
Abstract

In a recent issue of Thyroid, Barbesino reported on the interference of biotin intake in thyrotropin (TSH), free thyroxine (fT4), and triiodothyronine (T3) measurements, leading to a misdiagnosis of Graves' disease (1). Other recent case reports have confirmed this finding (2,3).
Biotin has a high affinity for streptavidin, and this phenomenon has been used in the design of competitive (fT4, T3) and immunometric assays (TSH). In both types of assays, an excess of biotin can result in low signal production, although the result depends on the assay design: falsely high levels are observed in competitive immunoassays, such as fT4 and T3, and falsely low levels are observed in immunometric “sandwich” assays, such as those used for TSH measurements (4,5).
To investigate how biotin directly interferes with these assays, samples were collected for TSH, fT4, and T3 measurements from 19 adult volunteers before and after oral ingestion of biotin (10 mg). The dose used was approximately 100 times higher than the required daily dose (30–100 μg) but corresponds to the dose in commercial dietary supplements. Blood samples were collected before and at 3 and 24 h after biotin ingestion. All the subjects collected the basal samples and the 24 h samples between 7:00 and 8:00am at fasting, and 3 h samples between 10:00 and 11:00am. None of the volunteers was taking any type of medication or had a personal or family history of thyroid disease. TSH and T3 measurement were performed with an electrochemiluminescence immunoassay (Roche Diagnostics GmbH, Mannheim, Germany; reference range 0.45–4.5 mIU/L for TSH and 70–200 ng/dL for T3). The fT4 measurement was performed with a chemiluminescent immunoassay (Access; Beckman Coulter, Brea, CA; reference range 0.6–1.3 ng/dL). TSH and T3 assays used streptavidin-coated microparticles as the strategy for streptavidin-biotin interaction, and the fT4 assay used streptavidin-coated solid phase. After obtaining Fleury Ethics Committee approval (protocol number 1546784), signed informed consent was obtained from all patients.
The mean level of TSH was 2.84 ± 1.27 mIU/L before biotin intake, and this decreased to 1.66 ± 0.6 mIU/L at 3 h after biotin ingestion (p < 0.005). However, none of the subjects had a TSH below the lower reference range 3 h after biotin ingestion. One important aspect that should be considered is the failure in the diagnosis of subclinical hypothyroidism in the two subjects with slight elevation of basal TSH concentrations, which dropped, to normal values after biotin ingestion. Regarding fT4 measurements, the mean level of fT4 was 0.8 ± 0.1 ng/dL before biotin ingestion and increased to 1.2 ± 0.2 ng/dL at 3 h after biotin ingestion (p < 0.0001); 10/19 (52%) subjects showed concentrations above the upper reference limit. The mean level of T3 was 116 ± 10 ng/dL before biotin ingestion and increased to 154 ± 26 ng/dL at 3 h after biotin ingestion (p < 0.0001), but all the concentrations of all samples remained within the reference range.
At 24 h after biotin ingestion, TSH, fT4, and T3 levels returned to the appropriate reference intervals and did not differ significantly from the basal concentrations. Figure 1 summarizes the mean TSH, fT4, and T3 values before and at 3 and 24 h after biotin ingestion.
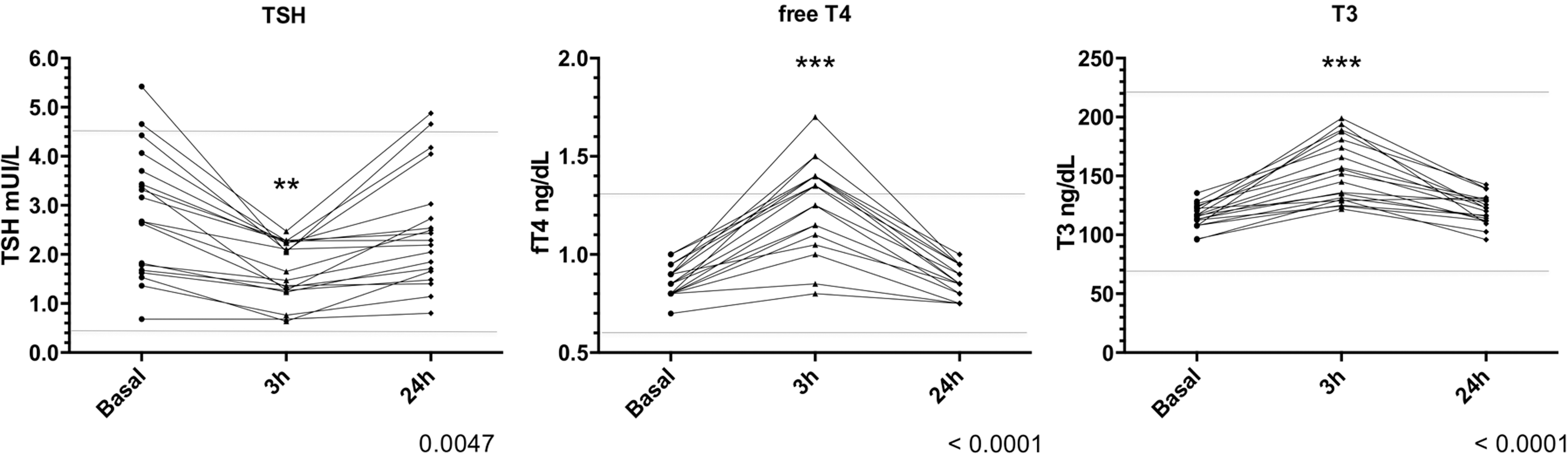
Left: Mean thyrotropin values before and at 3 and 24 h after biotin ingestion (reference range 0.45–4.5 mIU/L). Middle: Mean free thyroxine values before and at 3 and 24 h after biotin ingestion (reference range 0.6–1.3 ng/dL). Right: Mean triiodothyronine values before and at 3 and 24 h after biotin ingestion (reference range 70–200 ng/dL). **p < 0.05; ***p < 0.001.
In the past few months, several thyroid hormone profiles suggestive of Graves' disease have been identified in our laboratory in asymptomatic patients ingesting high doses of biotin. These interesting findings combined with a literature review of single case reports of patients with the same hormonal profile (1 –3) motivated us to perform this study. This is the first study to demonstrate that acute ingestion of biotin (10 mg) by healthy volunteers interferes with TSH, fT4, and T3 assays, and these effects disappear within 24 h. The biotin dose used corresponds to the one in over-the-counter diet supplements. Previously, Wijeratne et al. demonstrated a similar effect after ingestion of 30 mg of biotin in a single subject (5). Therefore, these findings are consistent with acute exogenous interference of biotin in these assays and exclude thyroid disease or alterations in thyroid hormone clearance. This possibility must be considered in patients taking biotin and presenting with laboratory findings suggestive for hyperthyroidism but without clinical symptoms of the disease. In these cases, biotin should be discontinued, and a new sample should be collected for repeat thyroid function tests. In principle, this type of interference should be considered in all immunoassays using a streptavidin-biotin design. In the present study, assays using both streptavidin–biotin interaction strategies (streptavidin-coated particles and streptavidin-coated solid phase) were associated with the same phenomenon.
Footnotes
Author Disclosure Statement
All authors are consultants for Fleury Group.