
Abstract
Background:
Several studies have reported inconsistent findings on the advantages and disadvantages of long-term treatment with antithyroid drugs (ATD). A systematic review and meta-analysis was undertaken to clarify the numerous aspects of long-term treatment with ATD.
Methods:
Medline and the Cochrane Library for trials published between 1950 and May 2016 were systematically searched. Studies containing data for long-term (>24 months) ATD treatment were included. Summary estimates of pooled prevalence, odds ratio, and weighted mean difference were calculated with a random effects model.
Results:
Of 587 related articles found, six fulfilled the inclusion criteria. Long-term ATD treatment induced a remission rate of 57% [confidence interval (CI) 45–68%], a rate that was higher in adults than in non-adults (61% vs. 53%). The rate of complications was 19.1% [CI 9.6–30.9%], of which only 1.5% were major complications. The annual remission rate for each year of treatment was 16% [CI 10–27%], which was higher in adults than non-adults (19% vs. 14%). However, it should be noted that this is not a true linear correlation, but a positive relationship can be suggested between time and remission rate. Meta-regression revealed that smoking had a significant lowering effect on remission rate.
Conclusions:
Long-term ATD treatment is effective and safe, especially in adults, indicating that it should be considered as an alternative treatment for Graves' disease.
Introduction
G
There are three treatment modalities for GD: antithyroid drugs (ATD), radioactive iodine (RAI), and surgery (8). In the United States, RAI is the therapy mostly preferred by physicians, although there has been an increasing trend in recent years to use ATD and reduce the use of RAI (9). In Europe, Latin America, and Asia, there is higher physician preference for ATD (10 –15) in order to avoid ablation and to assist some patients to enter prolonged remission.
The major clinical drawback of treatment with ATD is the high rate of relapse of hyperthyroidism when therapy is discontinued (16). Because of this risk of recurrence, RAI treatment or thyroid surgery is often recommended. Nevertheless, the convenience of ATD treatment and the fact that it does not irreversibly compromise the thyroid has made long-term low-dose ATD treatment a rational alternative for control of GD (17). The 2016 American Thyroid Association (ATA) guidelines recommend that “if a patient with GD becomes hyperthyroid after completing a course of MMI [methimazole], consideration should be given to treatment with RAI or thyroidectomy. Continued low-dose MMI treatment for longer than 12–18 months may be considered in patients not in remission, who prefer this approach” (9).
The present study aimed to synthesize data available to clarify the advantages and disadvantages of long-term treatment with ATD.
Methods
A systematic review of the published work according to the PRISMA statement for the conduct of meta-analyses (18) was performed to estimate the rates of remission and complications in long-term treatment with ATD.
Eligibility criteria
All original studies containing data for long-term ATD treatment (>24 months of treatment in all patients included) were eligible for inclusion. Exclusion criteria were irrelevant articles (based on screening of titles and abstracts), insufficient data available in the article, duplications of articles, no original data (review articles), and articles containing continuous ATD treatment. All included studies were planned for long-term treatment duration. All patients who withdrew from ATD treatment due to side-effects or poor compliance were excluded.
Study identification
Relevant studies were identified by searching Medline (from 1950 to May 2016) and the Cochrane Library database (no date restriction) using the search terms of “Graves' disease and antithyroid drugs,” “Graves' disease and long-term therapy,” “Graves' disease and continuous therapy,” “long-term antithyroid drugs,” “long-term methimazole therapy,” “long-term carbimazole therapy,” “long-term propylthiouracil therapy,” “continuous antithyroid therapy,” “continuous methimazole therapy,” “continuous carbimazole therapy,” and “continuous propylthiouracil therapy.” The search was done without language restriction. Reference lists from identified articles were manually scanned to identify any other relevant studies.
All articles were reviewed independently by two reviewers (R.M. and F.A.), and any disagreement was resolved by consensus. After abstract screening and retrieval of potentially eligible studies, the full-text articles were assessed for eligibility. Duplicate studies were excluded. Prior to review, the reviewers were blinded to names of journals and authors.
Data collection and management
Two reviewers (R.M. and F.A.) independently extracted data from included trials, and any disagreement was adjudicated by consensus. Published reports were obtained for every study, and standard information was extracted into a spreadsheet. The data sought included time and location of study, age and sex of individuals, number of study subjects, modality of treatment, duration of ATD treatment, remission rate, complications (major, minor), baseline data (goiter, smoking, thyroid peroxidase antibody [TPOAb], thyroglobulin antibody [TgAb], TRAb, and TSH-binding inhibitor immunoglobulin [TBII]), data at time of drug withdrawal (goiter, smoking, bone mineral density [BMD], TPOAb, TGAb, TRAb, TBII, lipid profiles and cardiac echo parameters).
The present study defined “long-term treatment” as >24 months of treatment with ATD, and “short-term treatment” as ATD treatment duration of ≤24 months. A patient was considered to be in remission if she/he had a normal serum TSH, free thyroxine (fT4), and total triiodothyronine (T3) for one year after discontinuation of ATD therapy. The defined cut point of age for adults was set at 18 years. Each group was divided into subgroups of adults and non-adults (<18 years old), if data were available.
Risk of bias assessment
Two reviewers (R.M. and F.A.) independently assessed methodological quality of the included trials using the Newcastle–Ottawa Quality Assessment Scale (19), and any disagreement was resolved by consensus. This tool appraises the selection of the study groups, the comparability of the groups, and the ascertainment of exposure or outcome. Potential publication bias was assessed with funnel plots of the Arcsin prevalence versus its standard error (20).
Meta-analysis
Individual prevalence, odds ratio (OR), and weighted mean difference (WMD) for the defined groups were calculated from the data extracted from each manuscript before data pooling. Summary estimates of pooled prevalence, OR, and WMD were calculated with a random-effects model. Inconsistency was assessed using the I 2 statistic, with values <25% indicative of low and >75% indicative of high inconsistency, not due to chance (21). Agreement between reviewers was estimated with Cohen's test (22). A two-sided p-value of <0.05 was regarded as significant for all analyses. Statistical analyses were done with Meta XL v3.0, and meta-regression was done with R v3.2.3.
Subgroup and sensitivity analyses and meta-regression
Subgroup analyses were done based on the adult status (adult/non-adult) of the study population, if data were available. The defined cut point of age for adults was set at 18 years. Meta-regression was done for assessment of contributing factors on remission rate. Sensitivity analyses were also conducted, excluding one study at a time in order to evaluate whether any specific study significantly influenced the overall pooled results.
Results
Study selection and characteristics
The literature search yielded 587 articles, of which 145 were reviewed in full text (Fig. 1). Of the six articles that met the inclusion criteria, three had data for adults, and three articles had data for non-adults. Three of the articles only had data on long-term ATD treatment, one article compared long-term ATD with RAI, one article compared results of short-term versus long-term ATD, and one reported comparisons of long-term treatment with MMI versus propylthiouracil (PTU). All included studies employed titration regimens, except for one study by Elbers et al. (23) that used a block and replace strategy. Table 1 summarizes characteristics of the included studies.
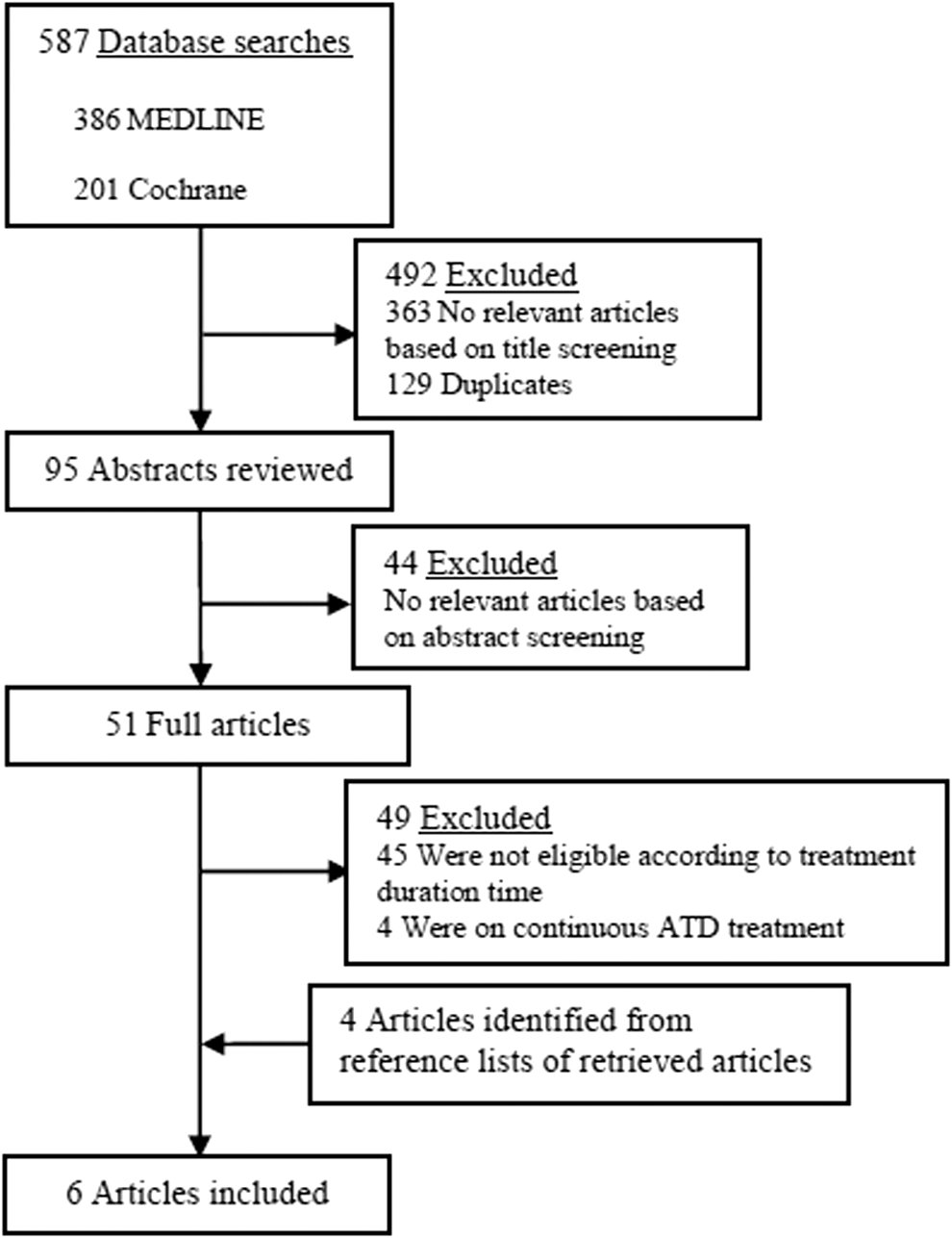
Flow chart for the systematic review and the meta-analysis.
AITD, antithyroid drugs; MMI, methimazole; PTU, propylthiouracil; RAI, radioiodine; NR, not reported.
Study quality
The risk of bias of included studies was low, mainly due to lack of blinding when assessing the outcomes (Table 2). Formal statistical testing with funnel plots showed no evidence of publication bias. Inter- reviewers agreement was “excellent” (Cohen's test κ = 0.98).
Lost to follow-up is known to introduce bias. However, it has been proposed that for values <20%, the amount of bias could be negligible (19).
RR, remission rate; TRAb, thyrotropin receptor antibody; TgAb, thyroglobulin antibody; TPOAb, thyroid peroxidase antibody.
Meta-analysis
Six articles (23 –28) had sufficient data for remission rates with long-term ATD treatment. Considering that one article (26) had two profiles comparing MMI versus PTU, there were seven data profiles from six articles. The pooled analyses in Figure 2 shows that long-term ATD treatment induced a remission rate of 57% ([confidence interval (CI) 45–68%]; I 2 = 85%). Subgroup analysis demonstrated that the remission rate in adults was higher than that of non-adults (61% vs. 53%). Long-term ATD treatment was associated with 19.1% complications ([CI 9.6–30.9%]; I 2 = 83%), of which only 1.5% were major complications.
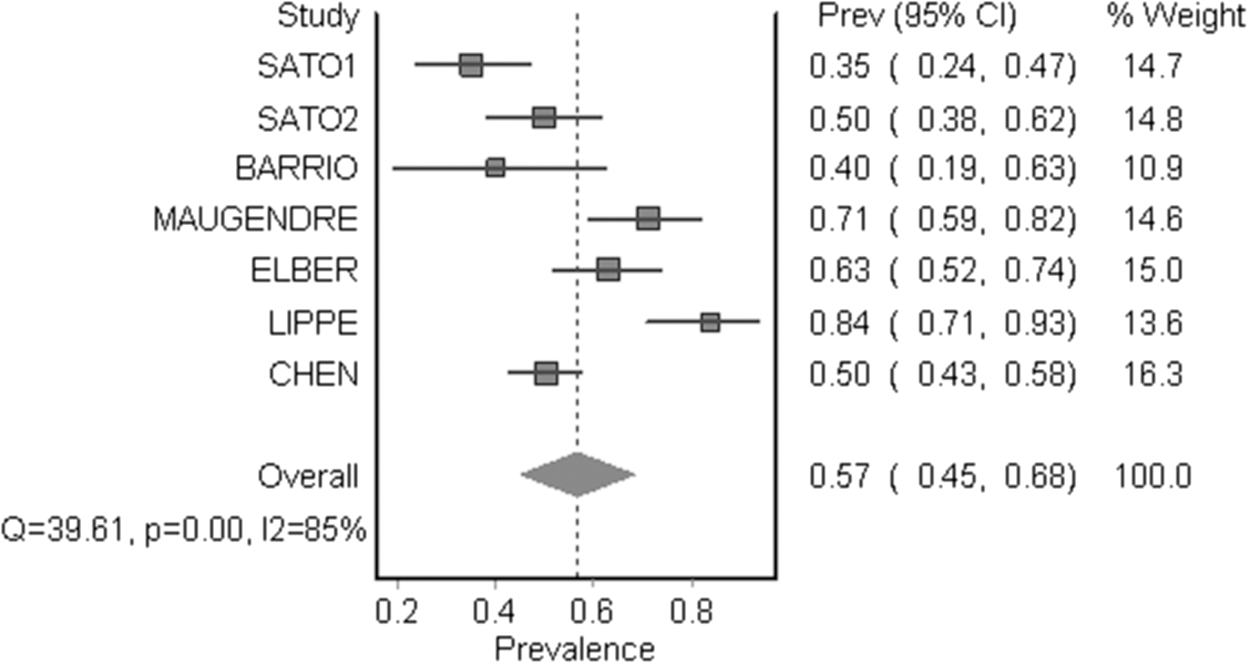
Forest plot of prevalence and confidence interval (CI) of pooled studies reporting remission rates for long-term antithyroid drug (ATD) treatment. SATO1, data for group of methimazole users; SATO2, data for group of propylthiouracil users.
Further analysis was done for the evaluation of the effect of “treatment duration” on remission rate. Remission rate for each year of treatment was 16% ([CI 10–27%]; I 2 = 94%; Fig. 3), a rate that was higher for adults than it was for non-adults (19% vs. 14%). Sensitivity analysis showed that after exclusion of an article by Chen et al. (28), the remission rate per year-treatment rose to 29% in adults.
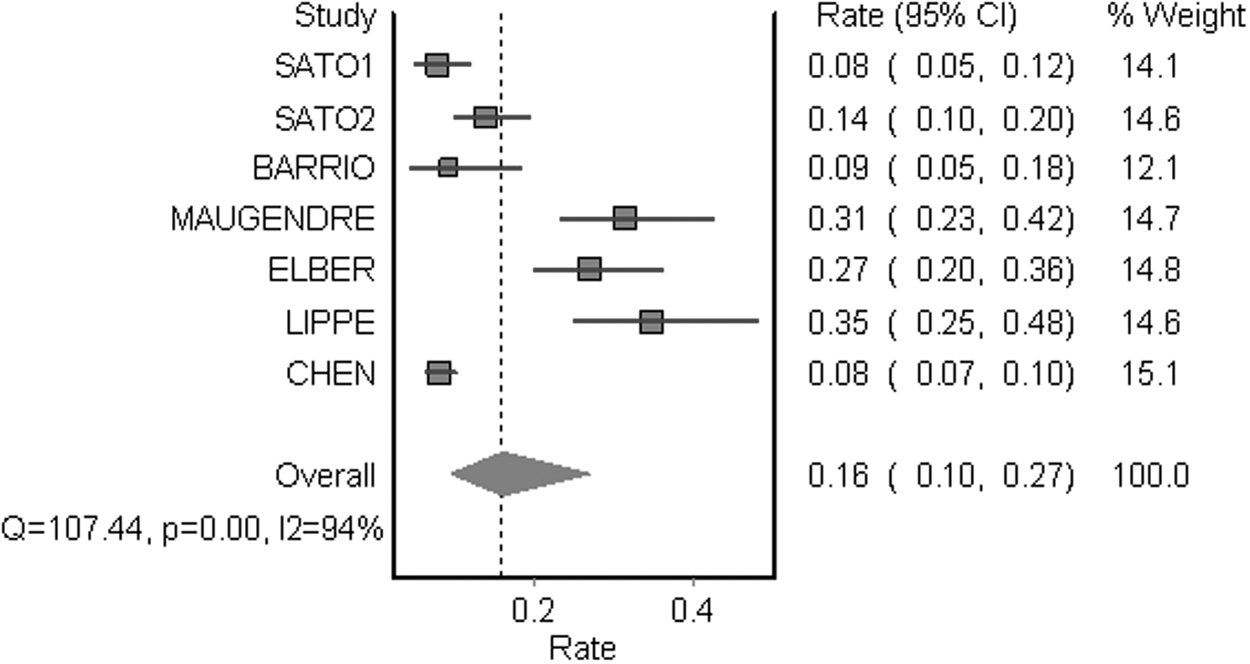
Forest plot of rate (remission per year treatment) and CI of pooled studies reporting remission rate for long-term ATD treatment.
Meta-regression
Meta-regression was done for assessment of contributing factors on remission rate. Meta-regression revealed that smoking had a significant lowering effect on remission rate. For other available covariates (goiter and TPOAb, TgAb, and TRAb positivity), meta-regression was not possible because of insufficient data.
Discussion
To the best of the authors' knowledge, this is the most comprehensive meta-analysis to date clarifying some aspects of long-term ATD treatment for GD. This study suggests that long-term ATD treatment is effective and safe.
Results of this study show that long-term ATD treatment induces a high remission rate, especially in adults, associated with low rates of complications. Meta-regression reveals that smoking has a significant lowering effect on remission rate.
Results of the analysis demonstrate a remission rate of 16% per year of treatment. However, it should be noted that the effect of “treatment duration” on remission rate is calculated based on small numbers of studies, and this is not a true linear correlation. However, a positive relationship between time and remission rate is suggested.
To the authors' knowledge, there is no similar systematic review or meta-analysis for comparison data in this field. However, there are some studies reporting outcomes of long-term ATD treatment, either per se or in comparison with other treatment modalities. Nevertheless, there are many articles (observational studies, randomized controlled trials, and narrative reviews) that attempt to validate the best treatment option for GD.
Therapy for GD involves complex decision making. There is no perfect recommended treatment for all patients, and any therapeutic option is associated with certain limitations and complications. There are three treatment modalities for GD: ATD, RAI, and surgery (8). ATD can restore euthyroidism, although the disease may recur after a course of ATD. In contrast, RAI treatment, as well as surgical thyroidectomy, leads to hypothyroidism in most cases. Other drawbacks of these modes of treatment include the potential the following uncommon events: surgical complications, radiation exposure, and the need for hospitalization in some countries (17). However, ATDs are not free from adverse effects. Minor complications such as a rash, gastric intolerance, and arthralgia are observed in up to 19% of patients, while major complications occur rarely (<0.5% of cases), and they can include agranulocytosis and hepatotoxicity, which can both be life-threatening (29,30).
Adverse effects usually occur during the first three to six months of treatment, and major adverse events tend to be associated with high ATD doses (17). In a retrospective cohort analysis from Japan (30), of >50,000 GD patients, 55 developed agranulocytosis, five of whom had pancytopenia, for an estimated cumulative incidence of 0.3% in 100 days, with a median interval to onset of 69 days. All 50 patients with agranulocytosis alone were successfully treated with granulocyte colony stimulating factor (G-CSF), steroids, or supportive care, but one of five patients with pancytopenia died. No predictive risk factors for the development of agranulocytosis could be identified. A second study from Japan (31) was based on a national database for adverse drug reactions, which may have included some patients reported earlier in the first study. A total of 754 GD patients who developed ATD-induced hematologic complications were reported, for an estimated incidence of 0.1–0.15%. At the onset of agranulocytosis, the average MMI dose was 25 mg/day, and the average PTU dose was 217 mg/day. The average age of patients developing agranulocytosis was slightly older (45 years vs. 40 years). Seventy-two percent developed agranulocytosis within 60 days of starting ATD, and 85% within 90 days. Thirty (4%) of the events were fatal. A recent pharmacoepidemiologic study from Taiwan (32) demonstrated that hepatotoxicity incidence rates peaked within 30 days of continuous treatment and tended to decline afterward. The rates were higher in older patients (aged >65 years) and with higher doses (MMI ≥10 mg/day; PTU ≥100 mg/day). Similar findings were also recently reported from China (33). The average doses of ATDs at the onset of hepatotoxicity were around 19 and 212 mg/day for MMI and PTU, respectively, indicating severe hepatotoxicity tended to occur within the first three months after the onset of ATD therapy.
In all women with GD who are of childbearing age, the prospect of future pregnancy should be considered. Women with GD desiring a future pregnancy should be advised regarding the complexity of disease management during future gestation, including the association of birth defects with ATD use. Preconception counseling should assess the risks and benefits of all treatment modalities, along with the patient's desired timeline for conception (34).
In spite of >70 years of experience with the use of ATD and RAI for the treatment of GD, the rationale for choice of therapy is often obscure (35,36). Very often, the choice has to be made between prolonged treatment with ATD, on the one hand, and lifetime therapy with thyroid hormones for thyroid failure on the other (37). In the United States, RAI has been the preferred therapy, although in recent years, there is a trend suggesting an increased use of ATD and a reduction of RAI as primary treatment (9). A 2011 survey of clinical endocrinologists showed that 59.7% of respondents from the United States selected RAI as primary therapy for uncomplicated cases of GD compared to 69% in a similar survey performed 20 years earlier (11). A recent study by Brito et al. revealed that the most common “initial” treatment for GD in commercially insured patients in the United States today is ATD. The increased use of ATD started in 2005 at the expense of RAI use. ATD was the most commonly used treatment in this cohort (58%), followed by RAI (35%) and surgery (6%). Compared to patients who received RAI, ATD patients were more likely to be younger, to have fewer comorbidities, and to be pregnant. Patients undergoing surgery were less likely to be male and to be Hispanic, and more likely to have a higher degree of comorbidities and to receive care in the Northeast and South U.S. regions (8). In Europe, Latin America, and Asia, there is higher physician preference for ATD (10 –15) in order to avoid ablation and to induce prolonged remission in some patients.
Several large cohort studies have reported increased mortality from vascular causes in RAI-treated patients (38,39). However, recently, Boelaert et al. reported an increase in cardiovascular and cerebrovascular deaths after RAI therapy not resulting in hypothyroidism as opposed to unchanged mortality in RAI-treated patients on levothyroxine therapy, reflecting the role of persistent hyperthyroidism as opposed to that of RAI therapy in mortality (40). In addition, there may be an increased cancer incidence and mortality in RAI-treated hyperthyroid patients (41). However, a recent meta-analysis found no increase in the overall cancer risk after RAI treatment for hyperthyroidism, although a trend toward increased risk of thyroid, stomach, and kidney cancers was seen (42).
ATD have been employed in the treatment of thyrotoxicosis for more than seven decades (43). Although these medications do not cure Graves' hyperthyroidism, they are very effective in controlling the condition when given in adequate doses. When they fail to achieve euthyroidism, the usual cause is nonadherence (44). A patient is considered to be in remission if she/he is found to have a normal serum TSH, fT4, and total T3 for one year after discontinuation of ATD therapy (9). The frequency of prolonged remission among patients treated with a thionamide for one to two years varies from 20% to 60%, with lower rates of remission occurring in children and adolescents (45). The remission rate varies considerably between geographical areas (9). In earlier studies from the United States, about 20–30% of patients were reported to have a lasting remission after 12–18 months of medication (46). More recent data are not available (9). The remission rate may be higher in Europe and Japan. A long-term European study indicated a 50–60% remission rate after five to six years of treatment (3), and a study from Japan reported a 68% remission rate after two years of treatment (47). A lower remission rate has been reported in men, smokers (men in particular), and those with large goiters (≥80 g) (48 –52). A meta-analysis suggested that the remission rate in adults is not improved by a course of ATDs of >18 months (53), although the authors pre-specified a minimum duration for drug treatment of six months, and this conclusion was based only on data from two of the included studies (27,54). A study conducted in Spain showed no difference in remission rates between 12- and 24-month ATD treatment and no prognostic role for TRAb (54). A meta-analysis by Feldt-Rasmussen et al. suggested that TRAb is not sufficiently predictive of relapse after ATD treatment in adults (55), whereas most recent studies have clearly demonstrated that TRAb levels at the onset and end of ATD treatment are of prognostic value (50,56 –61).
The major clinical drawback of treatment with ATD is the 20–70% relapse of hyperthyroidism when therapy is discontinued (16,62). However, treatment with ATD might have a beneficial immunosuppressive role, either, primarily, by decreasing thyroid-specific autoimmunity or, secondarily, by ameliorating the hyperthyroid state, which may restore the dysregulated immune system to normal (63). It is still a matter of debate whether this effect is due to an immunosuppressive effect of the drug itself, as suggested by some studies (64,65), or to a reduced production of thyroid antigens, which is followed by a reduced immune response (66). Considering all these possible mechanisms highlights the importance of maintaining the patients in a euthyroid state for a long period to minimize autoimmune aberration and GD recurrence (63,67). This may occasionally require more prolonged use of MMI, of which the lowest possible dose should be used to minimize the risk of side effects (63). Long-term treatment has been proposed by some authors (68,69), especially in children (25,70,71) and patients with Graves' orbitopathy (GO) (23,72).
Some studies have shown that long-term MMI is a reasonable alternative approach in selected patients (i.e., in younger patients with mild stable disease on a low dose of MMI) (68,69). Another study by Azizi et al. reported that continuous administration of MMI is safe, without major complications, and accompanied by fewer events of subclinical hypothyroidism and dyslipidemia in comparison to patients on levothyroxine substitution for RAI-induced hypothyroidism. In addition, parameters such echocardiography findings, BMD, and neuropsychology tests favor MMI treatment over RAI (73). A recent retrospective analysis compared long-term outcomes of patients who had relapsed after a course of ATD, treated with either RAI and levothyroxine or long-term ATD therapy (74). Patients treated with RAI more often had persistent thyroid eye disease, continuing thyroid dysfunction, and experienced more weight gain compared to those patients receiving long-term ATD treatment. Orgiazzi (17) concluded that the use of low doses of MMI is efficient and safe and offers better outcomes for GO than RAI treatment, and proposed that prolonged use of low doses of MMI may be an alternative for patients whose GD has relapsed, particularly for patients with GO or for patients who refuse a definitive treatment.
If a patient with GD becomes hyperthyroid after completing a course of MMI, the 2016 ATA guidelines recommend that “consideration should be given to treatment with RAI or thyroidectomy. Continued low-dose MMI treatment for longer than 12–18 months may be considered in patients not in remission who prefer this approach.” Howard (75) emphasized in 1967 that his approach to the therapy of thyrotoxicosis is to control the disease, for a lifetime if need be, with a drug such as PTU until spontaneous remission occurs. It has been repeatedly noted that thyrotoxicosis may be a self-limited disease, and treatment with ATD is often used for limited time durations only (75 –77). Slingerland et al. (78) declared: “A controllable, self-limited disease seems best treated with a controllable and limitable therapy.”
Despite the limitations of this study, which is based on published data and thus limits the capacity to explore factors associated with remission rates fully other than smoking (e.g., goiter size, sex, age, HLA and auto antibodies [TRAb, TgAb, TPOAb, and TBII]), this meta-analysis benefits from a comprehensive search strategy, no limitations for time and language in the search strategy, independent reviews by two reviewers, and no publication bias.
Conclusion
Long-term ATD treatment is effective and safe, especially in adults, indicating that it should be considered as an alternative treatment for GD.
Footnotes
Acknowledgments
We would like to thank Ms. Sara Jambarsang (PhD in biostatistics) for conducting these analyses. The authors wish to acknowledge Ms. Niloofar Shiva for critical editing of English grammar and syntax of the manuscript. We would like to express our appreciation to Ms. Tahereh Fakhimi Ata for typing of the manuscript.
Author Disclosure Statement
There authors have nothing to disclose.