
Abstract
Background:
Thyroid carcinoma is rare in young children, with a sharp increase in incidence among adolescents and young adults between 15 and 29 years of age. The incidence of thyroid carcinoma is increasing worldwide. Limited prospective population-based data are available to describe diagnostic and treatment practices in this age group. This study undertook a population-based review of thyroid carcinoma among 0- to 29-year-old individuals in Ontario, Canada, utilizing linked administrative data to describe the demographic and care patterns over nearly two decades.
Methods:
Cases from the Ontario Cancer Registry were identified and linked to administrative data sources at the Institute for Clinical Evaluative Sciences. Cases diagnosed prior to a patient's 30th birthday between 1992 and 2010 were considered eligible. Billing records identified ultrasonography, fine-needle aspiration biopsy, radioiodine therapy, and surgical approach.
Results:
A total of 2552 patients aged 0–29 years were diagnosed with thyroid carcinoma during the study period. There was a 2.1-fold increase in standardized incidence rate over the 19 years of this study. Thyroid carcinoma was diagnosed subsequent to a prior malignancy in 47/2552 patients at a median interval of 11.6 years after initial cancer diagnosis. Seventeen individuals developed a second malignancy after treatment for thyroid carcinoma. Most patients (90.44%) underwent preoperative ultrasound (ranging from 1 to 13 preoperative studies). Preoperative thyroid scintigraphy was used in 44% of patients, with a significant decline in usage over the study period. Fine-needle aspiration biopsy usage rose by 20% over the study period, although 26% of patients had no biopsy prior to surgery. Primary total thyroidectomy followed by two-stage thyroidectomy were the most frequently performed procedures, and 56% of patients received therapeutic radioiodine.
Conclusions:
This study establishes a foundation of diagnostic and practice patterns over nearly two decades. The study corroborates, in the Ontario population, the rising incidence of thyroid carcinoma in children and adolescents and young adults. Finally, it identifies the use of multiple preoperative ultrasound studies, low rates of thyroid biopsy, and thyroid scintigraphy as targets to improve efficiencies of care and to reduce unnecessary healthcare expenditures through education, standardization of diagnostic approach, and possibly regionalization of care.
Introduction
D
Papillary thyroid carcinoma (PTC) represents approximately 85% of all DTC cases among children and AYAs (3). Several clinical features distinguish it from disease in older individuals. PTC in children is more frequently regionally and distally metastatic and more likely to recur when compared to DTC in adults (reviewed by Rivkees and Dinauer) (4). As such, it merits distinct consideration from adults. Moreover, aspects unique to childhood, adolescence, and young adulthood obligate a dedicated examination of treatment and outcome variables in this group. Specifically, (i) a large proportion of this population is treated at pediatric centers, with substantially lower volumes than at centers that treat adult DTC (5); (ii) patients frequently undergo transition of care to adult centers during the follow-up period; and (iii) despite clinical distinctions with DTC in adults, there have historically been no clinical guidelines for younger patients that individualize treatment based on the distinct features of disease in this age group.
In 2015, the American Thyroid Association (ATA) published the first guidelines for the assessment and treatment of children and adolescents with DTC (6). These guidelines emphasize the importance of preoperative assessment to guide surgical planning (as do parallel adult guidelines) (7,8). Additionally, these guidelines mark a significant paradigm shift in approach to postoperative care of children with thyroid malignancy, adopting a risk-stratified strategy to drive surveillance and radioiodine therapy, whereby those patients with greatest risk for persistent disease (patients with significant central neck or lateral neck lymph node metastases) undergo the most aggressive treatment and follow-up. Finally, several recent studies have established the importance of surgical volume in driving quality measures such as length of stay and complication rates (5,9). To assess the impact of these guidelines on patterns of care and resource utilization, the current study was conducted to define the baseline status at a provincial population level, prior to the introduction of these guidelines, to help inform and guide further care and health-resource utilization.
DTC diagnosed in younger patients almost invariably follows an indolent course, with 30-year survival rates >90% (3), although lifelong disease surveillance is advocated (6). The intersection between young age at diagnosis and high survival establishes a large and growing cohort of long-term survivors who are at risk for primary disease recurrence and late sequelae of PTC diagnosis and/or treatment.
The incidence of DTC is rising more rapidly than any other malignancy worldwide in both pediatric and adult populations (10 –14). By 2019, PTC is projected to become the second most common cancer among women <45 years of age in the United States, with a cost to the healthcare system of between $2.1 and $3.1 billion (15). Although many have argued that this increase is attributable to increased diagnostic scrutiny in the context of improved quality and more widespread access to ultrasound and fine-needle aspiration biopsy, several arguments counter this as a sole explanation for the rise. First, if diagnostic scrutiny were the exclusive cause of the rising incidence, a plateau in incidence would be expected as emergent technologies saturated the prevalent cases in the population. To date, this has not proven to be the case, and incidence continues to rise. Second, if rising use of diagnostic imaging was the exclusive cause of the apparent increase, one would expect a shift toward detection of smaller tumors, with a concomitant diminution in large tumors. Several reports have shown that rates in all tumor sizes have increased (10,16 –18). Thus, there does appear to be a true rise in new cases of DTC.
With rising incidence and prolonged survival, an understanding of the demographics, epidemiology, and treatment patterns is essential to understand the societal burden of thyroid cancer in this population and to align resources, inform policy, predict clinical needs, and define optimal treatment paradigms.
This study reports a complete, unbiased, population-based analysis of thyroid cancer in 0- to 29-year-old individuals over a 19-year period in Ontario, Canada. Ontario is a single-payer health system, with centralized billing of physician services and diagnostic testing. Data were derived from a provincial cancer registry and administrative health databases, which capture billing, hospital admissions, emergency department visits, procedures, and laboratory testing. We describe the demographics, incidence trends, and diagnostic patterns over nearly two decades in this population.
Methods
Data sources and study population
A retrospective population-based cohort was established using the Ontario Cancer Data Linkage (CD-LINK) project, an initiative of the Ontario Institute for Cancer Research and the Health Services Research Program of Cancer Care Ontario (19). The Institute of Clinical and Evaluative Sciences deterministically links data sources using a unique encrypted health insurance number assigned to every person eligible for health insurance coverage in the province of Ontario. The Ontario Cancer Registry (OCR) (20), a population-based provincial registry of all incident cases of cancer, was linked to administrative data. Thyroid cancer diagnoses among children and AYAs were identified using the International Classification of Disease (ninth edition) code 193 for malignant neoplasm of the thyroid gland. Confirmed thyroid cancer cases from the OCR were restricted to those diagnosed at <30 years of age from January 1, 1992, to December 31, 2010. Only cases that had the highest level of diagnostic certainty were included and were identified from the OCR by source records ascertained by either a Regional Cancer Centre Registration (R) or by confirmed Pathology report (P). ICD-O histology codes (21) pertaining to the diagnosis of thyroid cancer available from the cancer registry were grouped into the following categories: papillary (8050, 8140, 8260, 8341–44, 8350); follicular-variant papillary (8340); follicular (8290, 8330, 8331, 8335); medullary (8510, 8246, 8345, 8511); and other (8337, 8347) (22). A total of 208 thyroid cancer cases were excluded for the following: Hospital Medical Records Institute or Inpatient/Same Day Surgery records were the only contributing sources of diagnostic information (n = 67); cases with histology codes of 8000, 8001, 8010, 8052, 8070, 8130, 8323, 8430, 8504, 9080, 9260, or 9750 (n = 39) wherein histology was ambiguously coded (i.e., “neoplasm”) or non-endocrine/non-epithelial malignancies (i.e., teratoma, sarcoma, etc.); or cases with unknown/unidentified cancer definitions (9990; n = 102). Given a variable interval between the time of clinical presentation and definitive diagnosis, age at diagnosis was defined as the patient's age at the time of initial thyroid surgery. Fine-needle aspiration biopsy was not considered adequate to establish a definitive diagnosis. While incident medullary thyroid carcinoma (MTC) cases were captured for the purposes of demographics (Table 1), these cases were excluded from analysis of secondary thyroid malignancies and second primary malignancies following thyroid cancer due to association of MTC with hereditary cancer syndromes, which would otherwise confound the analyses. Health service utilization data from five years prior to the diagnosis of thyroid cancer and follow-up data, including deaths, were ascertained until December 31, 2012. Comparison to population rates was achieved using a 5% age- and sex-matched random sample of the Ontario population during this study period. Ethics approval was obtained from the Research Ethics Board of The Hospital for Sick Children, Toronto, Canada.
For confidentiality reasons, some cells have been suppressed due to small cell sizes, as indicated by —.
p-Value computed using chi-square or Fisher's exact test for categorical data between male and female groups.
“Primary” thyroid cancer refers to patients where thyroid malignancy was the sole or initial malignancy and excludes individuals with a prior non-thyroidal malignancy.
“Other” histology includes insular and mixed medullary–papillary thyroid carcinoma.
N = 13 patients missing income, total number is based on 2539 patients.
Covariates
The Ontario Health Insurance Plan database (OHIP) contains a record of all fee-for-service interactions with the health system. The service being billed is identified through billing codes established by the provincial health ministry (23). Patients were considered to have experienced diagnostic interaction if a consultation or procedure with a specific billing code was identified on or before the diagnosis date of thyroid cancer (index date) for the following: endocrinology consultation (A007), thyroid scintigraphy (J818, J618, J671, and J871), use of ultrasonography excluding vascular studies (J105 and J405), and aspiration biopsy (Z726, Z727, Z771, and L805). Patients were considered to have experienced a treatment interaction if a procedure or treatment with a specific billing code was identified on or after the diagnosis date of thyroid cancer (index date) for the following: radioiodine therapy (X326), total thyroidectomy (S788), subtotal thyroidectomy (S789), hemi-thyroidectomy (S790), parathyroid(s) reimplantation (E880), and lymph node dissection (R910, R915, Z405, and Z406). These codes do not distinguish central from lateral cervical lymph node dissection.
Neighborhood income quintiles were determined by linking Canadian Census data from the census closest in time to each diagnosis date based on the postal code of residence at the time of diagnosis. The Statistics Canada postal code conversion software (24) was used to link the full six-digit postal code at the time of diagnosis to a Dissemination Area (DA; Enumeration Area [EA] prior to 2001), which is defined by Statistics Canada to be the smallest unit of geography that comprises a population of between 400 and 700 persons. The temporally nearest census to the diagnosis date was used to select the appropriate EA/DA. The census provides the average household income within the EA/DA based on a 20% sample of households. To control for differing household sizes within each EA/DA, an adjustment for household size was performed to generate the average income per single-person equivalent within the EA/DA. The details of the calculation of income per single person equivalent have been described elsewhere (25). To account for variability in the cost of living within the province, quintiles of neighborhood income were constructed within defined areas of the province (by census metropolitan area or census agglomeration area) (24,26). Urban and rural status was also identified by using the postal code at the time of diagnosis.
To preserve individual anonymity, cells of five or fewer individuals were suppressed.
Statistical analysis
Using the thyroid cancer case cohort from the OCR, direct age-standardized incidence rates of new cases per 100,000 per year were calculated using the 1991 Total Canadian Population (version 2) standard population provided by Statistics Canada (27). Incidence rates were calculated yearly and for four periods (1992–1995, 1996–2000, 2001–2005, and 2006–2010). All incidence rates were stratified according to sex. The confidence intervals (CI) were calculated using a Poisson distribution. Statistical calculations were performed using the SAS v9.2 (SAS Institute, Inc., Cary, NC).
Results
A description of the cohort stratified by sex is provided in Table 1. There were 2552 individuals diagnosed with thyroid cancer over the 19 years of the study. Overall, the female:male ratio was 4.6:1, although younger children (<13 years) presented at a ratio of 1.5:1. Statistically significant differences by sex were noted with histological type (p < 0.01), age at diagnosis (p < 0.01), income quintile at diagnosis (p = 0.03), and death (p < 0.01). Males are diagnosed less frequently with follicular-variant papillary thyroid carcinoma (FV-PTC) compared to females (23% vs. 30%), tend to be younger at diagnosis (22% of males diagnosed at <20 years of age vs. 17% of females), and occupy a higher income quintile (24% of males are in the highest income quintile vs. 17% of females).
Over the 19-year period, the age standardized incidence rate (ASIR) increased 2.1-fold (2.1 in females and 1.8 in males). The difference in the incidence between males and females has remained four to five times higher in females over the period (Table 2 and Fig. 1). Stratification of ASIR by age group (Fig. 2) confirms increasing incidence in all age categories, with the highest increase in those diagnosed at >19 years of age. Also noted were a significant increase in FV-PTC and a decrease in follicular carcinomas over time (data not shown).
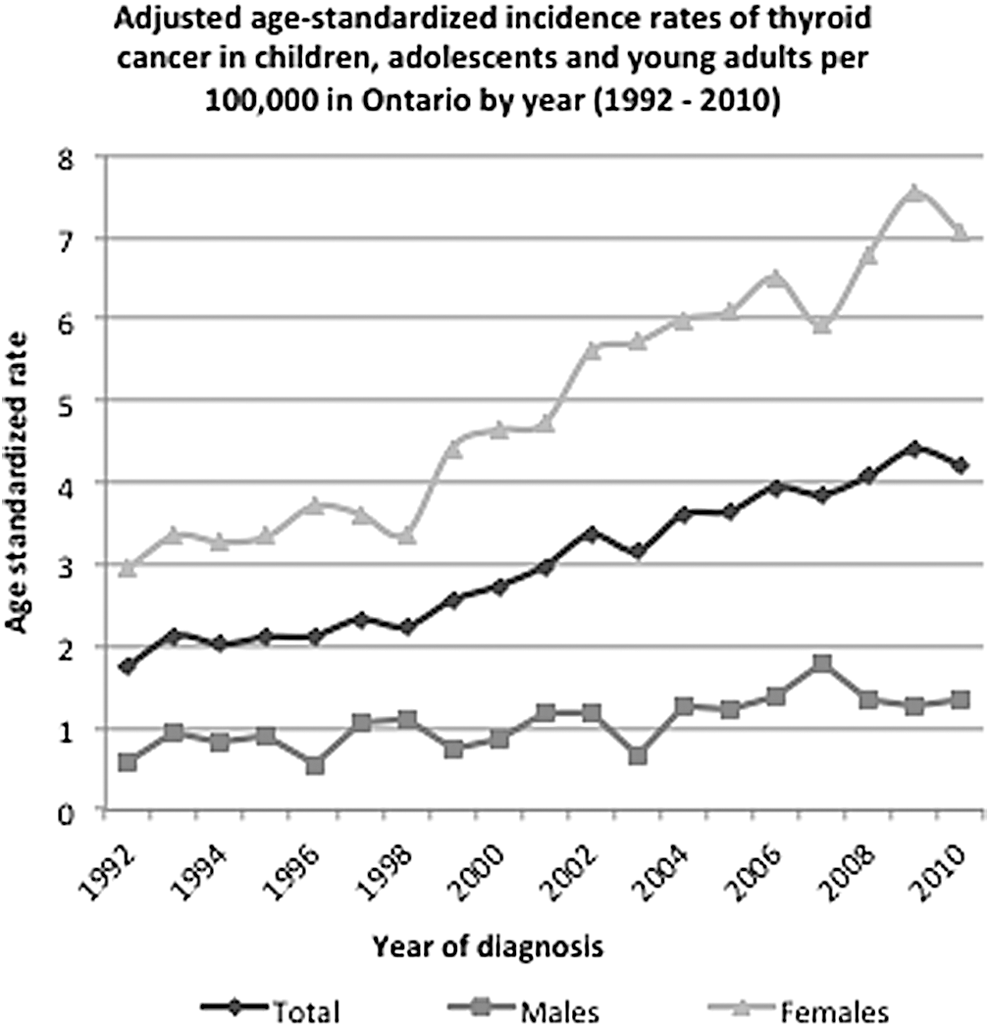
Adjusted age-standardize rates of thyroid cancer in children, adolescents, and young adults per 100,000 in Ontario by year (1992–2010).
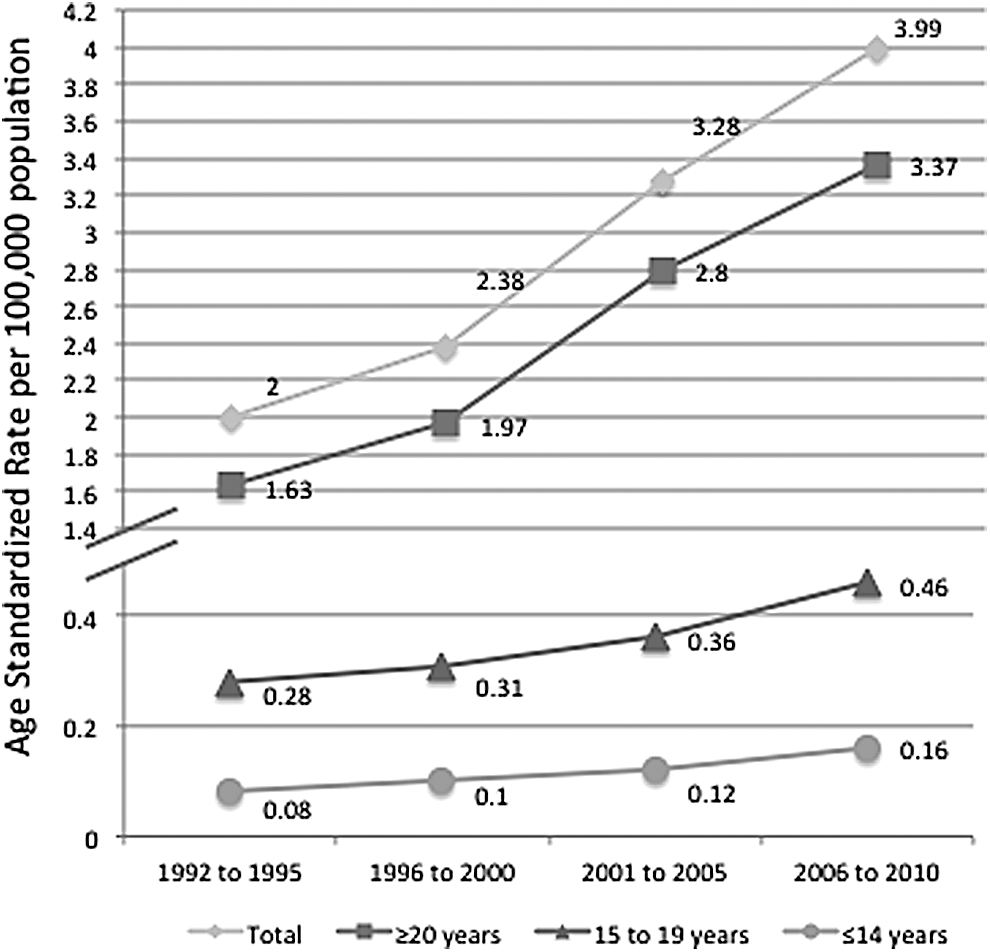
Age-standardized incidence rates by age category.
Incidence rate (IR) per 100,000.
Poisson approximation (Chiang formula).
Bains, Namrata. Standardization of Rates. APHEO. March 2009.
1991 Census Canadian population structure.
CI, confidence interval.
Multiple malignancies
In 1.8% (47/2552) of cases, thyroid cancer was not the primary neoplasm diagnosed. Primary malignancies were predominantly hematologic and central nervous system (n = 31). The median interval between the primary malignancy and diagnosis of thyroid carcinoma was 11.6 years (range 0.1–24.1 years). PTC was the histologic type in 94% of these cases. There was a 2.1-fold excess of secondary thyroid malignancy in males versus females (p = 0.01).
Additionally, there were 17 (0.66%) individuals diagnosed with primary PTC who developed subsequent primary malignancies (SPMs) at a median of 4.1 years (range 0.1–15 years) following treatment for PTC or FV-PTC. Eight SPMs were carcinomas, while other diagnoses included lymphoma, melanoma, and germ cell tumor. Ten patients with secondary non-thyroidal malignancies had previously received radioactive iodine (RAI) and developed secondary malignancies on average 3.2 years after RAI therapy (range −0.69 to 7.8 years). In contrast, the mean latency to second malignancy among those without RAI exposure was 7.3 years (range 0.5–15 years). The resultant odds ratio for a second primary malignancy following RAI treatment was 1.41 [CI 0.59–3.37]. There was no difference in the distribution of second cancer site or histology between those who received RAI and those who did not, although this study was underpowered to detect significant differences.
Mortality
There were 15 deaths in this pediatric and AYA population during the course of the study (587/100,000 [CI 329–952]) compared to an expected rate of 415/100,000 in the age- and sex-matched general population, for an excess mortality ratio of 1.4. Death occurred at a median of 3.1 years after diagnosis of thyroid carcinoma. Cause of death was not recorded for five individuals, while for six patients, death was unrelated to malignancy. Details related to cause of death were otherwise unavailable or redacted to maintain anonymity due to the rarity of such events. Thirteen patients had thyroid carcinoma as their sole malignancy. Males were 9.2 times more likely to die compared to females.
Diagnostic modalities
Details of diagnostic (preoperative) procedures are provided in Table 3. Overall, 44% of patients underwent preoperative thyroid scintigraphy, with a significant decline in use over the observation period (p < 0.01) and only 30% undergoing scintigraphy in the most recent period. Young adults (aged 20–29 years) were more likely to have undergone scintigraphy than children and adolescents were (46% vs. 36%).
p-Value computed using Cochran–Armitage trend test or chi-square test where appropriate.
In contrast, >90% of patients underwent at least one preoperative ultrasound, with a small but significant increase in use over the observation period (p < 0.001). A substantial proportion of patients underwent multiple preoperative ultrasounds (Fig. 3), although there was no age-related difference in usage. A total of 73% of patients underwent needle biopsy, with a 19% increase from the earliest part of the observation period to the most recent (66% in 1992–2001 vs. 79% in 2007–2010; p < 0.001). Biopsy was more likely to have been used in the young adult age group (75%) versus those ≤19 years (61%).
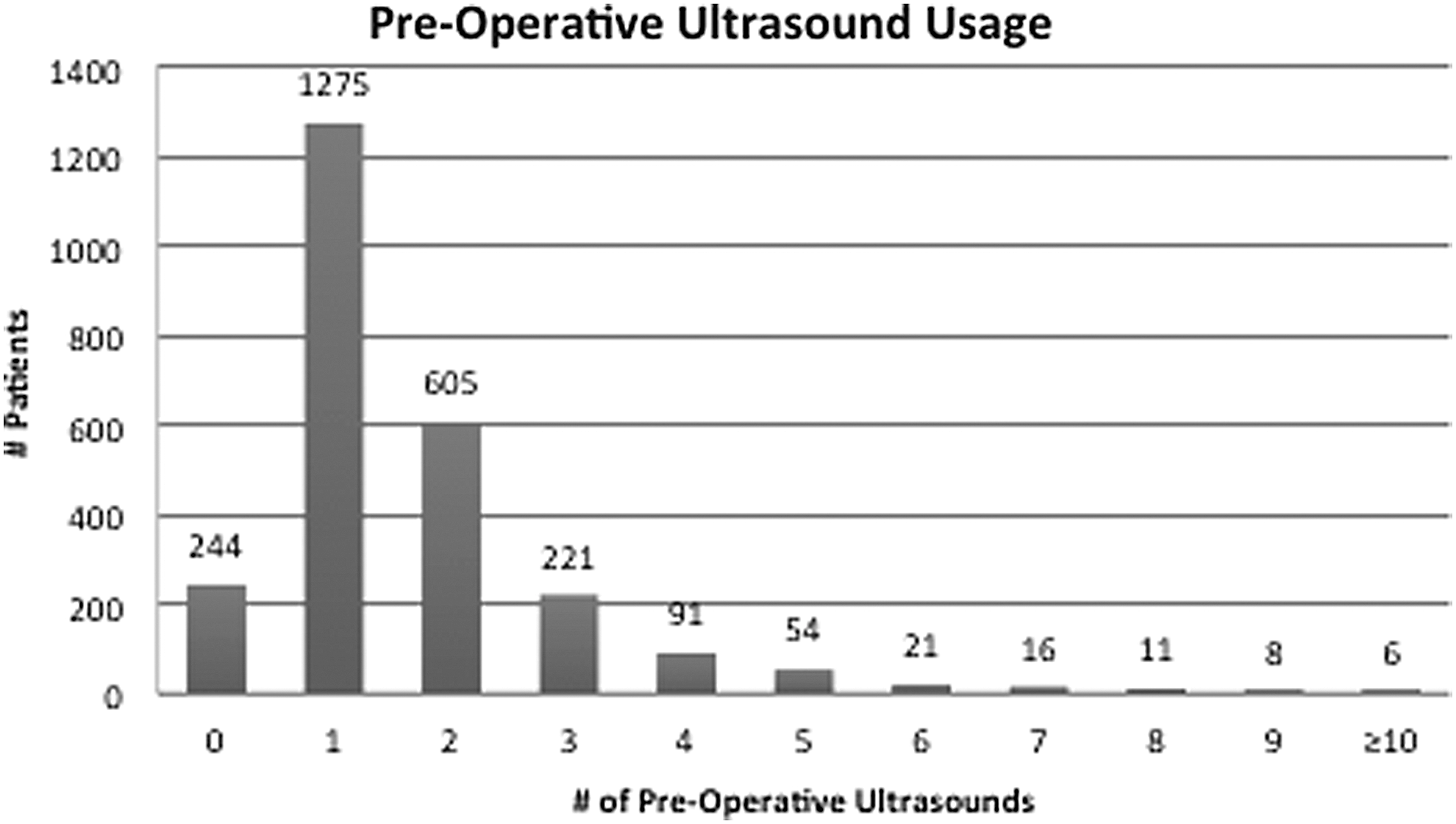
Preoperative ultrasound usage.
Treatment modalities
Therapeutic approaches are summarized in Table 4. Primary total thyroidectomy was the most frequent surgery performed (62% overall) followed by staged surgery (22% overall). Staged surgery was increasingly used for patients aged ≤19 years during the observation period, rising from 18% to 26%, while it declined over this period in the young adult group. Total thyroidectomy was more commonly employed for patients with PTC, whereas those with FV-PTC or FTC were more likely to undergo hemithyroidectomy or multi-stage thyroidectomy (data not shown). Approximately 35% of patients underwent neck dissection, the rate of which remained stable over the observation period. Parathyroid re-implantation was more common in those in the group aged ≥20 years and rose over time, while its use in younger patients was less frequent (17.8%) and remained static over time.
For confidentiality reasons some cells have been suppressed due to small cell sizes as indicated by —.
p-Value computed using Cochran–Armitage trend test or chi-square test where appropriate.
There were no surgical procedures billed during the study period for these patients.
The use of ablative radioiodine therapy has remained stable during the observation period (p = 0.10), with approximately 56% of subjects undergoing therapeutic RAI. Usage of RAI in children and adolescents rose significantly over the duration of this observation period, whereas usage in young adults did not change.
Discussion
This study establishes a foundation of diagnostic and practice patterns over a 19-year period. Of note, this study encompasses an era that preceded clinical practice guidelines for pediatric patients and for which adult guidelines did not appear until 2006, near the end of the study period (28). Thus, variations in practice patterns are to be expected.
The epidemiology is described of incident thyroid cancer among children and AYAs aged 0–29 years, and an account is provided of the diagnostic and treatment modalities over nearly two decades from 1992 to 2010 in Ontario, derived from comprehensive, population-based data sets.
The incidence of thyroid cancer in this pediatric and AYA population increased twofold over the 19 years of observation, with females developing thyroid cancer at a rate four to five times higher than that in males. The overall incidence and sex ratio is very similar to that reported in other geographic regions for similar age groups (3,29,30). The stability of the rate ratio when comparing the ASIR over time indicates that the increasing incidence is not driven by sex-specific differences.
As noted in multiple studies, there is a pronounced sexual dimorphism in incidence rates above the age of 12 years, the approximate median age of menarche. The mechanism of this divergence is unclear, although estrogenic influences as well as an excess of autoimmunity (to which malignancy risk has been associated) remain possible influences.
There was a small but significant rate of thyroid carcinoma as a second primary malignancy. This is consistent with recent data that identified thyroid carcinoma as the second most common second primary malignancy in children diagnosed with cancer prior to 15 years of age (31). Exposure to ionizing radiation is a recognized risk factor for PTC, and thus it is not surprising that primarily malignancies that typically include radiotherapy as a component of treatment constituted the majority of this population, although individual patients' radiation exposure prior to a thyroid cancer diagnosis was not specifically captured in this data set. The median latency to secondary thyroid malignancy was 11.2 years, which is also consistent with radiation-induced malignancy (32).
While it was not unexpected that almost all patients underwent preoperative ultrasound, it was somewhat surprising to find that 207 individuals (9% of the cohort) underwent four or more ultrasounds prior to initial surgery. While the nature of the current study (with data derived from administrative databases rather than individual case reports) precludes exploration of the rationale for multiple preoperative ultrasounds, this does highlight an area deserving further investigation in order to identify opportunities to optimize resource utilization specifically aimed at reducing unnecessary diagnostic studies prior to establishment of a definitive diagnosis.
Over the duration of this study period, there was a trend toward decreasing use of preoperative thyroid scintigraphy (which is rarely indicated for assessment of a thyroid nodule in the context of malignancy). The persistent utilization of preoperative thyroid scintigraphy (30% during the most recent time period), however, highlights another opportunity to reduce unnecessary healthcare expenditures by educating practitioners regarding appropriate evaluation of thyroid nodules and/or by regionalization of care to centers of excellence where current guidelines may be more likely to be adopted. A recent report demonstrated higher inappropriate use of therapeutic RAI in regions with more limited access to healthcare (33). It would be reasonable to speculate that similar findings may apply to inappropriate use of preoperative diagnostic RAI in regions with more limited expertise, although such data do not currently exist.
In parallel to the decreasing use of scintigraphy, a rising utilization of preoperative needle biopsy was noted—a modality that has been associated with a reduction in “unnecessary” surgery for benign nodules (34) and that can direct selection of the most appropriate surgical procedure. Nevertheless, a substantial proportion of patients underwent thyroid surgery with no prior biopsy, and this proportion was greater in the pediatric (<19 years) age group than in the young adults (38.3% vs. 24.1%), even in the most recent era (28.2% vs. 19.6%). This distinction may originate in prior surgical dogma, which advocated surgery as a primary diagnostic modality in children, given a substantially higher rate of malignancy among pediatric nodules when compared to adults. Nonetheless, the utility and test characteristics of fine-needle aspiration cytology in pediatrics has been validated and is well established (35 –37), and it is considered the standard of care in children with thyroid nodules (6). Identification of the rationale for avoiding biopsy prior to surgery and efforts to encourage this practice more widely represent an additional opportunity for optimization of resource utilization in this population.
Review of treatment modalities confirms that the majority of individuals underwent primary total thyroidectomy, with RAI ablative therapy in 55% of patients. There was no difference in primary surgical approach between the pediatric (≤19 years) and young adult (≥20 years) groups, although staged procedures were more common in the younger group in more recent years. Access to data distinguishing central versus lateral neck dissection was not available. Parathyroid re-implantation increased over time in the young adult group alone.
The overall rate of RAI usage was stable during this study period. The proportion of younger patients (i.e., those <20 years of age) receiving therapeutic RAI did increase significantly over the study period. While a recent study demonstrated a rise in RAI from 4% in 1973 to 62.8% in 2008, it is unclear whether there was a significant increase in usage during the latter part of this analysis, corresponding to the current study (1992–2010) (38). In the context of the 2015 ATA pediatric guidelines, directing more limited utilization of RAI therapy, a decline in these numbers over the next 5–10 years is anticipated.
Surgical complication rates are higher in pediatric patients compared to adults. Cervical surgical volumes are also inversely correlated with complication rates, although access for pediatric patients to high-volume endocrine or head and neck surgeons may be limiting, particularly outside of large metropolitan areas (39). This raises the question of regionalization of care for young patients with thyroid carcinoma, an issue that is not addressed in this study but one that must be explored in the context of these data in future analyses.
The strengths of this study include complete data regarding children and AYAs within a provincial population based on a single-payer system with consolidated administrative databases derived from legislated collection of clinical data.
The analysis is limited by a lack of data on disease extent and the basis for management decisions for individual patients. This is inherent to the use of retrospective administrative data. Cell-size restrictions, established to protect anonymity of patients with rare diagnoses, preclude extensive characterization of certain populations, including those with thyroid cancer diagnosed prior to the age of 12 years and those who died following a diagnosis of thyroid malignancy. Moreover, diagnostic and treatment details, including nodal burden, tumor size, stage, surgical complication rates, and dose of RAI, are not captured in these data sets, nor are other clinical variables such as family history, genetic predisposition or environmental (non-therapeutic) exposures. Finally, as these data do not include patient-level information, it is not possible to comment on surgical or RAI-related complication rates or the relationship to patient volumes.
Better integration of patient-level variables, including tumor extent, treatment complication rates, and outcomes tied to these administrative data, would inform decision making related to optimal treatment approaches and relationships between volumes and outcome.
This study has characterized the landscape of thyroid carcinoma in children and AYAs over a 19-year period using a true population-based data set, including diagnostic and therapeutic resource utilization patterns. Opportunities for healthcare cost reduction are highlighted, including limiting the usage of preoperative thyroid scintigraphy and the number of ultrasound studies performed prior to a definitive diagnosis and potentially reducing unnecessary surgery by encouraging more widespread utilization of fine-needle biopsy. These data are relevant to policy makers and healthcare administrators to assist in resource allocation and quality benchmarking. Future work should include exploration of geographic distribution related to access and volume, as well as investigation of the health service utilization patterns of these patients during the survivorship period.
Footnotes
Acknowledgments
J.D.P. and J.D.W. received funding from the Pediatric Oncology Group of Ontario (POGO). This study was also supported through funding support to ICES from an annual grant by the Ministry of Health and Long-Term Care (MOHLTC) and the Ontario Institute for Cancer Research (OICR) and through provision of data by the Institute for Clinical Evaluative Sciences (ICES) and Cancer Care Ontario (CCO). The opinions, results, and conclusions reported in this paper are those of the authors. No endorsement by ICES, CCO, OICR, or the Government of Ontario is intended or should be inferred.
Author Disclosure Statement
The authors have declared no conflicts of interest.