
Abstract
Background:
Well-differentiated thyroid cancer (WDTC) is the most common endocrine neoplasia, and its incidence is rising. Studies have reported an increased risk of second primary cancer (SPC) in WDTC survivors, but its relationship with radioiodine treatment (RAIT) and other risk factors remains controversial. This study evaluated whether RAIT is an independent risk factor for SPC in WDTC patients.
Methods:
This was a retrospective single-center study. A total of 2031 patients with WDTC diagnosed between 1998 and 2009, treated and followed at the authors' tertiary cancer center, were included.
Results:
The median age of patients was 48 years (range 5–90 years); 83% were women and 77% underwent RAIT. The median follow-up was 8.8 years (range 5.0–17.0 years). A total of 130 SPC were diagnosed: 108/1570 (6.9%) received RAIT (RAIT+) and 22/461 (4.8%) did not (RAIT–). The most common SPC was breast cancer (31%), followed by genitourinary and gastrointestinal cancer (18% each). The 10-year cumulative incidence of SPC was 8.2% in RAIT+ and 4.5% in RAIT–. The absolute risk increase in the RAIT+ group versus the RAIT– group at 10 years of follow-up was 0.039 [confidence interval (CI) 0.011–0.067] per patient-year. The number needed to harm (NNH) was 25.6 [CI 15.0–87.2], indicating that on average during a 10-year follow-up period, there is one additional case of SPC for every 26 patients receiving RAIT. When controlling for age, sex, and familial and personal histories of cancer, there was an 84% increase in the risk of SPC in the RAIT+ group compared to the RAIT– group (p = 0.026; relative risk = 1.84 [CI 1.02–3.31]). There was an association between SPC incidence and total cumulative activity administered, which was statistically significant >200 mCi. The incidence of SPC was higher in both the WDCT and the RAIT+ cohorts compared to the general population (standardized incidence ratios = 1.32 and 1.40, respectively).
Conclusion:
These results indicate that in spite of the low incidence of SPC in WDTC patients, the risk is increased after RAIT, particularly for activities >200 mCi. Thus, considering the excellent survival of patients with WDTC, clinicians need to weigh the risks and benefits of RAIT, especially in patients with low-risk thyroid cancer.
Introduction
W
The current approach for WDTC is surgery, followed by radioiodine treatment (RAIT) and suppressive therapy with levothyroxine oriented by histological features and risk assessment (5).
RAI has been used in the treatment of thyroid cancer since 1940 (6). It targets thyroid tissue, ablating any normal thyroid remnant in order to reduce the risk of recurrence and facilitating further surveillance by serum thyroglobulin (Tg) measurement. Furthermore, it is useful for re-staging with whole-body scintigraphy and for treatment of locoregional as well as metastatic disease. Usually, about 80% of the administered RAI activity will be excreted within 48 hours and will completely disappear (due to organic excretion and physical decay) about 10 days after administration. RAI is mainly eliminated by the urinary tract, about 10% by the digestive tract, and in lower amounts by the salivary glands, thus potentially exposing these tissues to ionizing radiation (7). Two types of biological effects of ionizing radiation are known: deterministic effects and stochastic effects. Deterministic effects are caused by the decrease or loss of organ function due to cell damage or cell death (i.e., nausea, leukopenia, anemia, infertility, and cataracts). There is a threshold dose and a linear relation with total administered activity. If the radiation exposure is reduced or discontinued, these effects are usually reversible. Stochastic effects result from radiation-induced changes in cells that retain their ability to divide (they may cause leukemia and solid cancers). There is no threshold dose, they are not reversible, and, ultimately, they can be responsible for genetic mutations. To minimize this risk, administered activity and radiation exposure should be “as low as reasonably achievable” (8). The peak incidence for radio-induced hematological cancers is 5–9 years and for solid cancers is at least 10–15 years after radiation exposure (9). There are well-described adverse effects of RAIT, most of which are time limited (e.g., cervical edema, sialadenitis, infertility, etc.), but late effects do occur in a subset of patients (10).
Some studies have shown an increased risk of second primary cancer (SPC) in WDTC survivors compared to the general population (11 –13). Although RAIT may play a role in the induction of some of these SPC, the high incidence of tumors preceding WDTC may suggest etiologic similarities (14). Nevertheless, studies found conflicting data: some series showed that the risk of SPC is related to RAIT (15,16), while other authors suggest a non RAIT-related risk (14,17,18). Therefore, this subject is still under debate.
The main aim of this study was to compare the incidence of SPC in patients with WDTC exposed to RAIT (RAIT+) with those not exposed to RAIT (RAIT–). The secondary aims were to evaluate the relationship between the 131I cumulative activity administered and risk of SPC and to compare the incidence of SPC in WDCT survivors (also evaluating the subgroups exposed and not exposed to RAIT) to the general population.
Materials and Methods
Patients
A single-center cohort study was conducted with retrospective data collection. All consecutive patients diagnosed with WDTC (ICD-10-CM C73) (19) between 1998 and 2009 at the authors' tertiary cancer center were identified from the South Regional Cancer Registry database. This population-based registry incorporates all the health institutions from the south of mainland Portugal and Madeira Islands, altogether comprising about 4,500,000 inhabitants. Inclusion criteria were surgically resectable WDTC and a minimum follow-up of five years after diagnosis. Patients with inoperable WDTC at the time of diagnosis were excluded. Cases with a documented history of radiotherapy or radiation exposure before the diagnosis of WDTC were also excluded. The study protocol was approved by the Ethics Committee at the authors' institution.
Patient management and follow-up protocols
At the authors' institution, the main criteria for RAIT are: age >45 years, tumors >4 cm, multifocal tumors, extrathyroidal extension, vascular invasion, aggressive variants of WDTC, lymph node and distant metastases, and incomplete resection (R1/R2). The initial activity of RAI administered ranges from 50 to 100 mCi, depending on the risk stratification. Patients with evidence of metastatic disease or high-risk patients with moderate to intense 131I neck uptake in the whole-body scintigraphy performed 48 hours after first RAIT receive subsequent 131I treatments in case serum Tg remains detectable. In addition, some patients with biochemical evidence of disease, even without significant iodine-131 uptake, are also submitted to subsequent RAIT.
Follow-up procedures comprise serum free thyroxine (fT4), thyrotropin (TSH), Tg, and Tg antibodies (TgAb) two to three months after first RAIT. Patients without metastatic disease undergo neck ultrasound and serum fT4, TSH, Tg, and TgAb determination six to nine months after first RAIT. In patients without evidence of disease (undetectable Tg and TgAb in association with negative neck ultrasound), subsequent follow-up procedures include serum fT4, TSH, Tg, and TgAb assays every year and a neck ultrasound every three years. Patients with evidence of disease are followed up according to individual patient characteristics.
Outcomes and variables analyzed
The primary outcome was time to diagnose a SPC. This was calculated from the date of first RAI administration to the date of diagnosis of SPC. In patients not treated with RAI, the time to SPC was calculated from an index date, which took into account the median time between initial surgery and first RAI administration observed in the group of patients treated with RAI (in practice, this was calculated as the date of initial surgery plus five months). SPC was defined as any non-thyroidal primary malignancy with histological diagnosis >12 months after the first RAI administration/index date. Any second malignancy diagnosed within one year was considered synchronous and accounted for personal history of cancer, together with any prior malignancies. For patients who developed more than one SPC, the date of the earliest occurring malignancy was considered. Data on occurrence of SPC and follow-up survival data were retrieved from the Regional Cancer Registry database. The cutoff date for follow-up was January 2014.
Information on patient demographics (sex and age at the time of WDTC diagnosis), WDTC characteristics (stage and histology) and management (including date of first RAIT, total cumulative activity and number of RAIT administered), and familial and personal history of cancer was retrospectively collected from each patient's clinical notes.
Sample size
This study hypothesized that RAIT increases the risk of SPC in patients with WDTC. An a priori power calculation was performed considering the presence of competing risks and a threefold increase in the cause-specific hazard ratio of SPC (HR = 3) as the minimum effect size that we wished to detect at a significance level of 0.05 (two-sided). The competing event was defined as death without SPC and the event of interest as diagnosis of SPC (SPC and death due to other causes were considered as independent events). The a priori assumptions for the power calculation were: (i) about 400 new cases of operable WDTC could be eligible for inclusion per year over a period of five years (from 2000 to 2004), giving a planned total sample size around 2000 patients; (ii) minimum follow-up of 10 years; (iii) 10-year Kaplan–Meier estimates for the event of interest and for the competing risks are 97.5% and 90%, respectively; (iv) around 25% of the patients not treated with RAI. Based on these assumptions, the calculated power in the presence of competing risks was 73% increasing to >75% if no competing risks were considered. However, when patient clinical files were revised for eligibility assessment, it was verified that the accrual rate had been overestimated. For this reason, the accrual period was extended from 5 to 11 years (from 1998 to 2009) and the minimum follow-up shortened from 10 to 5 years. These changes resulted in a 7% decrease in the statistical power of the study. All consecutive eligible cases identified in this accrual period were included.
Statistical analysis
The cumulative incidence of SPC was calculated for the groups with and without RAIT using competing risk analysis, taking death not SPC related as a competitive event. The absolute risk increase (ARI) of SPC 10 years after RAIT/index date in RAIT+ compared to RAIT– patients was calculated based on the 10-year Kaplan–Meier survival estimate of time to SPC. ARI was then used to calculate the number needed to harm (NNH) (NNH = 1/ARI) (20). Gray's test and log rank test were used for univariate group comparison analysis. In order to control for the potential confounding factors (age, sex, familial history of cancer, and personal history of cancer [previous or synchronous]), multivariable analysis was conducted using the regression model proposed by Fine and Gray for competing risk analysis and the standard Cox proportional hazards model. Patients with missing values for the covariates were excluded from the multivariable analyses. In both models, proportional hazards assumption was checked by the Schoenfeld residuals.
An exploratory analysis by cumulative activity of RAI administered was also performed, considering the groups 0 mCi (no RAIT), 1–99 mCi, 100–199 mCi, 200–299 mCi, and ≥300 mCi. This categorization was chosen to reflect treatment with activities <100 mCi and one to three or more standard treatments of 100 mCi. A univariate analysis was conducted as a global comparison between the five groups followed by post hoc pairwise comparisons, with p-value adjustment using the Hochberg method. Multivariable exploratory analysis was conducted using the same methods and the same covariates as the main analysis.
In order to check the robustness of the comparative study between RAIT+ and RAIT– groups, several sensitivity analyses were conducted by increasing the latency period from index date to diagnosis of SPC to three and five years (instead of one year) and after excluding all breast cancer cases from the SPC group.
In a secondary analysis, the incidence of SPC in the global WDTC cohort and in both RAIT+ and RAIT- subgroups was compared with that of the general population by calculating the standardized incidence ratios (SIRs) for all sites/types of SPC (observed cases divided by expected cases) and the respective exact confidence intervals (21). The accumulated person-years at risk was calculated by compiling the person-years of observation according to the age groups ≤19 years, 20–49 years, and ≥50 years old, sex, and calendar-year period from the first RAI administration/index date to the date of SPC, date of death, or date of last follow-up, whichever occurred first. This was then multiplied by the cancer incidence rates specific for age groups ≤19 years, 20–49 years, and ≥50 years old, sex, and calendar-year intervals 2000–2004, 2005–2009, and 2010–2014 for the general population reported by the South Regional Cancer Registry to obtain the expected number of all SPC. All tests were two sided. A 5% significance level was considered. All statistical analyses were conducted using R software (22) and the packages “cmprsk” (23) and “survival” (24).
Results
Patient and RAIT characterization
Between 1998 and 2009, the authors' institution treated 2319 patients with thyroid cancer. A total of 288 patients were excluded: 40 subjects had previous cervical irradiation, 44 had anaplastic cancer, 97 had medullary cancer, 24 patients received adjuvant radiotherapy, and 83 were lost to follow-up. Therefore, 2031 patients diagnosed with WDTC were included. Patients and the tumor characteristics are presented in Table 1. The majority were women (83%), the median age was 48 years (range 5–90 years), and 2% (n = 36) were below 18 years old. The percentage of patients submitted to RAIT was 77% (n = 1570). The demographic and clinical characteristics were similar in both RAIT+ and RAIT– groups, particularly in terms of the sex distribution and the familial and personal history of cancer and histology (Table 1). As expected, the RAIT+ group presented a higher percentage of T4 tumors (21% vs. 4%). In this group, the median cumulative activity and median number of RAIT per patient were 118 mCi (range 50–1200 mCi) and 1 (range 1–8), respectively. In the RAIT+ group, the majority of patients received a total cumulative activity between 100 and 199 mCi (n = 1062; 68%), 14% (n = 227) received activities between 200 and 299 mCi, 10% (n = 155) received ≥300 mCi, and the remaining 8% (n = 130) received <100 mCi. The median and mean follow-up time from WDTC diagnosis in this cohort was 8.8 years and 9.1 years, respectively (range 5.0–17.0 years, standard deviation [SD] ±3.2), with a median follow-up time of 8.7 years (range 5.0–17.0 years) in the RAIT+ group and 10.0 years (range 5.0–16.0 years) in the RAIT– group. There were 128 deaths, 23% of which were related to WDTC.
Incidence of SPC
A total of 130 SPC were diagnosed in 129 patients, of which 108 (83%) were identified in the RAIT+ group and 22 (17%) in the RAIT– group (one patient submitted to RAIT had two SPC; Table 2). The most common SPC was breast cancer, corresponding to 31% of all SPC, followed by genitourinary and gastrointestinal malignancies, each representing 18%. Hematological SPC represented only 9% of cases. The median and mean latency periods for the diagnosis of SPC were 5.1 and 5.4 years (range 1.1–13.8 years; SD ±3.1) in the RAIT+ group and 6.2 and 6.4 years (range 1.0–12.3 years, SD ±3.3) in the RAIT– group, respectively. When analyzing the 107 patients treated with RAI who developed SPC, the median RAIT frequency and the median total activity administered were 1 (range 1–8) and 154 mCi (range 70–1072 mCi), respectively.
One patient treated with radioiodine had two second primary cancers: gut cancer and leukemia.
Other: two patients with unknown primary cancer, one patient with thymus cancer, and one patient with sarcoma.
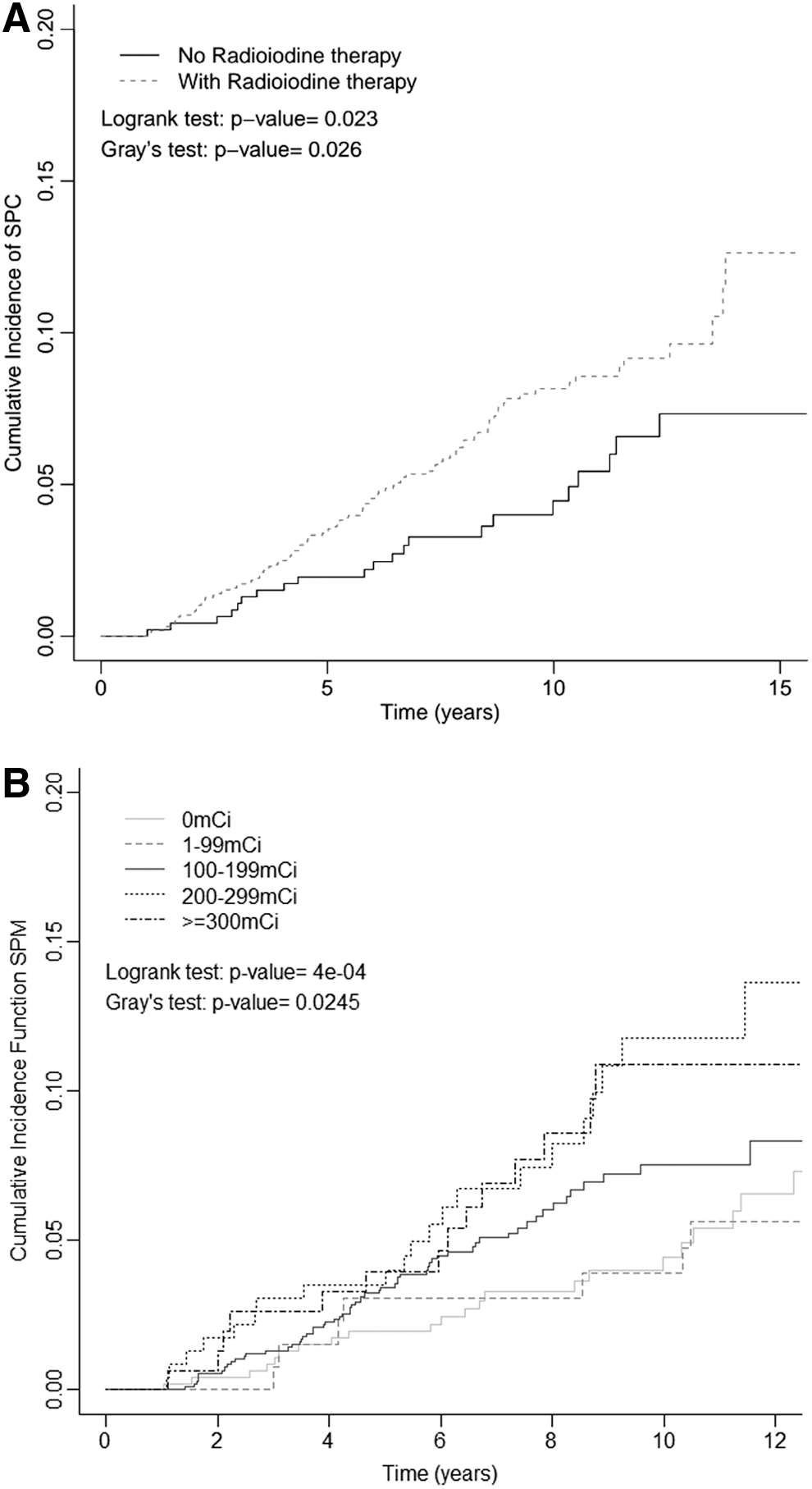
Figure 1A shows the cumulative incidence functions of SPC in the RAIT+ and RAIT– groups. The five-year cumulative incidence rates in the RAIT+ and RAIT– groups were 3.5% [confidence interval (CI) 2.6–4.5%] and 2.0% [CI 1.0–3.5%], respectively. In both groups, there was a twofold increase in the cumulative incidence at 10 years compared to 5 years (RAIT+: 8.2% [CI 6.6–9.9%]; RAIT–: 4.5% [CI 2.6–7.0%]). The cumulative incidence of SPC was consistently higher in the RAIT+ compared to the RAIT– group throughout the entire follow-up, and this difference was statistically significant (p = 0.026; Fig. 1A). The absolute risk increase of SPC 10 years after RAIT/index date in RAIT+ versus RAIT– was 0.039 [CI 0.011–0.067] per patient-year. Based on this result, it is thus estimated that on average, for every 25.6 patients exposed to RAIT, there is one patient with SPC at 10 years of follow-up who would not otherwise occur if RAIT had not been administered (NNH = 25.6 [CI 15.0–87.2]).
Cumulative incidence of second primary cancer (
Table 3 presents the results of the multivariable analysis. In both Fine and Gray and Cox regression models, treatment with RAI had a significant impact on the development of SPC. Indeed, in the Cox model, there was a 86% increase in the hazard of SPC in the RAIT+ group compared to the RAIT– group when controlling for age, sex, and familial and personal history of cancer (HRadjusted = 1.86 [CI 1.03–3.36]). Similarly, the Fine and Gray model showed a 84% increase in the risk of SPC in the presence of the competing event death and controlling for the factors age, sex, and familial and personal history of cancer (relative risk [RR]adjusted = 1.84 [CI 1.02–3.31]).
The cumulative incidence functions of SPC by total activity administered, calculated as part of the exploratory analysis, are presented in Figure 1B.
The cumulative incidence was consistently similar between patients not treated (0 mCi) versus treated with activities <100 mCi (p = 0.700) and patients not treated (0 mCi) versus treated with activities between 100 and 199 mCi (p = 0.079).
A trend was found for an increasing cumulative incidence of SPC with higher activity (10-year cumulative incidence rates of SPC in groups who received 0, <100, 100–199, 200–299, and ≥300 mCi were 4.4%, 3.9%, 7.5%, 11.8%, and 10.9%, respectively).
Similarly, the exploratory multivariable analysis concerning the RAIT cumulative activity administered also indicated an increase in the risk of SPC with increasing cumulative activity of radioiodine (Table 4). Compared to no RAIT, the relative risk of SPC ranged from a non-statistically significant increase of 1.2-fold in the group receiving <100 mCi to a 2.3- to 2.4-fold statistically significant increase for activities of ≥200 mCi (Table 4).
Sensitivity analysis
This analysis was performed to test the robustness of the results when considering different SPC latency periods and to overcome the possible influence of breast cancer, which was the most common SPC in this cohort (Table 5).
Base case scenario analysis: all patients included (n = 2031); latency period for SPC classification: diagnosis >1 year after first radioiodine treatment administration/index date.
SPC, second primary cancer.
The analysis considering longer latency periods (>3 and >5 years after RAIT/index date, instead of >1 year) showed a consistently higher cumulative incidence of SPC in patients submitted to RAIT. Nevertheless, these results were not statistically significant, probably due to the decrease in the number of SPC, which was around 50% in the >5 years latency period scenario. After excluding the 40 patients with breast cancer, the cumulative incidence of SPC was still significantly higher in the RAIT+ compared to the RAIT– group (p = 0.026; Table 5).
SIR of SPC
The SIR of SPC was higher in the WDCT cohort compared to the general population (SIR = 1.32; Table 6). There was also a difference between the RAIT+ group and the general population (SIR = 1.40), but this was not verified in the RAIT– group (SIR = 1.02).
Discussion
A retrospective cohort study was conducted in a reference tertiary cancer center, which included 2031 patients with WDTC, with a minimum follow-up of five years. The majority of patients (77%) underwent RAIT. The observed 10-year cumulative incidence was 8.2% in the RAIT+ group [CI 6.6–9.9%] and 4.5% in the RAIT– group [CI 2.6–7.0%]. The absolute risk increase of SPC 10 years after RAIT/index date was 0.039 [CI 0.011–0.067] per patient-year in the RAIT+ compared to the RAIT– group. The calculated NNH was 25.6 [CI 15.0–87.2], which indicates that on average, during a 10-year follow-up period, there is one additional case of SPC for every 26 patients receiving RAIT, which would not otherwise occur if RAIT had not been administered.
When controlling for age, sex, and familial and personal history of cancer, the results indicate a 84% increase in the risk of SPC in WDTC patients submitted to RAIT compared to those not treated with RAI. In addition, an independent association was found between SPC cumulative incidence and total activity administered, which was statistically significant for activities ≥200 mCi. Also, after adjusting for sex, age, and calendar-year period, patients with WDTC had a higher incidence of SPC compared to the general population (SIR = 1.32). The same was also verified in the RAIT+ group (SIR = 1.40) but not in the RAIT– group (SIR = 1.02).
Published studies about the influence of RAIT in the development of SPC show conflicting data. Some studies found, similar to the present observation, an increased incidence of SPC in patients submitted to RAIT (10,11,15,25,26). These studies included a European pooled analysis (SIR = 1.3) (10), as well as two studies published in 2015, one from the United States based on the SEER database (SIR = 1.42) (11), and another from Taiwan based on the National Health Insurance database (SIR = 1.41) (26).
Other authors did not find a significant association between RAIT and SPC (14,17,27,28). In 2015, Ko et al. (28) performed a nationwide study based on the Taiwan National Health Insurance Database, which included 1834 patients. They found that there was a tendency for an increased incidence of SPC in the RAIT group, but statistical significance was not detected.
In the present series, the most common SPC was breast cancer (31%), followed by genitourinary and gastrointestinal cancers (18% each). Many studies have reported an association between RAIT and solid tumors (10,11,15,25,28 –30) without consistency across these studies.
Regarding breast cancer, some studies have also reported an association with RAIT (15,26,29,30). Theoretically, this association might be caused by different factors such as female predominance in WDTC survivors, genetic predisposition, diagnostic bias due to a stringent follow-up, or the presence of sodium–iodide symporters in mammary tissue leading to radioiodine uptake (14,31). In the present study, the RAIT+ and RAIT– groups had a similar sex distribution and follow-up procedures. Furthermore, to rule out potential genetic influences, a multivariable analysis was conducted controlling for familial and personal history of cancer, and the results were consistent with an independent effect of RAIT. In addition, to confirm the robustness of the data further, a sensitivity analysis was performed by excluding breast cancers, but the difference between the RAIT+ and RAIT– groups remained significant.
In spite of the known association between leukemia and other myelodysplastic syndromes with radiation exposure, in this study, the majority of SPC were solid tumors, and only 9% of the SPC were hematological. This is in agreement with many previous studies (11,15,25,26). In the present series, the median and mean times for developing a SPC were 5.1 and 5.4 years (range 1.1–13.8) in the RAIT+ group and 6.2 and 6.4 years (range 1.0–12.3) in the RAIT– group, respectively. These are somewhat lower than the published data, which refer median and mean latency periods for the development of SPC ranging from 8 to 16 years (11,15,29,30,32) and from 5 to 15 years (10,14,27,32), respectively.
Besides the findings of an increased incidence of SPC in the RAIT+ group compared to the RAIT– group, an increasing incidence of SPC according to the total RAI activity administered was also found, which was statistically significant for activities >200 mCi. The results are consistent with the findings previously published by other groups: a Taiwan National Health Insurance Database study published by Teng et al. (26) reporting an increased risk of SPC, especially with cumulative RAI doses >150 mCi (however, in this study, patients treated with radiotherapy were not excluded); a study by Lang et al. (30) showing that the cumulative RAI activity between 80 and 240 mCi (RR = 2.38) and external local radiotherapy (RR = 1.95) were significant risk factors for the development of SPC; and a study by Hyeon et al. (33) reporting that the risk for leukemia was increased in patients treated with activities >100 mCi.
It has often been discussed that other factors besides radiation can be associated with SPC. Several studies showed that the overall risk of SPC in thyroid cancer survivors is related to the following factors: sex (17,26), previous history of cancer (18), age at thyroid cancer diagnosis (15,17,18,26,27,29), latency period to the development of a SPC (26), genetic factors (14,15,25), and follow-up bias (24). In the present study, all these potential confounding factors were considered in the multivariable and sensitivity analyses.
To the authors' knowledge, this is the largest study of SPC in WDTC carried out by a single institution in Europe, with a median follow-up period of 8.8 years. When comparing to others, one should consider that in the present study, a prior power calculation of the sample size was performed, an index date was obtained, and a case group (RAIT+) and a control group (RAIT–) were established with the aim of adequately comparing the two groups. Furthermore, potential genetic factors were controlled by taking into account the familial and personal history of cancer, and patients with previous radiation exposure as well as patients submitted to adjuvant external radiotherapy were excluded to minimize the possibility of radio-induced cancer bias. All patients included in this study were treated and followed up at the same institution, which is a cancer referral center that follows international guidelines, assuring treatment homogeneity among all patients. Also, the retrieval of information from the Regional Cancer Registry about the diagnosis of SPC and patient survival guarantees that any SPC diagnosed in other institutions has been included in this analysis. A rigorous statistical analysis and a quality control analysis were performed to prevent potential bias for SPC, namely for breast cancer. All these aspects increase the confidence in the obtained results.
There might be some limitations to the study related to the retrospective data collection and the bias associated with a single-center study. These could be mainly due to the impossibility of performing internal dosimetry in the analyzed period and controlling for other potentially important confounders (i.e., occupational and environmental radiation exposure, smoking habits, and comorbidities), as well as due to the missing data concerning familial history of cancer in 19% of patients. Nevertheless, and for the reasons explained above, it is considered that SPC under-reporting is very unlikely.
RAIT has been used in clinical practice for about 70 years, and its good results have been confirmed and accepted. Nevertheless, the present data indicate that there is a low but significant risk for SPC after RAIT, particularly for 131I activities >200 mCi. Considering the excellent survival rate of patients with WDTC, clinicians need to weigh the risks and benefits of RAIT, especially in patients with low-risk thyroid cancer.
Footnotes
Acknowledgments
The authors would like to acknowledge the Regional Oncological Register, South Section, for the assistance in the data extraction and SIRs calculation, and the Portuguese Institute of Oncology, Lisbon Centre, and the Oncologic Endocrinology Association, for giving the opportunity to conduct this study. Also iNOVA4Health—UID/Multi/04462/2013, a program financially supported by Fundação para a Ciência e Tecnologia / Ministério da Educação e Ciência, through national funds and co-funded by FEDER under the PT2020 Partnership Agreement is acknowledged.
Author Disclosure Statement
No competing financial interests exist.