
Abstract
Background:
Racial disparities in the management of differentiated thyroid cancer (DTC) exist in the United States. There is a paucity of data examining their temporal trends. It was hypothesized that racial disparities in care provided to patients with DTC have improved over the past 15 years.
Methods:
Adult patients undergoing surgery for DTC were included from the National Cancer Data Base (1998–2012). Temporal trends in appropriate extent of thyroidectomy and radioactive iodine therapy (RAI) were described for different racial groups. Multivariable logistic regression models were employed to estimate the adjusted association of receipt of appropriate extent of surgery and RAI, specifically under- and over-treatment, among different racial groups.
Results:
Among 282,043 DTC patients, 80.3% were non-Hispanic white (white), 8.1% Hispanic, 7.2% non-Hispanic black (black), and 4.4% Asian. Black versus white race/ethnicity was associated with lower odds of receiving appropriate surgery (odds ratio [OR] = 0.78 [confidence interval (CI) 0.71–0.87]; p < 0.001). Appropriate RAI treatment was higher in blacks (OR = 1.07 [CI 1.02–1.12]; p = 0.01) and lower for Hispanics (OR = 0.90 [CI 0.86–0.95]; p < 0.001) compared with whites. There was a higher likelihood of RAI under-treatment in minority groups (Hispanic OR = 1.27, black OR = 1.26, Asian OR = 1.25; p < 0.001), and a lower likelihood of RAI over-treatment (Hispanic OR = 0.89, black OR = 0.83, Asian OR = 0.79; p < 0.001) compared with whites. Over time, an increasing proportion of black and white patients underwent appropriate extent of thyroidectomy (1998 vs. 2012: 78% vs. 88% and 81% vs. 91%, respectively). Compared with 1998, fewer patients in 2012 were under-treated with RAI: whites (48% vs. 29%, respectively), blacks (51% vs. 33%), Hispanics (51% vs. 37%), and Asians (55% vs. 39%). The extent of RAI over-treatment increased (1998 vs. 2012): whites (1% vs. 4%), blacks (2% vs. 4%), Hispanics (2% vs. 4%), and Asians (2% vs. 3%), respectively.
Conclusions:
Appropriate utilization of surgery and RAI for DTC has improved over time. However, the proportion of patients receiving appropriate thyroid surgery is consistently lower for blacks compared with whites. RAI over-treatment increased for all races over the study period. Efforts are needed to standardize DTC care among minority patients.
Introduction
R
Thyroid cancer is the fastest increasing malignancy in the United States, with an incidence that has increased by nearly 300% in the last three decades (10,11). While this increase seems to be leveling off (12), costs of treatment and follow-up care for thyroid cancer are substantial (13), making it an important public health issue (14). Differentiated thyroid cancer (DTC) accounts for >90% of the new cases of thyroid cancer diagnosed in the United States. Thyroidectomy with or without postoperative administration of radioactive iodine therapy (RAI) represents the mainstay of treatment for DTC. While prognosis from thyroid cancer is generally excellent, patient outcomes are significantly associated with receipt of evidence-informed therapy (15). Thyroid cancer patients receiving care that is out of step with national practice guidelines have been demonstrated to experience compromised survival (16).
There is a growing body of research demonstrating that racial disparities in thyroid cancer care persist in the United States (17 –23). These studies have demonstrated the association of race/ethnicity with clinicopathologic characteristics of disease at presentation: larger tumor size, more follicular pathology, higher complication rates, longer hospital stay, and lower compliance with treatment recommended in guidelines have been observed among minority populations and especially among blacks (17 –25). Multiple efforts have been initiated at the national level to address the issue of racial disparities in the management of thyroid cancer (8,17,26,27). The Endocrine Society in a scientific statement on healthcare disparities in endocrine disorders has stressed the need to “develop policies to increase minority access to high-volume surgeons and earlier intervention in centers with appropriate endocrine and surgical expertise so as to improve clinical outcomes and reduce mortality in minorities with thyroid cancer” (17). Highlights from the 2013 National Healthcare Quality and Disparities Reports stressed the need to “improve access to care, reduce disparities, and accelerate the pace of quality improvement, especially in the areas of preventive care and chronic disease management,” including cancer care (27).
The aim of this study was to evaluate how racial/ethnic differences have evolved in the United States over the last two decades with regard to the extent and appropriateness of surgery and RAI treatment for DTC.
Methods
Data source
The National Cancer Data Base (NCDB) is a joint program of the American Cancer Society and the Commission on Cancer (CoC) of the American College of Surgeons. The NCDB is a nationwide, facility-based, comprehensive data set containing more than 29 million cancer cases from 1500 CoC-accredited cancer programs across the United States, capturing at least 85% of all new thyroid cancer cases.
The NCDB Participant User File was used to identify all patients with thyroid cancer who underwent thyroid surgery with or without RAI treatment for whom data were available between 1998 and 2012. Adult patients with DTC (papillary and follicular) were identified by using the following International Classification of Diseases for Oncology, 3rd Edition (ICD-O-3) codes: 8050/3, 8260/3, 8340/3, 8341/3, 8342/3, 8343/3, 8344/3, 8290/3, 8330/3, 8331/3, 8332/3, and 8335/3. Patients diagnosed with Hürthle cell carcinoma were excluded due to the small sample size and lack of consistency in treatment guidelines (28,29). Variables such as patient age at diagnosis, race/ethnicity, sex, annual income, insurance status, and year of diagnosis were obtained from the database. Annual income was determined from the NCDB by linking each patient's ZIP code to the year 2000 United States Census data. Racial groups were defined as non-Hispanic white (white), non-Hispanic black (black), Hispanic, and Asian. Patients with unknown race information or race classified as “other” were excluded.
Data on extent of surgery (documented as thyroid nodulectomy, thyroid lobectomy, or total thyroidectomy), extrathyroidal extension, status of the surgical margins, and receipt of RAI treatment also were extracted from the database. Thyroid nodulectomy was defined as removal of less than a thyroid lobe. Thyroid lobectomy was defined as removal of a lobe, and total thyroidectomy included total, near-total, or subtotal thyroidectomy (30,31). Patients with known extent of thyroid surgery were categorized as having appropriate versus inappropriate thyroid surgery based on their risk category as defined by American Thyroid Association (ATA) and National Comprehensive Cancer Network (NCCN) guidelines (32 –35). Inclusion of both NCCN and ATA guidelines was important to define practice patterns over the course of the study. Hence, the criteria defining risk were broad, as defined below for both surgery and RAI treatment. The appropriateness of thyroid surgery was defined as a total thyroidectomy or lobectomy for low-risk tumors (intrathyroidal tumor size <4 cm with no lymph node or distant metastases) and a total thyroidectomy as appropriate treatment for intermediate/high risk tumors (tumor size >4 cm, or any size tumor with extrathyroidal extension or lymph node or distant metastases). Inappropriate thyroid surgery was defined as nodulectomy (any tumor size with or without lymph node or distant metastases) and lobectomy for intermediate/high-risk tumors (Table 1). Patients with known RAI data were categorized as having received appropriate RAI treatment, RAI under-treatment, or RAI over-treatment based on ATA/NCCN guidelines (32 –35). The appropriate RAI treatment group included those patients who were indicated to receive RAI and did, and those who were not indicated to receive RAI and did not. The under-treatment group included those who did not receive RAI treatment when it was indicated, and included patients with any of the following: tumors ≥4 cm, with extrathyroidal extension, positive surgical margins, and lymph node or distant metastases. The over-treatment group included those who received RAI treatment when it was not indicated, and patients with tumors < cm, no extrathyroidal extension, negative surgical margins, and no lymph node or distant metastases (Table 1).
LN, lymph node; RAI, radioactive iodine; +, present; −, absent.
Statistical analyses
The cohort was analyzed by patient race/ethnicity using four groups: white, Hispanic, black, and Asian. Patient characteristics were summarized by race/ethnicity with n (%) for categorical variables and median (interquartile range) for continuous variables. Chi-square tests were used to compare categorical variables, and analysis of variance was used for continuous variables.
Multivariable logistic modeling was employed to estimate the adjusted odds ratios (ORs) and confidence intervals (CIs) for race/ethnicity and year of diagnosis after adjustment for known covariates for each outcome (appropriate surgery, appropriate RAI treatment, RAI under-treatment, and RAI over-treatment). A similar stratified analysis was performed based on geographic region (West, South, Midwest, or Northeast). Each model was conducted with the addition of a year of diagnosis × race interaction term to determine if the change over time differed by race. Overall survival (OS) was defined as the time from diagnosis to death from any cause, or last follow-up. Survival was compared between groups using the log-rank test, and the 5- and 10-year OS rates were estimated using the Kaplan–Meier method. A two-sided significance level of 0.01 was used for all statistical tests. All statistical analyses were conducted using SAS v9.4 (SAS Institute, Cary, NC). This study was deemed to be exempt by the Institutional Review Board.
Results
A total of 282,043 patients with DTC were included in the analysis. Overall, 80.3% were white, 8.1% Hispanic, 7.2% black, and 4.4% Asian (Table 2). Black and Hispanic patients were less likely to have medical insurance (91.3% and 84.8%, respectively) compared with white and Asian patients (94.9% and 93.0%, respectively; p < 0.001). They also were more likely to be from areas with a median annual income <$35,000 (44.0% and 35.1%) compared with either white or Asian patients (21.6% and 13.8%, respectively; p < 0.001). Compared with other patients, black patients more often presented with larger tumors (>4 cm) and were less likely to undergo lymph node dissection. Consequently, black patients were found to have a lower rate of documented lymph node metastases.
Appropriate RAI includes patients with indications for RAI and who received it, and patients who did not have indications for RAI and did not receive it. Over-treatment includes patients who did not have indications for RAI but received it. Under-treatment includes patients who did have indications for RAI but did not receive it. Values are presented as percentages of given sample size. Percentages were rounded and may not add to 100 because of missing values. White and black are non-Hispanic.
Log-rank p-value.
DTC, differentiated thyroid cancer; NCDB, National Cancer Data Base; IQR, interquartile range; OS, overall survival.
Compared with white patients, black patients had reduced 5- and 10-year OS rates (94% vs. 93% and 87% vs. 84%, respectively; log-rank p < 0.001). Hispanic patients had the highest rate of 30-day readmission (5.2%), followed by black (4.4%), Asian (3.8%), and white patients (3.6%; p < 0.001). Thirty- and 90-day mortality rates were highest for black patients (0.2% and 0.4%, respectively), but similar for the other races (p < 0.001).
Overall, the majority of the patients underwent total thyroidectomy (80.4%), and extent of surgery (lobectomy vs. total thyroidectomy) was largely similar across race groups. Appropriate extent of thyroid surgery was less likely to be performed for black compared with white patients (90.7% vs. 93.1%; p < 0.001 in unadjusted analyses). After adjustment, black race was associated with lower odds of receiving appropriate extent of thyroid surgery compared with white race (OR = 0.78 [CI 0.71–0.87]; p < 0.001; Table 3).
The reference level for all odds ratios is non-Hispanic white. Surgery odds ratios are adjusted for year of diagnosis, patient age, clinical stage, hospital type, income level, insurance status, sex, and cancer type. RAI odds ratios are adjusted for year of diagnosis, patient age, clinical stage, hospital type, income level, insurance status, sex, cancer type, extent of surgery, tumor size, if patients had lymph nodes examined or positive, and margin status. All region odds ratios were also adjusted for hospital location.
AOR, adjusted odds ratio.
In total, 47.8% of patients received RAI. The odds of receipt of appropriate RAI treatment were higher for blacks (OR = 1.07 [CI 1.02–1.12]; p = 0.01) and lower for Hispanics (OR = 0.90 [CI 0.86–0.95]; p < 0.001) compared with white patients. The likelihood of RAI under-treatment was higher for all other races compared with white patients (Hispanic OR = 1.27 [CI 1.18–1.36]; black OR = 1.269[CI 1.17–1.37]; Asian OR = 1.25 [CI 1.14–1.37]; p < 0.001), while whites were more likely to be over-treated with RAI when compared with all other races (Hispanic OR = 0.89 [CI 0.84–0.94]; black OR = 0.83 [CI 0.79–0.88]; Asian OR = 0.79 [CI 0.74–0.85]; p < 0.001; Table 3).
Temporal trends in appropriate extent of thyroid surgery
After adjustment, there was an improvement over time in appropriate surgical care as measured by extent of thyroid surgery. However, black patients consistently had a lower rate of appropriate surgical care when compared with whites (Fig. 1). Overall, the odds of receipt of appropriate thyroid surgery increased over time at a rate of 5% per year (OR = 1.05 [CI 1.04–1.06], data not shown), but the interaction term of year × race was not significant (p = 0.97), indicating that the trajectory of change over time in the adjusted odds of receiving appropriate surgery did not differ between races (Supplementary Table S1; Supplementary Data are available online at
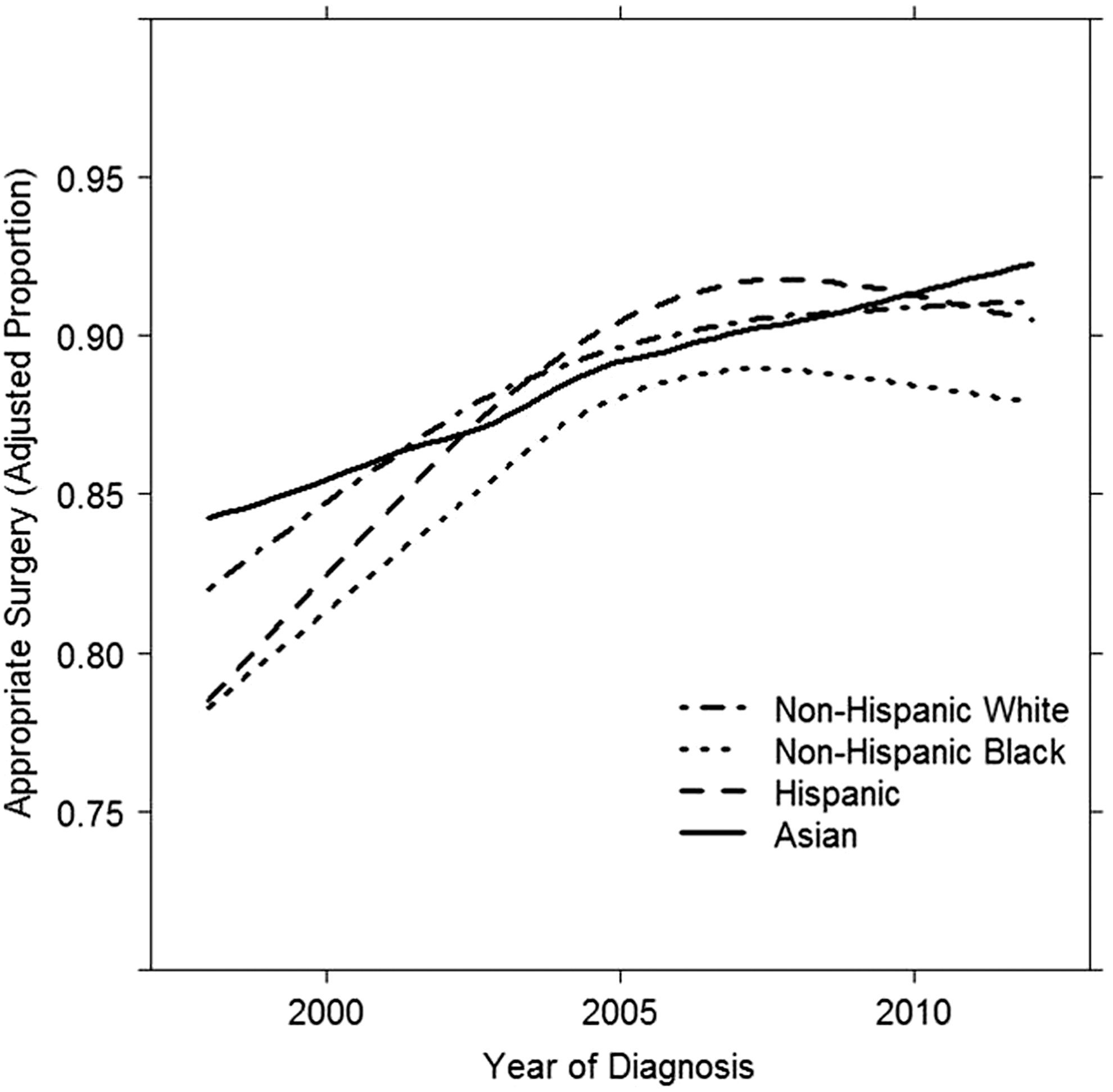
Temporal trends of adjusted proportions of patients who received appropriate extent of thyroidectomy for differentiated thyroid cancer by racial group.
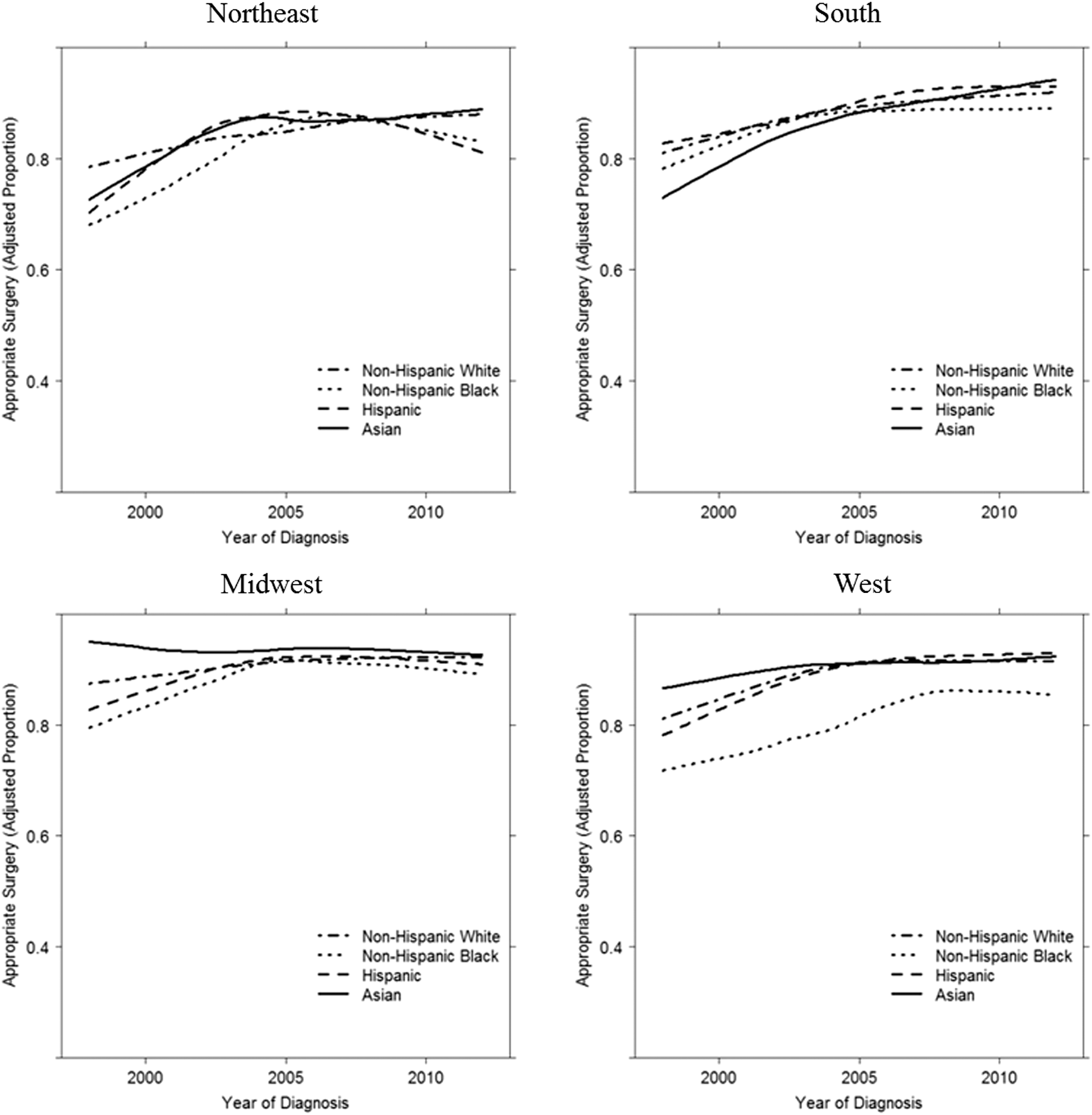
Temporal trends of adjusted proportions of patients who received appropriate extent of thyroidectomy by geographic region.
Surgery proportions are adjusted for age, sex, facility type, facility location, insurance status, income level, stage at diagnosis, and cancer type. RAI proportions are adjusted for all aforementioned covariates and tumor size, surgery type, margin status, had lymph nodes (LN) examined, and had positive LN.
Temporal trends in RAI administration
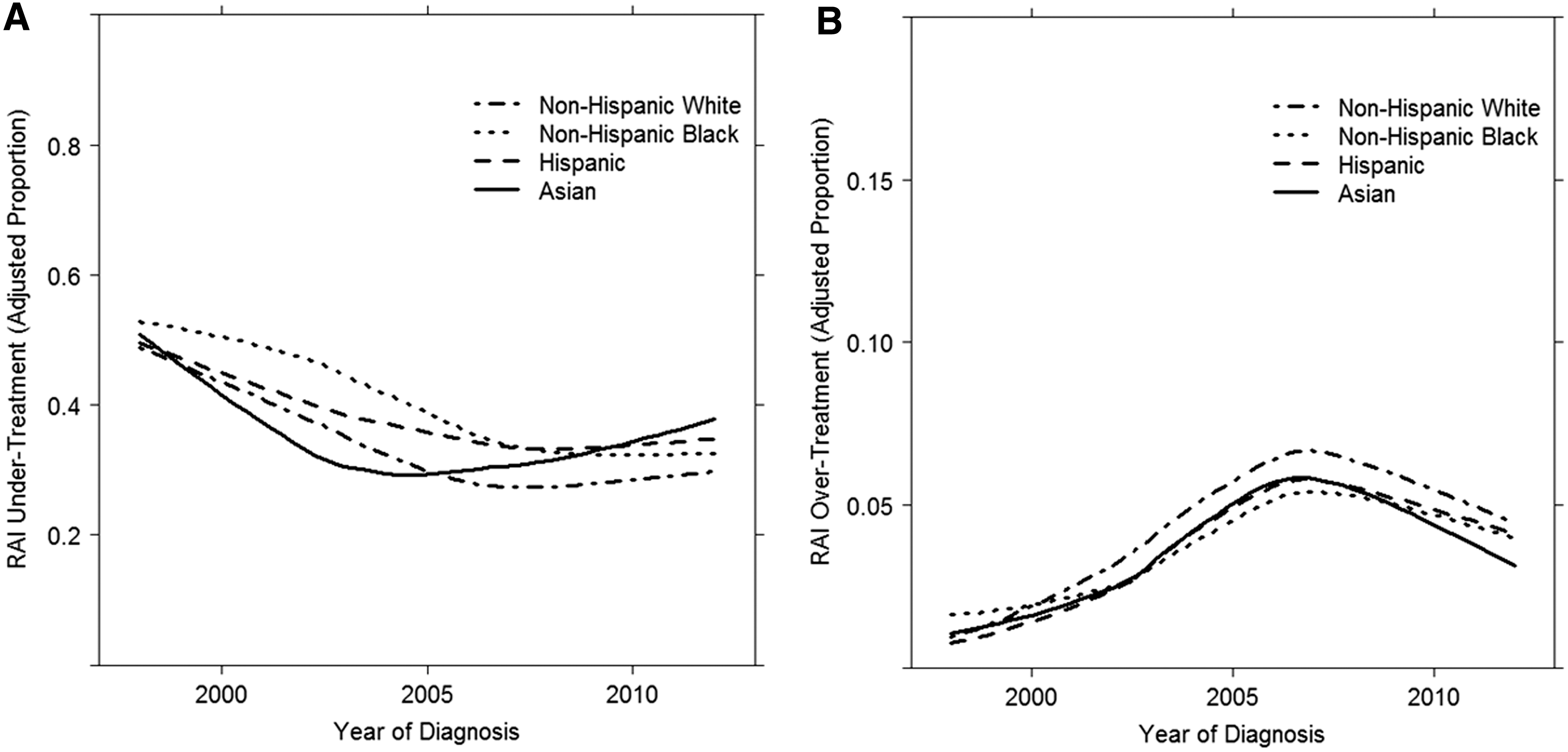
The adjusted proportion of patients who were under-treated with RAI decreased for all race groups over the study period (Fig. 3A). Compared with 1998, fewer patients were under-treated with RAI in 2012: whites (48% vs. 29%), blacks (51% vs. 33%), Hispanics (51% vs. 37%), and Asians (55% vs. 39%), respectively (Table 4). Overall, the odds of under-treatment showed a 3% decline per year (year of diagnosis OR = 0.97; p < 0.001, data not shown), and the change over time did differ based on race (interaction p < 0.001). The odds of being under-treated seemed to decline at a higher rate over time for blacks compared with whites (year × race interaction p = 0.02), whereas Asians had a lower rate of decline over time in the odds of being under-treated (Fig. 3A, year × race interaction p = 0.002; Supplementary Table S1).
Temporal trends of adjusted proportions of patients who were under-treated with radioactive iodine (RAI) therapy (
Adjusted rates of RAI over-treatment increased over time for all race groups (Fig. 3B). Compared with 1998, more patients were over-treated with RAI in 2012: whites (1% in 1998 vs. 4% in 2012), blacks (2% vs. 4%), Hispanics (2% vs. 4%), and Asians (2% vs. 3%), respectively (Table 4). The overall odds of over-treatment with RAI have been marginally increasing (year of diagnosis OR = 1.01; p < 0.001, data not shown), but the interaction term of year × race was not significant (p = 0.35), again indicating that the trajectory of change over time in the adjusted odds of receipt of RAI over-treatment did not differ based on race (Supplementary Table S1). Similar changes over time were seen in use of RAI across different geographic regions (Fig. 4).
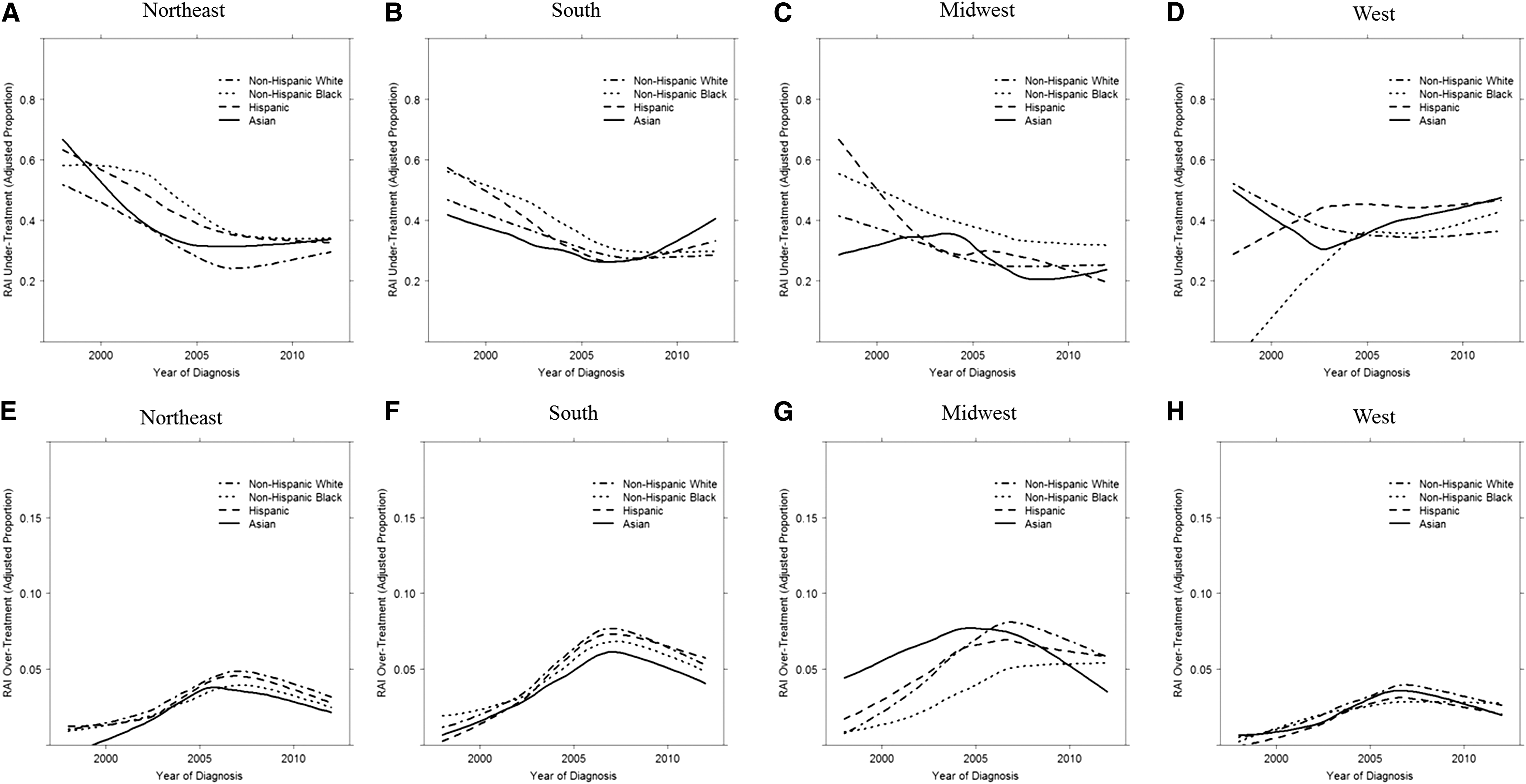
Temporal trends of adjusted proportions of patients who were under-treated with RAI (when indicated) (
Discussion
This is the first study examining temporal trends in the appropriate treatment of DTC based on patient race/ethnicity. Even though there was incremental improvement in the appropriate extent of surgery over the study period for all races, black patients continued to be at a significant disadvantage when compared with other races, and the rate of improvement for black patients lagged behind that of whites. These trends were consistent across all geographic regions, and seemed to be driven by an increase in use of total thyroidectomy instead of lobectomy for low and intermediate/high-risk disease.
A population-based study by Sosa et al. involving 16,878 patients culled from the Nationwide Inpatient Sample demonstrated an association between race/ethnicity and short-term patient outcomes following thyroid surgery. It was noted that more blacks and Hispanics underwent subtotal thyroidectomy (both 57%) compared with whites (43%; p < 0.001) (18). This study also indicated that black (53%) and Hispanic patients (55%) had compromised access to high-volume surgeons compared with whites (44%; p < 0.001). They also had longer length of hospital stay (black 2.5 days, Hispanic 2.2 days, white 1.8 days; p < 0.001), higher complication rates (black 4.9%, Hispanic 3.6%, white 3.8%; p = 0.05), and higher total hospital costs, lending credence to the concept that access to experienced surgeons may have been a mitigating factor for the observed discrepancy in outcomes. These findings were supported by another study by Noureldine et al., which demonstrated a disadvantage in access to high-volume surgeons for minorities with thyroid and parathyroid diseases (36). Compared with whites, black patients had less access to intermediate- and high-volume surgeons (49% vs. 45% and 19% vs. 16%, respectively; p < 0.001), with Hispanics having the least access to high-volume surgeons (only 13%).
It has been well documented that low-volume surgeons perform the majority of thyroid surgery in the United States, and this is associated with higher complication rates, on average (16,18,37,38). Adherence to practice guidelines has been associated with improved overall patient outcomes (16,37), and multiple studies have demonstrated that low-volume surgeons and centers are less likely to follow practice patterns that are adherent to guidelines (17,37,39). Therefore, it is possible that compromised access to high-volume surgeons combined with receipt of care that is not in accordance with national practice guidelines may indeed lead to higher rates of inappropriate treatment algorithms for minority populations. In a study of 39,687 patients, Adam et al. showed that black race and treatment at non-academic centers were associated with discordance with treatment guidelines (p < 0.01), which in turn seemed to be associated with patient survival (16).
In a study of 189,219 patients, Haymart et al. demonstrated an overall increase in the proportion of patients receiving RAI from 1990 to 2008. However, blacks were less likely to receive RAI (OR = 0.83 [CI 0.77–0.89]) compared with white patients (20). In the United States, indications for appropriate RAI treatment for DTC are recommended by practice guidelines, such as those published by the ATA and NCCN (32 –34). Famakinwa et al. examined adherence to ATA guidelines for RAI administration in the Surveillance, Epidemiology, and End Results database, demonstrating that compliance was lowest among patients >65 years of age and those who were black (p < 0.001) (24).
Over the study period, there was overall an increment in the receipt of appropriate RAI treatment, especially for blacks. However, the shift noted in RAI treatment was such that under-treatment decreased while over-treatment increased. A disadvantage of under-treatment was maintained across all minority patients compared with whites, while over-treatment with RAI was most notable for whites. Given that most of the RAI for DTC in the United States is administered by specialists (endocrinologists and/or nuclear medicine physicians), the likelihood of compliance with guidelines might be expected to be higher. This may explain the observed results in this study of bridging the gap in the appropriate use of RAI when comparing black and white patients. Nonetheless, under- and over-treatment with RAI persisted over the study period, highlighting the fact that unmeasured factors likely mitigate this observation.
Racial disparities with regard to outcomes as well as access have been observed for a number of other conditions, including cardiac disease, human immunodeficiency virus, end-stage renal disease, diabetes, cancer screening and treatment, and many surgical procedures (27,40). The Endocrine Society published a statement acknowledging potential racial bias in the treatment of endocrine diseases, specifically noting the association between more advanced presentation of thyroid cancer and lower socioeconomic status, as well as compromised access to high-volume surgeons that has been observed among ethnic minorities (17). The 2013 National Healthcare Disparity Report evaluated for the first time trends in the prevailing disparities in healthcare among ethnic minorities by measuring multiple healthcare processes, outcomes, and access between 2002 and 2011 (27). The report noted that “most disparities in quality of care related to race, ethnicity, or income showed no significant change, neither getting smaller nor larger.” Specifically related to cancer, racial disparities were persistent in relation to access, screening, and treatment over this period. The present study supports these findings overall, although with RAI treatment, incremental narrowing of disparities for some minorities was noted.
There are limitations to this study, including those inherent in the use of large administrative databases. Specifically, these include the possibility of coding errors and missing data. However, the data set used has been validated. The data set lacks certain detailed clinical information, such as radiologic information, surgical intent, patient preference, disease recurrence, and disease-specific mortality. The study demonstrates compromised 5- and 10-year overall survival among black patients, but in the absence of disease-specific survival data, it is difficult to attribute all of this difference to disparities in thyroid cancer treatment. Disease-specific survival is not available in the NCDB. Therefore, it could not be analyzed. This study represents an extensive review of a large number of patients based on contemporary population-level data, incorporating a widely representative sample of patients and providers, thereby providing credence to the findings. The reasons for the observed ethnic/racial disparities are likely multifactorial and intricate. The study could not specifically tease these out. Potential explanations for these observed disparities may include educational disparities, socioeconomic and cultural differences among races, untimely or difficult access to adequate care or experienced physicians and surgeons, and lack of adequate insurance coverage, among many others. More studies are needed to clarify with granularity the significance of association between race/ethnicity and receipt of appropriate care, with the aim of narrowing the apparent gap in quality of care.
In summary, this study demonstrates that appropriate utilization of thyroid surgery and RAI for DTC improved over the past 15 years for all racial groups. This finding is hopeful, and suggests that awareness of guidelines has increased. Given that variation in practice implies variation in care, adherence to evidenced-based guidelines is important. In addition, with growing literature confirming racial disparities in health delivery, practitioners may have become more attuned to efforts to improve quality of care for all patients. Nonetheless, the proportion of patients receiving appropriate extent of thyroid surgery was consistently lower for black compared with white patients. There was a higher likelihood of RAI under-treatment among minority groups compared with whites, whereas a higher likelihood of RAI over-treatment was observed among white patients. Given the increasing trend in incidence of thyroid cancer and the substantial costs incurred in the longitudinal care of such patients, the opportunity remains for clinicians, payers, and policy makers to work together to standardize thyroid cancer care among vulnerable minority populations.
Footnotes
Acknowledgments
The NCDB is a joint project of the Commission on Cancer of the American College of Surgeons and the American Cancer Society. The data used in the study are derived from a de-identified NCDB file. The American College of Surgeons and the Commission on Cancer have not verified and are not responsible for the analytic or statistical methodology employed, or the conclusions drawn from these data by the investigators.
Author Disclosure Statement
Julie Ann Sosa is a member of the Data Monitoring Committee of the Medullary Thyroid Cancer Registry, funded through UBC by GlaxoSmithKline, NovoNordisk, Astra Zeneca, and Eli Lilly. No competing financial interests exist for the remaining authors.