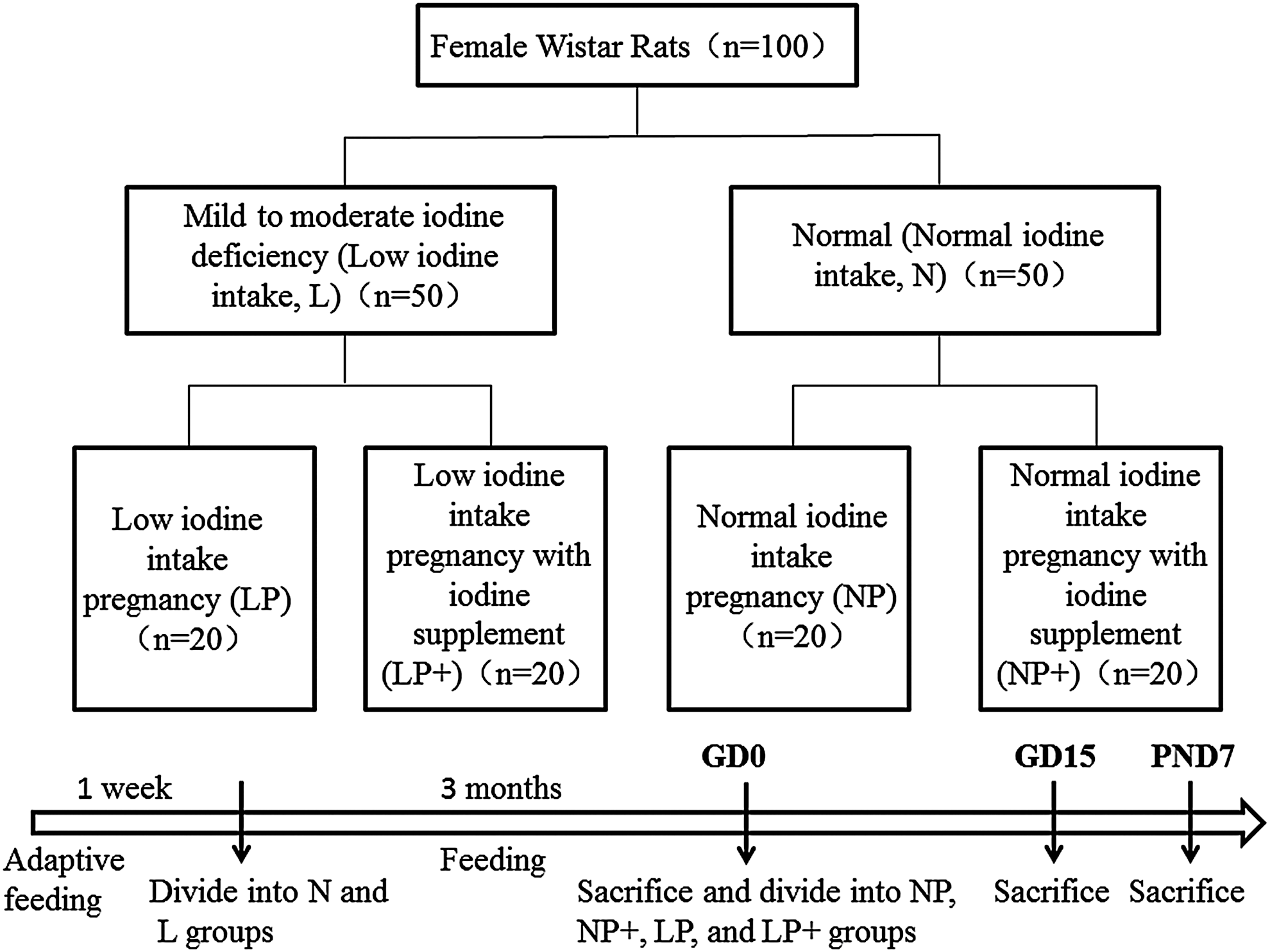
Groups and procedures. Rats that were positive for spermatozoa were considered as mated and the time was recorded as gestational day (GD) 0. The day of birth was designated as postnatal day (PND) 0.
Collection of urine
Urine was collected in a metabolic cage before and after pregnancy. The rats were placed in metabolic cages in the morning, and water consumption and diet were calculated. At the same time on the next morning, urine was collected, and urinary volume was noted. The urine was stored at −20°C for further measurement.
Measurement of iodine in tissue and urine
The Sandell–Kolthoff spectrophotometric method is the most commonly used method for iodine analysis. However, it is not included in the standard methods of the Association of Official Analytical Chemists. Several studies have postulated that not only iodine can catalyze the Sandell–Kolthoff reaction, but sodium and iron can accelerate this reaction, raising the possibility of a positive bias of the catalytic spectrophotometric methods compared with inductively coupled plasma-mass spectrometry (ICP-MS) (4 –7).
For ICP-MS, the sample was kept in a quartz tube, and 1 mL of nitric acid and 0.5 mL of hydrogen peroxide were added. The closed quartz tubes were placed inside a high-performance microwave digestion system (ETHOS 1; Milestone, Sorisole, Italy), and the sample decomposition was carried out according to a preselected program (35 min digestion time; 900 W of power). After cooling, 5 mL of ultrapure water and 2 mL of ammonia were added to the tubes. Finally, the digests were made up to 10 mL with ultrapure water. Terbium was added to the tubes for internal standardizing. Blanks were treated in the same manner. Two subsamples for each of the samples were digested. Nitric acid, hydrogen peroxide, and ammonia were purchased from Sinopharm Chemical Reagent Co. Ltd. (Beijing, China). Ultrapure water with a resistivity >18 MΩ was obtained from a Millipore MQ ion-exchange system fed with deionized water (US filter). Samples were analyzed using ICP-MS (7700; Agilent Technologies, Santa Clara, CA).
Determination of thyroid hormone
Serum thyrotropin (TSH), total triiodothyronine (TT3), total thyroxine (TT4), free T3 (fT3), and free T4 (fT4) levels were measured using an automated Immulite2000 analyzer with a chemiluminescent immunoassay kit (Diagnostic Products, Los Angeles, CA).
Determination of serum thyroglobulin
Serum samples were analyzed by enzyme-linked immunosorbent assay (USCN Life Science, Wuhan, China).
Statistical analysis
Statistical data are expressed as mean ± standard deviation, and were analyzed using SPSS Statistics for Windows v17.0 (SPSS, Inc., Chicago, IL). Differences between two groups were analyzed using Student's t-test, and differences among more than two groups were analyzed using one-way analysis of variance, followed by the least significant difference method. A p-value of <0.05 was considered statistically significant. All artwork was created using GraphPad Prism (GraphPad Software, Inc., La Jolla, CA).
Results
Urinary iodine in pregnant rats
Total 24 h urinary iodine is illustrated in Figure 2. The urinary iodine concentrations of the pre-pregnancy rats were 4.13 ± 0.31 and 1.73 ± 0.11 μg/24 h. In both the NP and the LP groups, the urinary iodine concentrations increased significantly in the first trimester (T1) (p < 0.05) and decreased in the second (T2) and third trimesters (T3).
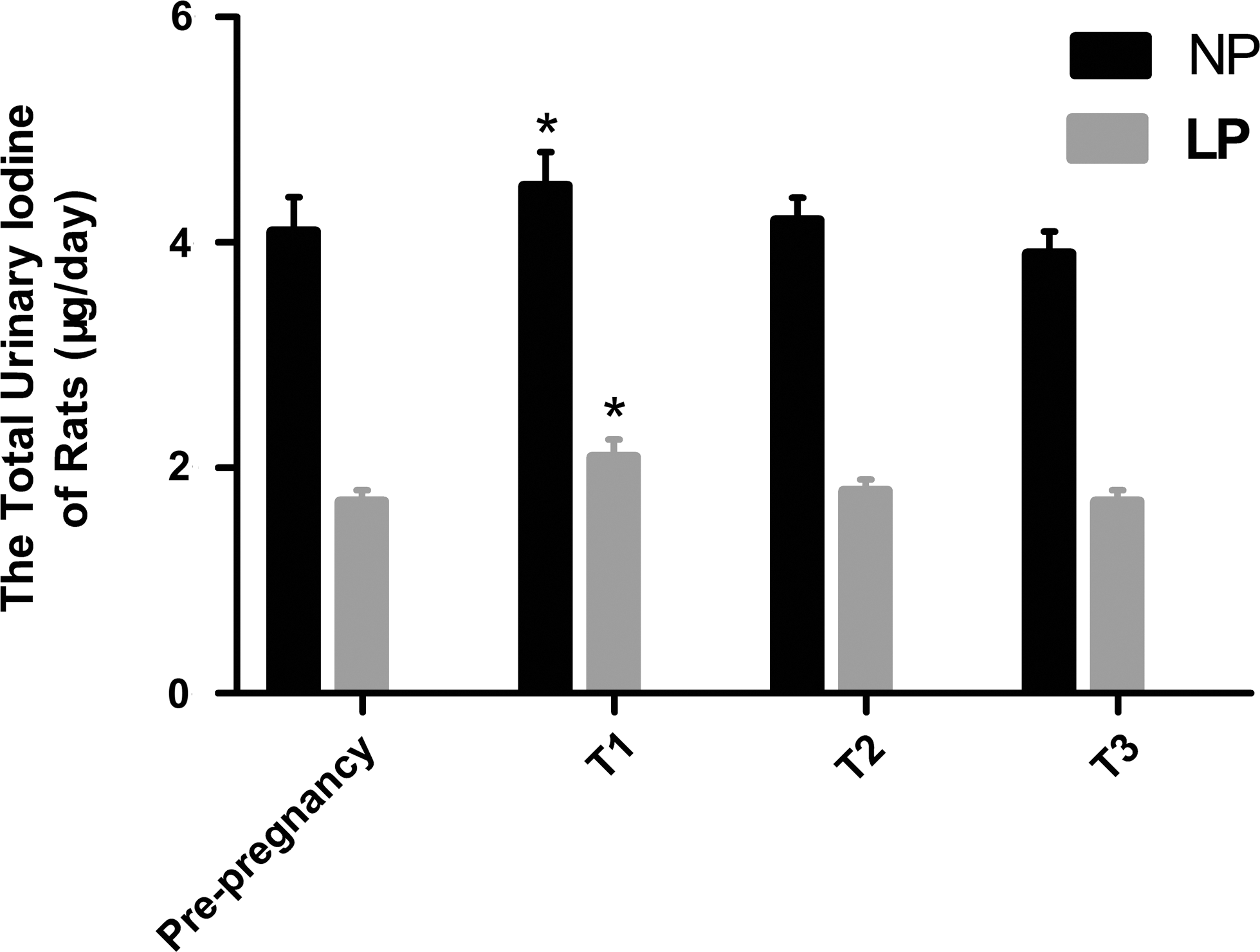
Total urinary iodine concentration of rats in each group. *p < 0.05 compared with other groups. T1, first trimester; T2, second trimester; T3, third trimester.
Concentration of iodine in the maternal thyroid
The concentration of iodine in the maternal thyroid was 112.7 ± 13.7 and 82.6 ± 10.6 μg/g in the N and L groups, respectively, and there was a significant change between the groups (p < 0.05). On GD15, the concentration of iodine in the NP group increased to 117.5 ± 19.6 μg/g, and dropped to 104.3 ± 15.4 μg/g on PND7. The concentration of iodine in the NP+ group was 110.0 ± 11.9 and 96.7 ± 12.3 μg/g on GD15 and PND7, respectively. The concentration of iodine in the thyroid of the LP group significantly decreased to 65.7 ± 9.2 μg/g on GD15, and further decreased to 47.0 ± 8.2 μg/g on PND7 (p < 0.05). The concentration of iodine in the LP+ group was 75.4 ± 10.7 and 65.1 ± 11.2 μg/g on GD15 and PND7, respectively, which was significantly higher than in the LP group (p < 0.05; Fig. 3A).
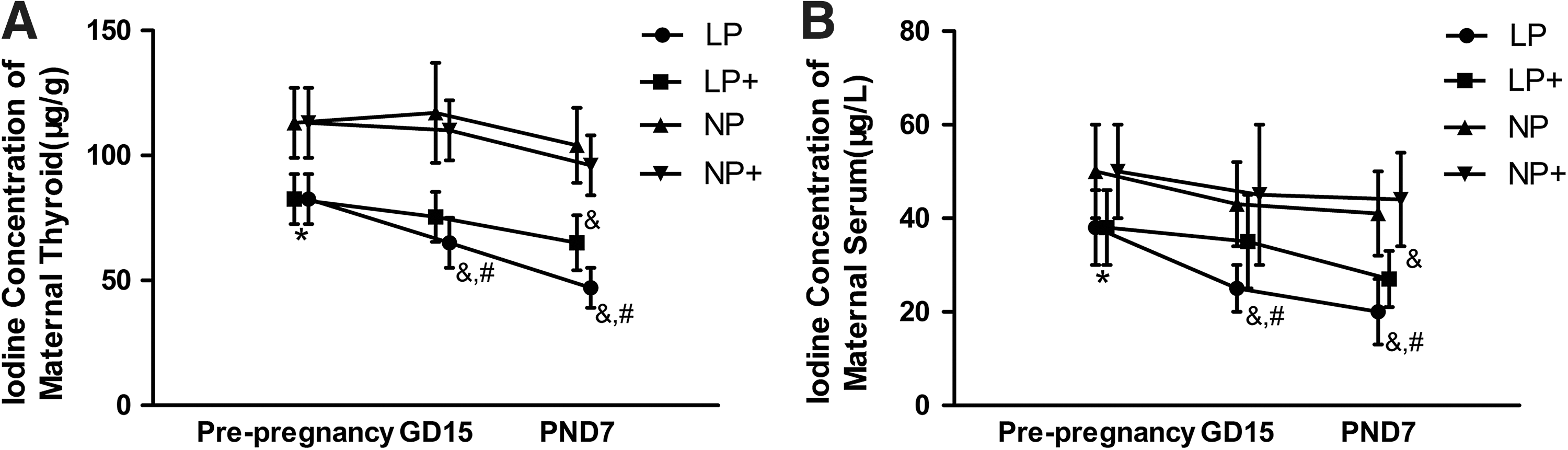
Iodine concentration in the maternal thyroid and serum in each group. (
Concentration of iodine in the placenta
The concentration of iodine in the placenta of the NP and NP+ groups was 84.8 ± 16.8 and 72.8 ± 20.4 ng/g, respectively, but the difference was not significant. The concentration of iodine in the placenta of the LP and LP+ groups was 47.1 ± 12.8 and 51.6 ± 14.8 ng/g, respectively, and that in the normal group was significantly higher than that in the iodine-deficient group (p < 0.05; Fig. 4A).
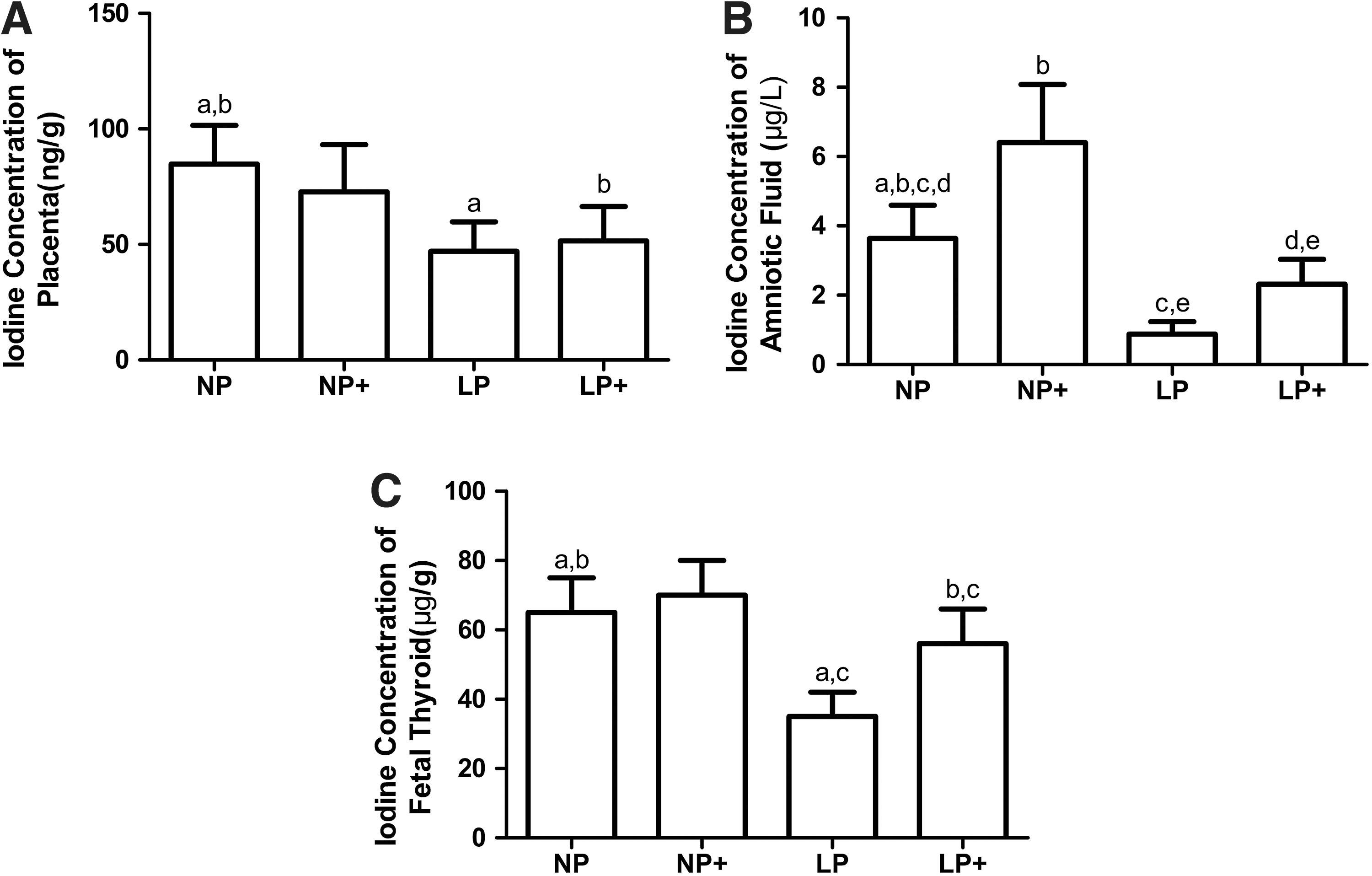
Iodine concentration in the placenta, amniotic fluid, and the thyroid of offspring in each group. (
Concentration of iodine in amniotic fluid
The concentration of iodine in the amniotic fluid was tested on GD15, and it correlated with maternal iodine nutrition. It was 3.6 ± 0.9, 6.4 ± 1.7, 0.9 ± 0.3, and 2.3 ± 0.7 μg/L in the NP, NP+, LP, and LP+ groups, respectively. There were significant changes among the four groups (p < 0.05; Fig. 4B).
Concentration of iodine in the thyroid of offspring
The iodine concentration in the thyroid of the offspring in the NP and NP+ groups was 65.5 ± 15.4 and 70.3 ± 13.8 μg/g, respectively, but the difference was not significant. However, the concentration of iodine in the LP and LP+ groups was 35.7 ± 6.9 and 56.0 ± 10.4 μg/g, respectively, and there was a significant difference (p < 0.05; Fig. 4C).
Concentration of iodine in maternal serum
The concentration of iodine in maternal serum was 51.1 ± 10.4 and 38.7 ± 8.4 μg/L in the N and L groups, respectively, and there was a significant change between the two groups (p < 0.05). It was 43.6 ± 8.7 μg/L on GD15 and 41.6 ± 9.5 μg/L on PND7 in the NP group. The concentration of iodine in maternal serum was 45.2 ± 15.4 μg/L and 44.5 ± 9.4 μg/L in the NP+ group on GD15 and PND7. On GD15, the concentration of iodine in the LP group decreased to 25.7 ± 5.4 μg/g, and on PND7 it decreased to 20.5 ± 7.2 μg/g, which was significantly lower than before pregnancy (p < 0.05). The concentration of serum iodine in the LP+ group also decreased to 35.7 ± 9.6 μg/L on GD15 and to 27.5 ± 6.2 μg/L on PND7, which was significantly higher than in the LP group (p < 0.05; Fig. 3B).
Maternal serum thyroglobulin concentration
The serum thyroglobulin (Tg) concentration in the N group was significantly lower than that in the L group (p < 0.05). There was a small change in the serum Tg concentration in the NP and NP+ groups during pregnancy. In the LP group, serum Tg on PND7 was higher than in the nonpregnant group. In addition, in the LP+ group, serum Tg was lower than in the LP group on GD15 and PND7, but there was no significant difference (Fig. 5).
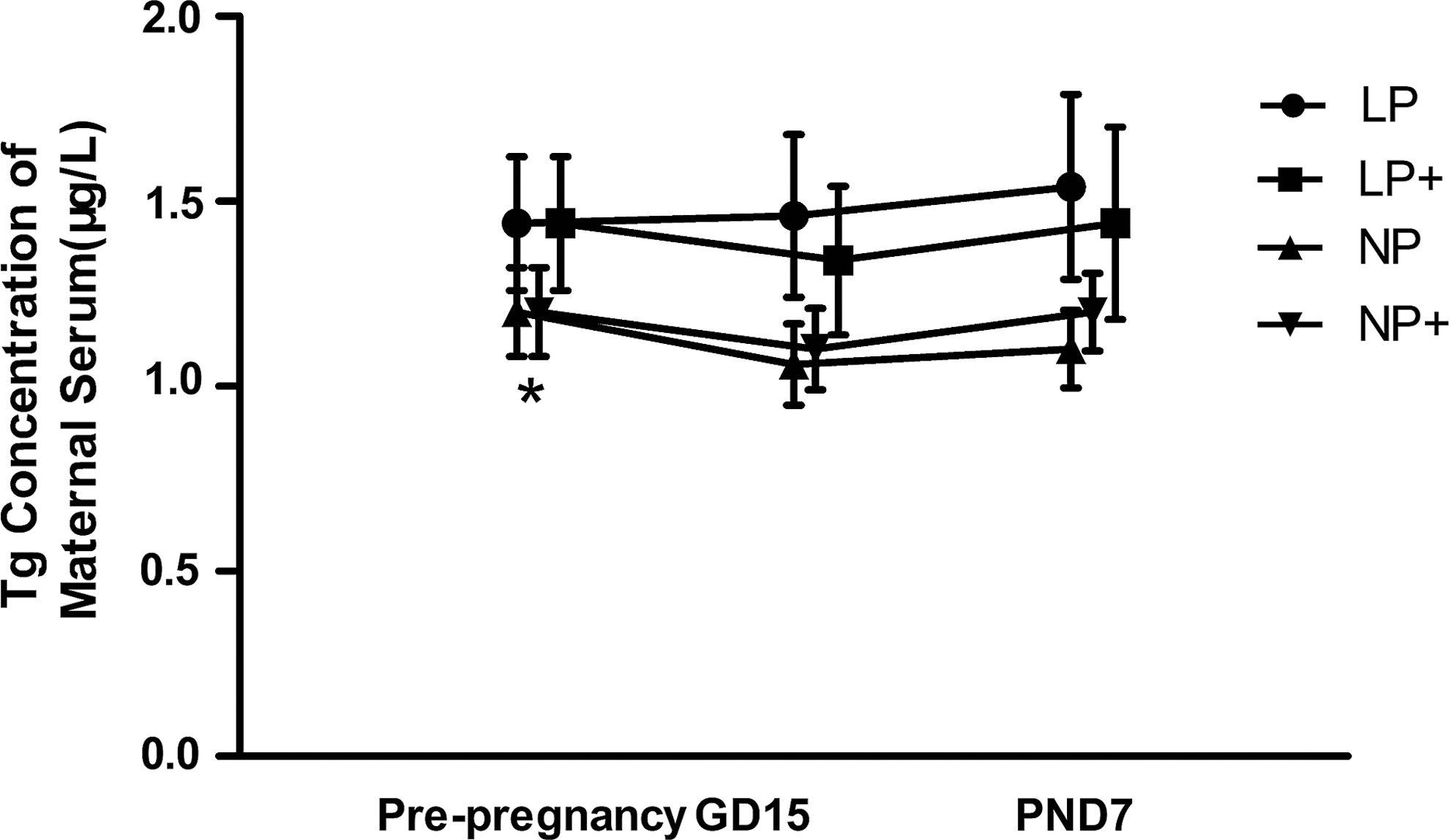
Thyroglobulin concentration in the maternal serum in each group, *p < 0.05 compared with the L group.
Maternal serum thyroid hormone concentration
There was no significant change in serum TT3, TT4, fT3, fT4, and TSH in the N, NP, and NP+ groups. In the MMID groups, compared with the LP group, the TT4 level significantly increased in the LP+ group on GD15, whereas the TT3/TT4 ratios decreased (p < 0.05). There was a significant change in serum TSH, TT4, fT4, and TT3/TT4 in the normal and MMID groups (p < 0.05; Table 1).
Results are mean ± standard deviation.
p < 0.05 compared with normal group; * p < 0.05 compared with LP group.
TSH, thyrotropin; fT3, free triiodothyronine; TT3, total T3; fT4, free thyroxine; TT4, total T4; N, normal group; NP, normal iodine intake in pregnancy group; NP+, normal iodine intake in pregnancy with iodine supplement; L, low iodine intake group; LP, low iodine in pregnancy group; LP+, low iodine in pregnancy with iodine supplement group; GD, gestational day; PN, postnatal day.
Discussion
According to the AIN-93G standard of animal diets, the iodine intake of rats is ∼4 μg. Other related research also showed that the daily iodine intake for rats is 4–5 μg (8). A previous study our group confirmed that the iodine intake for rats with marginal iodine deficiency was 3 μg/day and 1.2 μg/day for severe deficiency (9). This is similar to another study showing an intake of 3 μg/day for mild iodine deficiency and 1.5 μg/day for severe deficiency (10). In this study, 2 μg/day and 4.5 μg/day were chosen for MMID and normal iodine intake, respectively. The findings show that the urinary iodine in MMID rats was ∼50% of that in the normal group, with elevated serum TSH, TT3/TT4, and Tg, and decreased serum fT4, and TT4. All these changes indicate that the rats were in a state of iodine deficiency. Pregnancy rate and the mortality of maternal and newborn rats were similar in normal and MMID rats. Moreover, there was no significant change in body and thyroid weight between the normal and MMID groups. These results differ from findings associated with severe iodine deficiency.
The iodine concentration in the thyroid is a better indicator for the evaluation of iodine nutrition than urinary iodine is. In rats evaluated after pregnancy, the concentration of iodine in the maternal thyroid on PND7 decreased by >50% compared with the pre-pregnancy levels. In contrast, the concentration of iodine in the thyroid of normal rats did not change significantly, which indicates that there was no obvious iodine deficiency during pregnancy. It was also found that the thyroidal iodine concentration in newborn offspring in the LP group was only half of that observed in the NP group, which indicates that the iodine stores in the thyroid of offspring were affected by the iodine-restricted MMID condition.
The World Health Organization (WHO), the United States Institute of Medicine, and the American Thyroid Association all recommend increasing iodine intake during pregnancy, even in iodine-sufficient regions (11 –13). The present study found that the concentration of iodine in the maternal thyroid on GD15 and newborn offspring did not change significantly with or without iodine supplementation during normal pregnancy. In contrast, there were significant differences between the LP and LP+ groups in the MMID group. Based on this, one can infer that for MMID rats, iodine treatment is beneficial for the mother and the offspring.
In the growth and development of offspring, the role of the placenta and amniotic fluid is important. It has been confirmed that the placenta is an organ rich in iodine (14,15). The data presented here demonstrate that the iodine concentration in the placenta was related to the pre-gestational iodine nutrition status, and the concentration in the LP group was significantly lower than that in the NP group. In addition, iodine treatment during pregnancy did not significantly affect iodine concentration in the placenta. This suggests that iodine transportation in the placenta is likely an active process and not merely a passive one. Amniotic fluid is rich in nutrients that are needed for fetal growth, and it provides mechanical cushioning. The source of amniotic fluid changes with the different stages of fetal development. Amniotic fluid is derived from blood plasma components during early pregnancy and mainly from fetal urine in late pregnancy (16). Thus, in late pregnancy, the concentration of iodine in amniotic fluid directly reflects the level of iodine nutrition in the offspring (17). Early in the last century, it was found that iodine-containing drugs can significantly increase urinary iodine in pregnant women and iodine concentrations in the amniotic fluid (18). It has also been confirmed that fetal TSH levels correlate with the iodine content of the amniotic fluid (19). In this study, there were significant differences in the iodine concentration in the amniotic fluid between the four groups, indicating that the iodine concentration in amniotic fluid is affected by iodine treatment during pregnancy, as well as the pre-gestational maternal iodine status.
Serum Tg is another important indicator of iodine nutrition (20), and it is widely used in children (21). However, the use of Tg as a biomarker for the iodine status of pregnant women is still controversial, and is confronted with many unresolved questions. In this study, serum Tg concentrations in normal rats were significantly lower than in the MMID group. The serum Tg concentration in the LP group on PND7 was higher, although the change was not significant. This result is consistent with previous epidemiological studies (22,23). However, it is worth noting that on GD15 and PND7, serum Tg in the NP+ group was higher than in the NP group, although not significantly. Serum Tg levels in pregnancy are influenced by physiological changes, including the iodine status, human chorionic gonadotropin, and TSH (24). Therefore, further research on the regulation of Tg during pregnancy is needed.
Compared with the LP group, TT4 levels in the LP+ group significantly increased on GD15, whereas the TT3/TT4 ratio was decreased. This indicates that iodine supplementation was beneficial for MMID pregnant rats. On the contrary, no significant change was observed in TSH, TT3, TT4, fT3, and fT4 levels in the NP and NP+ groups. In addition, the risk of increased TSH levels in the NP+ group was higher than that in the NP group on PND7. This suggests that iodine supplementation was not beneficial for iodine-sufficient rats during pregnancy and lactation, and it might even be harmful. Rebagliato et al. found in an iodine-sufficient region that there was an increased risk of TSH levels >3 mIU/L in women who consumed >200 μg/day of iodine supplements compared with those who consumed <100 μg/day. Additionally, pregnant women with high urinary iodine concentrations were prone to hypothyroxinemia (25). Later, Murcia et al. found that maternal intake of 150 μg/day compared with <100 μg/day of iodine from supplements was associated with a 5.2-point decrease in the Psychomotor Development Index. Thus, further evidence on the safety and effectiveness of iodine supplementation during pregnancy is needed before it is systematically recommended in iodine-sufficient or mildly deficient areas (26).
In conclusion, there are sufficient iodine stores in the thyroid of maternal rats with normal iodine intake during pregnancy, and there is no need for iodine supplementation. However, it is insufficient in rats with MMID. Iodine supplementation can increase the iodine concentration in the thyroid of maternal rats with MMID and their offspring, as well as in amniotic fluid during pregnancy.
Footnotes
Acknowledgments
The language of the manuscript has been refined and polished by the International Science Editing Company.
Author Disclosure Statement
The authors have nothing to disclose.