
Abstract
Background:
Historical anaplastic thyroid cancer (ATC) outcomes have been terrible, with a median survival of only five months and <20% one-year survival. Improved outcomes are now achieved with aggressive initial therapy in stages IVA and IVB disease, but patients with distant metastatic disease (stage IVC) still do poorly; improved therapies are sorely needed. Kinase inhibitors have emerged as promising agents in the therapy of advanced medullary and differentiated thyroid cancer, but there are limited data regarding the use of lenvatinib in ATC. The aim of this study was to delineate clinical outcomes in a series of patients with advanced ATC in response to lenvatinib therapy.
Methods:
A retrospective analysis was conducted involving all lenvatinib-treated Mayo Clinic ATC patients in 2015.
Results:
Of 28 distinct ATC patients seen in 2015, three (11%) with metastatic disease of ECOG performance status 2–3 were treated with lenvatinib. Two patients were male; age range at ATC diagnosis was 57–84 years. All three patients attained successful local control of their disease with surgery and/or combined chemoradiotherapy. Lenvatinib was offered as the second, third, or fourth line of therapy at the time of metastatic disease progression. Two patients incurred minor responses to therapy, with structural regression of distant metastatic tumor disease soon after starting lenvatinib treatment (at one to two months), while one patient achieved stable disease, but no Response Evaluation Criteria In Solid Tumors partial responses resulted. Overall survival after starting lenvatinib was two, six, and seven months. Fatigue and hypertension were prominent, and one patient developed pulmonary emboli while on lenvatinib.
Conclusion:
This initial single-institution experience suggests that lenvatinib may have some disease-modifying activity in metastatic ATC that is otherwise refractory to cytotoxic chemotherapy. Unfortunately, observed benefits were transient, and toxicities were prominent. Clinical trials are required to ascertain better the utility of lenvatinib in the management of advanced ATC.
Introduction
I
A 50-year experience of 134 cases of ATC treated at the Mayo Clinic between 1949 and 1999 demonstrated median survival of only three months overall (4). Postoperative radiotherapy was associated with slightly longer median survival (5 vs. 3 months), but this was not statistically significant (p < 0.08). Multimodality therapy, including operation, chemotherapy, and radiotherapy, was not associated with improved survival in this initial study.
In an analysis of the Surveillance, Epidemiology, and End Results (5) data, overall ATC survival at two and five years was 12.9% and 7.5%, respectively, with a median survival of only four months. Patients with disease confined to the thyroid with no extension beyond the capsule (stage IVA) had two- and five-year overall survival rates of 32.7% and 22.9%, respectively, and a median survival of nine months. With disease extension into adjacent tissue (stage IVB), median survival was six months, and overall survival was 16.2% and 10.1% at two and five years, respectively. Median survival for patients with further extension or distant metastatic disease (stage IVC) was three months, with a two-year overall survival rate of 2.1%.
A small series of 10 consecutively treated stage IVA and IVB ATC patients at the Mayo Clinic (6) demonstrated apparently improved outcomes with combination intensity-modulated radiotherapy (IMRT) and radiosensitizing chemotherapy; overall survival was 70% and 60% at one and two years, respectively. At last follow-up, 50% of patients were alive, followed for a minimum of 32 months. The reasons for the benefits observed in this second Mayo Clinic study might be attributable to interval “innovations” such as IMRT, addition of taxane chemotherapy (to prior anthracycline-only treatment), and the use of adjuvant chemotherapy cycles in addition to only that required for radiosensitization. However, these outcomes are only relevant to patients with stages IVA and IVB locoregionally confined disease at diagnosis. Extension of this initial experience is underway, with similarly positive outcomes observed in a subsequent series of patients (7). However, the impacts of an aggressive initial therapeutic approach appear greatest in patients with less extensive disease at diagnosis.
Unfortunately, it is very frequent for ATC patients to present with, or later develop, distant metastases, wherein outcomes are very poor, and therapies have low efficacies. For example, at the Mayo Clinic, 46% of patients had evidence of metastases at diagnosis (4) and experienced consequently very poor prognosis and median survival of less than three months. These patients have not been effectively salvaged using available therapies.
Newer approaches for the management of ATC are desperately needed. Although taxanes, combretastatin family members, and anthracyclines have some activity in advanced ATC, responses to cytotoxic chemotherapy are typically short-lived (8). Within the last several years, kinase inhibitors have emerged as promising agents in the therapy of advanced medullary thyroid cancer (MTC)] (9 –11) and DTC (12,13), but efficacy in ATC has been discouraging to date. For example, the clinical effects of the kinase inhibitor pazopanib were recently assessed in ATC in conjunction with a prospective Phase 2 open-label clinical trial (8); no confirmed Response Evaluation Criteria In Solid Tumors (RECIST) were observed among 15 treated patients, despite a 49% response rate in DTC. Moreover, several impressive but transient tumor responses were observed among pazopanib-treated ATC patients, but the median time to progression was only 62 days and the median survival 111 days.
Lenvatinib is a multitargeted inhibitor of kinases, including VEGF receptors [1–3], FGF receptors [1–4], PDGFRα, KIT, and RET, and has recently been approved by the Food and Drug Administration for the treatment of advanced iodine-refractory DTC in February 2015 (13). In the lenvatinib SELECT Phase 3 study (13) of patients with advanced DTC, median progression-free survival in the lenvatinib group was 18.3 months compared to 3.6 months in the placebo group. In a separate Phase II Japanese study of lenvatinib in advanced thyroid cancers, 11 patients with ATC received treatment with lenvatinib, with responses seen in three patients (14). Given the high response rates of lenvatinib in DTC and the durable responses reported among a small number of ATC patients treated in conjunction with early lenvatinib trials, this drug may have promise in ATC as well, but it has yet to be rigorously tested.
Since ATC is an extremely aggressive disease with an urgent need to improve outcomes and therapies, this study investigated the few patients with ATC who have been treated with lenvatinib via “off-label” use at the authors' institution administered. The objective was to delineate clinical outcomes among patients with metastatic ATC treated with lenvatinib in this setting.
Methods
All ATC patients treated with lenvatinib at the Endocrine Oncology clinic at the Mayo Clinic, Rochester, MN, in 2015 were eligible for analysis. The study was approved by the Mayo Clinic Institutional Review Board. Demographic, clinical, laboratory, radiologic, and pathology data were extracted from the electronic medical record, and a retrospective analysis was conducted. ATC patients were staged using AJCC 7th edition TNM (15) as stage IVC. Descriptive analyses were used to present outcomes, given there were only three eligible patients. RECIST response was calculated as a percentage of baseline/pre-lenvatinib RECIST tumor measurements, with best RECIST response being the lowest percentage calculated at any point after lenvatinib initiation.
Results
During 2015, 28 distinct patients with ATC were seen at the Mayo Clinic Rochester site. Of these, three (11%) with metastatic, progressive, and therapy-refractory ATC of ECOG performance status 2–3 were treated with lenvatinib. Case summaries of each patient are provided below.
Patient 1
A 67-year-old male presented with sudden voice hoarseness due to a left paralyzed vocal cord, with a 5 cm fluorodeoxyglucose positron emission tomography (FDG-PET)-positive left thyroid mass and pulmonary metastases identified in October 2014, initially thought to be poorly differentiated thyroid carcinoma (PDTC) and considered unresectable. He was treated with prophylactic tracheostomy and chemoradiation with two cycles of carboplatin and paclitaxel and IMRT with 6600 cGy in 33 fractions elsewhere, with some decrease in the size of the neck tumor but with progression of pulmonary metastases. This initial therapy was complicated by urosepsis, dehydration, and requirement for temporary percutaneous gastrostomy tube (PEG) placement. Four months after initial diagnosis, he was first seen at the Mayo Clinic. Pathology was revised from PDTC to ATC. A total thyroidectomy was performed on May 7, 2015, with a 4.8 cm × 4.3 cm × 2.6 cm ATC arising from PDTC, with Hürthle cell features replacing the entire left lobe. Due to the presence of lung metastases, his initial staging was considered as TNM stage IVC. An abscess necessitated broad spectrum antibiotic treatment. Therefore, second-line chemotherapy was not elected as the next step for therapy. He was thus treated with 24 mg/day of lenvatinib, with minor disease regression of lung metastases resulting at 35 days, but with a best RECIST response of 99.4% of baseline (Fig. 1A).
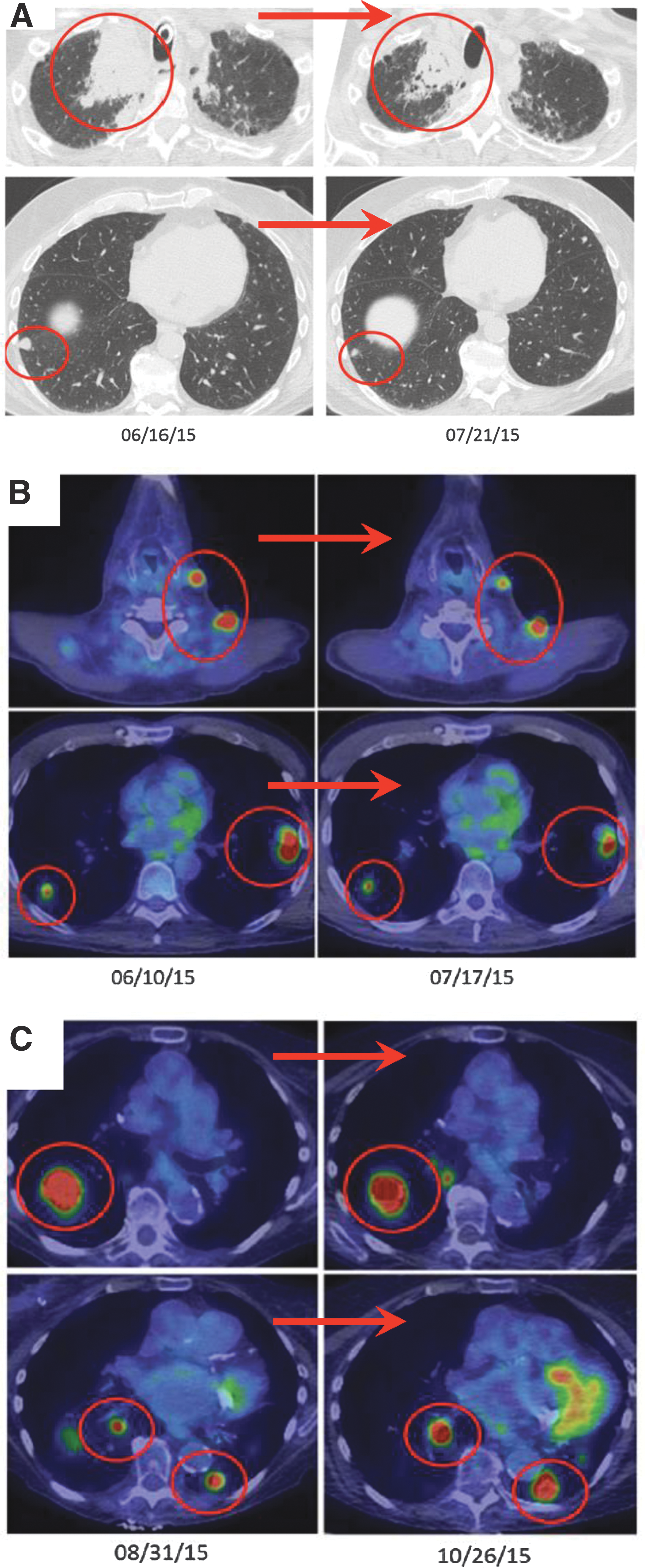
Cross-sectional and fluorodeoxyglucose positron emission tomography (FDG-PET) images in response to lenvatinib therapy in anaplastic thyroid carcinoma patients. (
Soon after starting lenvatinib, his blood pressure increased to >150 mm HG systolic, with medication adjustments needed. Amlodipine was added, and lisinopril was dose-adjusted. Due to nausea, vomiting, and dehydration requiring hospitalization, a dose reduction was required. At a lenvatinib dose of 10 mg/day, he incurred significant disease progression, but with an incremental increase to 20 mg/day, disease control was reestablished. Due to limit tolerability to the medication, however, dose reductions were needed to 14 mg/day and then to 10 mg/day. At this later dose, tolerance was improved, but disease progression occurred, and lenvatinib was discontinued.
Temsirolimus was used next based in part upon the presence of an NF1 mutation (Table 1; NF1 T1052fs*8) as third-line medical therapy, with a best RECIST response of stable disease lasting less than eight weeks in duration. His quality of life and functional status declined rapidly thereafter, and palliative therapy was elected, with death occurring 19 days later.
Bold text indicates potential rationally targetable mutations.
IMRT, intensity-modulated radiotherapy; SBRT, stereotactic body radiation therapy.
Patient 2
A 57-year-old male presented with anterior left neck enlargement and left jaw neck pain. Further evaluation revealed a 5 cm left thyroid mass, intensely hypermetabolic on FDG-PET, with gross extrathyroidal extension (ETE). He underwent total thyroidectomy, demonstrating an 8.5 cm ATC with gross ETE invading the internal jugular vein (IJV) and N1b disease (stage IVB). He was treated with combined chemoradiotherapy (weekly docetaxel-doxorubicin [20 mg/m2 each intravenously (i.v.)] and 6600 cGy in 33 fractions) with a good initial response. However, temporary PEG placement was needed due to radiation-induced mucositis and difficult-to-control secretions. Surgical drainage of a superficial abscess in his previous surgical incision was also required. Seven months after diagnosis (four months after radiotherapy), he developed lung and other distant metastases, initially treated focally with cryoablation and/or radiotherapy. Eight months after diagnosis, he developed diffuse disease progression and was re-treated with docetaxel and doxorubicin, with initial disease control reestablished.
Ultimately, further disease progression prompted lenvatinib therapy at 24 mg/day, reestablishing structural disease control with a best RECIST response of 83.6% from baseline, with the largest pulmonary lesion within the lateral left lower lobe decreasing in FDG avidity from 11.8 to 4.5 SUV, and new lesional central necrosis consistent with response to interval therapy (July 2015; Fig. 1B). Due to development of an interval pulmonary embolism, lenvatinib was discontinued transiently. During this period, his disease rapidly and symptomatically progressed. Lenvatinib re-initiation (September 2015) reestablished disease control.
On further follow-up (November 2015), he started to have a more mixed response to lenvatinib, but with net disease progression and increased pain, with a new hemorrhagic metastatic lesion involving the pons and a new cerebral metastasis treated focally with stereotactic radiosurgery (gamma knife). He continued to tolerate lenvatinib at full dose (24 mg/day) with modest nausea treated occasionally with ondansetron. Due to progression, a biopsy (November 2015) of a soft-tissue para-spinal metastasis was done, yielding two possible targetable mutations (Table 1; NF1 and PTEN loss). NF1 and PTEN could both potentially increase the probability of response to mTOR inhibition with everolimus or temsirolimus, and NF1 could also be targeted with cobimetinib and trametinib treatment. However, by the time these results became available, the patient had elected palliative care. The patient died seven days after entering the hospice.
Patient 3
An 84-year-old woman presented with a rapidly enlarging neck mass, ear discomfort, and a harsh voice. Imaging revealed a right 7 cm thyroid mass with gross ETE, seen associated with numerous malignant-appearing lymph nodes and lung metastases (stage IVC). Her cancer was deemed unresectable at presentation due to tumor invasion of the right IJV, encasement of the right internal carotid artery, invasion of the right cricoid and thyroid cartilages, and further spread through the thyroid/hyoid membrane.
She received initial chemoradiotherapy with weekly paclitaxel-carboplatin (50 mg/m2 and 2 AUC, respectively, i.v.) and IMRT 6600 cGy in 33 fractions, with good local response with frank diminished of bulky lymphadenopathy resulting. However, chemoradiotherapy was complicated by mucositis, skin irritation, dysphagia, and inability to swallow, with a temporary need for PEG placement. Four weeks after finishing chemoradiation, her lung metastases started to progress. She was treated with docetaxel and doxorubicin (20 mg/m2 each weekly i.v.) with no benefit. Lenvatinib (24 mg/day) was initiated as third-line treatment, but dose reductions were required due most notably to disabling fatigue. She also developed easily managed hypertension and transient mild thoracic erythematous cutaneous rash. Mixed effects on lung metastases were noted in response to intermittent treatment with lenvatinib at lower doses. Her best RECIST response was of 108% from baseline, but there was evidence of central cavitation of lung metastases. She ultimately developed brain metastases, for which she received stereotactic radiosurgery, with marked clinical improvement ensuing. Lenvatinib was stopped just before gamma knife treatment and was not resumed. Hospice care was elected, and the patient died 27 days after cessation of lenvatinib.
Discussion
This article describes the authors' initial clinical experience with “off-label” use of lenvatinib for the treatment of metastatic ATC in the salvage setting. The objective was to delineate clinical outcomes among a series of ATC patients treated with lenvatinib at the Mayo Clinic.
In two of the three patients, there was a minor structural response to lenvatinib therapy (Fig. 1A and B) on cross-sectional imaging soon after starting lenvatinib treatment (at one to two months). In the third case, there was a mixed response to therapy (Fig. 1C). No RECIST partial or complete responses were observed. Interestingly, minor responses were seen in the younger male patients with relatively better tolerance to the medication compared to the third case, an elderly woman with very poor tolerance of the medication. Overall survival after lenvatinib initiation was seven, six, and two months for cases 1, 2, and 3, respectively, with the eldest and most frail patient having the shortest survival.
Lenvatinib required dosage reduction in two of the three patients. Overall, the most significant and difficult-to-manage adverse reaction to lenvatinib was fatigue, with cases 1 and 3 experiencing (CTCAv4) grade 3 fatigue (16). Unlike sorafenib (12), a rash was not a significant issue with lenvatinib therapy in this small case series. Consistent with the side-effect profile reported for DTC patients treated with lenvatinib (13), hypertension was a common adverse reaction.
The retrospective nature of this study and small sample size prevent robust conclusions from this experience. Lenvatinib showed some activity in ATC, but responses/disease control was brief. A clinical trial is thus required to assess more comprehensively the utility of lenvatinib in the treatment of metastatic ATC. Such a trial is presently activating (NCT02657369).
Conclusions
This article presents the authors' initial experience with the “off-label” use of lenvatinib for the treatment of ATC. This initial experience suggests that lenvatinib has potential disease-modifying activity in metastatic ATC that is otherwise refractory to cytotoxic chemotherapy and radiotherapy. Unfortunately, observed benefits were transient, with survival ranging from two to seven months from time of lenvatinib initiation. Clinical trials are required to ascertain better the utility of lenvatinib in the management of advanced ATC (NCT02657369 is activating presently).
Footnotes
Acknowledgments
We are thankful to Eisai for facilitating off-label use of lenvatinib for our patients, to Ms. Candace Kostelec for administrative assistance, and to our patients for entrusting us with their care and for their provision of ongoing inspiration. Dr. Iñiguez-Ariza is also indebted to the Fundación para la Salud y la Educación Dr. Salvador Zubirán A.C. (FunSaEd) and to the Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán (INCMNSZ), Mexico City, Mexico, for generous Fellowship support enabling her studies at the Mayo Clinic. This study was presented in part at the 2016 Annual Meeting of the Endocrine Society, Boston, MA (paper 26540).
Author Disclosure Statement
The authors have no disclosures.