
Abstract
Background:
High-intensity focused ultrasound (HIFU) is a new promising thermal ablation technique for treating benign thyroid nodules, but its effectiveness in larger-sized nodules has been less well described. The present study aimed to evaluate the treatment efficacy (i.e., extent of shrinkage at six months) of large-sized benign thyroid nodules by ultrasound (USG)-guided HIFU ablation.
Materials and Methods:
After ethics approval, all consecutive patients who underwent HIFU ablation of a symptomatic benign thyroid nodule with six or more months of follow-up were analyzed. Treated nodules were categorized according to their pre-ablation volume (group I: <10 mL; groups II: 10–30 mL; group III: >30 mL). After treatment, the nodule volume was measured by USG at one week, one month, three months, and six months. Total energy delivered to each nodule (in kJ) and the time taken (in minutes) for that delivery were automatically recorded. The primary outcome was a change in nodule volume after six months, where percentage nodule volume change was calculated as (baseline volume – volume at six months)/(baseline volume) × 100. Ablation success was defined as >50% volume reduction.
Results:
Seventy-three nodules were treated successfully and followed for ≥6 months. The overall median six-month volume reduction was 68.3% (range 22.77–96.50%). At six months, group III had a significantly less volume shrinkage than group I (48.1% vs. 77.6%; p < 0.001) and group II (48.1% vs. 67.9%; p = 0.002). Also, the proportion of ablation success at six months in group III was significantly less than in the other two groups (p < 0.001). Pre-ablation nodule volume >30 mL (odds ratio = 7.813 [confidence interval 1.908–32.258]; p = 0.004) and lower total energy per nodule volume (odds ratio = 3.313 [confidence interval 1.113–9.688]; p = 0.029) were significant factors for less ablation success.
Conclusions:
Single-session HIFU ablation was highly effective in causing shrinkage of benign thyroid nodules at six months, but the extent of shrinkage for larger-sized nodules (>30 mL) was noticeably less than that of smaller-sized nodules. Both pre-ablation nodule volume and total energy per nodule volume were significant determinants of ablation success. For larger-sized nodules, additional HIFU treatment three to six months after initial treatment might be preferred over sequential treatment within the same session.
Introduction
T
High-intensity focused ultrasound (HIFU) is another promising form of thermal ablation technique, but this has been less well reported in the literature. Its major advantages over other thermal techniques are that it can induce a focused thermal tissue destruction of up to 85°C without needle puncture and skin penetration and that its efficacy is thought to be less dependent on the skill of the operator (11 –13). However, since it only produces thermal coagulation within a small volume, as determined by the size of the focal spot, ablating a larger tissue volume may take an excessive period of time (13). Although a few studies have shown HIFU ablation could induce moderate nodule shrinkage within the first few months, they have only applied it in relatively small-sized nodules (11,12). Therefore, it remains unclear how effective HIFU ablation is at causing shrinkage in larger-sized nodules. Given these issues, the present study aimed to review the authors' experience and specifically evaluate the treatment efficacy (i.e., extent of nodule shrinkage at six months) in larger-sized benign thyroid nodules.
Patients and Methods
This retrospective analysis was approved by the local Institutional Review Board. All consecutive patients who underwent HIFU ablation of a benign thyroid nodule at the authors' institution from 2015 to 2016 were analyzed. To be eligible for HIFU ablation, patients had to fulfil the following criteria. (i) The index nodule had to be benign (i.e., Bethesda class II (14) on fine-needle aspiration cytology (FNAC)) within three months of ablation and had to have a low to very low suspicion sonographic pattern on USG (2). (ii) The index nodule (which could either be a solitary nodule or a dominant nodule within a multinodular gland) had to be causing some neck symptoms or cosmetic concern. (iii) The index nodule had to appear predominantly solid (<30% cystic component) or solid on USG. (iv) The index nodule had to be within a treatable depth (i.e., 5–30 mm from the skin to the center of the nodule) (11,12). (v) The patient had to have a normal serum free thyroxine (fT4) level and a corresponding normal or low thyrotropin (TSH) level. Patients who were aged ≤18 years or >70 years old, pregnant or lactating women, or patients with a nodule with indeterminate/malignant FNAC or with intranodular macrocalcifications (i.e., precluding HIFU treatment), history of head and neck irradiation, family history of non-medullary thyroid carcinoma, pre-existing vocal cord palsy, or any medical conditions precluding intravenous sedation were not considered suitable for HIFU ablation. During this study period, no upper size limit was imposed for HIFU ablation. All USG assessments including the baseline and at subsequent visits were conducted by an independent, experienced sonographer not directly involved with the study. For the present study, only patients with six or more months of follow-up after ablation were included. After treatment, the treated nodule was measured by USG at one week, one month, three months, and six months. To evaluate the association between nodule volume and treatment efficacy, patients were categorized into three groups: group I—those with a pre-ablation nodule volume <10 mL; group II—those with a pre-ablation nodule volume of 10–30 mL; and group III—those with a pre-ablation nodule volume >30 mL.
Pretreatment evaluation
All thyroid swellings were graded clinically by the World Health Organization (WHO) grading system (15) and USG examination. For the latter, nodule dimensions were measured using the LOGIQ e (GE Healthcare, Milwaukee, WI) scanner equipped with a 10–14 MHz linear matrix transducer. Three orthogonal diameters of the index nodule (its longest diameter and two other perpendicular diameters) were measured. In general, the longest diameter was the cranio-caudal dimension (length) of the nodule, while the other two perpendicular diameters were the medio-lateral (width) and antero-posterior (depth) dimensions of the nodule. All measurements were made to the nearest 0.1 mm. To estimate nodule volume, the formula volume (mL) = (width [in cm] × length [in cm] × depth [in cm]) × (π/6) was used, where π was taken as 3.1416. Each patient's body weight (in kg), height (in cm), serum TSH (mIU/L), and fT4 (pmol/L) were also determined.
HIFU treatment
All treatments were performed by one person (B.H.L.) with more than two years of experience using the USG-guided HIFU device (EchoPulse; Theraclion, Paris, France). This device comprised an energy generator, a treatment head, a skin cooling device, and a touch-screen interface for planning. The treatment head incorporated an image transducer (7.5 MHz, 128 elements, linear array) and HIFU transducer (3 MHz, single element, 60 mm in diameter). After positioning, patients were sedated with diazepam (10–15 mg) and pethidine (50–100 mg). Under USG guidance, the treatment head was adjusted until the entire index nodule was within the treatable depth. The device computer (Beamotion version no. TUS 3.2.2; Theraclion) automatically divided the nodule into multiple ablation subunits. Each subunit measured 7.3 mm in thickness and 5 mm in width. Each subunit received a continuous eight-second pulse of HIFU energy followed by 40 seconds of cooling time before the beam moved to the adjacent subunit. This cycle continued until all subunits were ablated. To ensure safety, nearby structures such as the carotid artery, trachea, and skin were marked on the treatment screen and left unablated (Fig. 1). A laser-based movement detector enabled immediate power interruption when the patient moved or swallowed during ablation. To avoid skin burn, the skin was cooled by a balloon (filled with 10°C liquids) at the tip of the treatment head. All ablations started at 204 J/pulse and increased up to 280 J/pulse until hyperechoic marks appeared at the focal point (Fig. 1).

The touch-screen interface of the high-intensity focused ultrasound (HIFU) device. The central panel shows the top-view reconstruction of the nodule, which is made up of multiple white circles. The empty circles represent the unablated subunits, while the filled circles represent the ablated subunits. The hyperechoic marks (a sign of tissue necrosis) from the ablation are pointed by the two white arrows. CA, common carotid artery.
Treatment parameters
Both the total energy delivered to each nodule (in kJ) and the time taken (in minutes) for that delivery were automatically recorded by the computerized device. The former was defined as the actual energy received by the nodule (i.e., by subtracting any energy loss between the skin and the center of the intended treated area from the actual energy generated by the HIFU device), while the latter was defined as the time interval between the first and the last HIFU treatment pulse given to the index nodule. During treatment, patients' vital signs were continuously monitored. Any skin burn, swelling, and hoarseness of the voice during HIFU were recorded. Patients were asked to rate their pain during treatment, immediately after treatment, and before hospital discharge on a visual analogue scale (VAS; 0 = “no pain” and 10 = “worse possible pain”). Immediately after ablation, a transcutaneous laryngeal USG (TLUSG) was done to assess the mobility of both vocal cords (16).
Follow-up evaluation
During the first week, patients were specifically instructed to record any specific problems/complaints related to the treatment (such as swelling or dysphonia). The dimensions of the treated nodule were measured by USG at one week, one month, three months, and six months after treatment. The volume reduction ratio (VRR) was calculated based on the formula (baseline volume – volume at visit)(baseline volume) × 100. Ablation success was defined as >50% volume reduction from baseline. Total energy delivered per nodule volume was calculated based on total energy delivered divided by pre-ablation nodule volume (kJ/mL). At six months, the treated nodule was re-evaluated clinically using the WHO grading system (15). Serum TSH and fT4 were repeated at six months.
Statistical analysis
Continuous variables are expressed as median (range), and groups were compared using the Mann–Whitney U-test. Chi-square tests were used to compare categorical variables. For the correlation between continuous variables, Pearson's correlation test was performed. Changes in TSH over time were evaluated by Wilcoxon signed-rank test. Both the univariate and multivariate analyses were done by binary logistic regression analysis. Any parameters significantly associated with ablation success in the univariate analysis were entered into multivariate analysis. The area under a receiver characteristic (ROC) curve (AUC) was used to measure the relative predictability of significant factors. To improve clinical utility of continuous variables, Youden's index was used to calculate the best cutoff value. All statistical analyses were conducted using SPSS Statistics for Windows v18.0 (SPSS, Inc., Chicago, IL) and R v2.14.0 (R Foundation for Statistical Computing, Vienna, Austria). p-Values of ≤0.05 were considered statistically significant.
Results
Of the 75 patients who completed HIFU ablation, two were excluded because of incomplete six-month follow-up data. All patients completed their treatment in the outpatient setting (i.e., no overnight hospital stay), as well as their six-month scheduled visits and USG assessments.
In terms of baseline characteristics, age at treatment, body weight, height, body mass index (BMI), serum TSH and fT4, and side of nodule were similar between groups (see Table 1). However, group III had significantly more male patients than group I did (26.7% vs. 0.0%; p = 0.008). Also, group III had significantly more WHO grade 3 swelling than group I did (73.3% vs. 22.6%; p = 0.003). On USG, the median nodule width (p < 0.001), length (p < 0.001), and depth (p < 0.001) were significantly greater in group III than those in the other two groups.
Continuous variables were expressed as median (range); numbers in parentheses are percentages. Statistically significant values are shown in bold.
Group I vs. group III.
Group II vs. group III.
By Mann–Whitney U-test.
By chi-square test.
WHO, World Health Organization (grade 1a = palpable but not visible when neck is extended; grade 1b = palpable and visible when neck extended; grade 2 = visible when neck is in the normal position; grade 3 = visible from distance); TSH, thyrotropin; fT4, free thyroxine.
Perhaps owing to the larger nodule dimension, the median distance from skin to center of the nodule was significantly longer in group III than it was in group I (21.8 mm vs. 18.0 mm; p = 0.026), and this also almost reached significance between group III and II (21.8 mm vs. 17.3 mm; p = 0.076; Table 2). As expected, due to the larger nodule volume, both the total energy delivered and the ablation time in group III were the highest among the three groups (p < 0.001). However, the total energy delivered per nodule volume in group III was the lowest in the three groups (p < 0.001). In fact, the total energy delivered per nodule volume in group III was less than one-third of that in group I and roughly half of that in group II. However, pain scores appeared similar between the three groups during treatment, immediately after treatment, or before hospital discharge (p > 0.05).
Statistically significant values are shown in bold.
Group I vs. group III.
Group II vs. group III.
Calculated by total energy delivered (kJ) divided by nodule volume before ablation (mL).
By Mann–Whitney U-test.
VAS, visual analogue scale (0–10).
First six-month changes in nodule volume after HIFU ablation
Interestingly, in all three groups, there was an overall volume increase at one week from baseline (p < 0.05; Fig. 2). For group I, 20 (64.5%) patients had a median increase of 10.58% (range 1.37–47.11%), while the rest either had similar volume (±1%; n = 2) or size reduction (n = 9), with a median decrease of 3.84% (range 1.38–14.53%). Similarly, for group II, 21 (77.8%) patients had a median increase of 7.91% (range 1.39–31.74%) at one week, while the other six patients had similar volume (±1%), and no patients had a size reduction. For group III, at one week, 13 (86.7%) patients had a median increase of 3.43% (range 1.22–9.06%), while the rest either had similar size (±1%; n = 1) or reduced size (n = 1), with a median decrease of 8.28%. Although at one month all three groups had an overall nodule volume decrease from baseline (p < 0.05; Fig. 2), the extent of this volume decrease did not differ between the three groups (Table 3). However, at three months, there was a tendency for a larger median volume decrease from baseline in group I than in group III (54.5% vs. 40.0%; p = 0.073) and a larger volume decrease in group II than in group III (43.0% vs. 40.0%; p = 0.072). At six months, group III had a significantly less volume decrease than group I (48.1% vs. 77.6%; p < 0.001) and group II (48.1% vs. 67.9%; p = 0.002). Also, the proportion of successful ablation at six months in group III was significantly less than in group I (40.0% vs. 83.9%) and group II (40.0% vs. 85.2%). However, there was no significant difference in volume decrease between groups I and II at three months (p = 0.646) and six months (p = 0.102). The overall median six-month volume reduction was 68.3% (range 22.77–96.50%; Fig. 3).
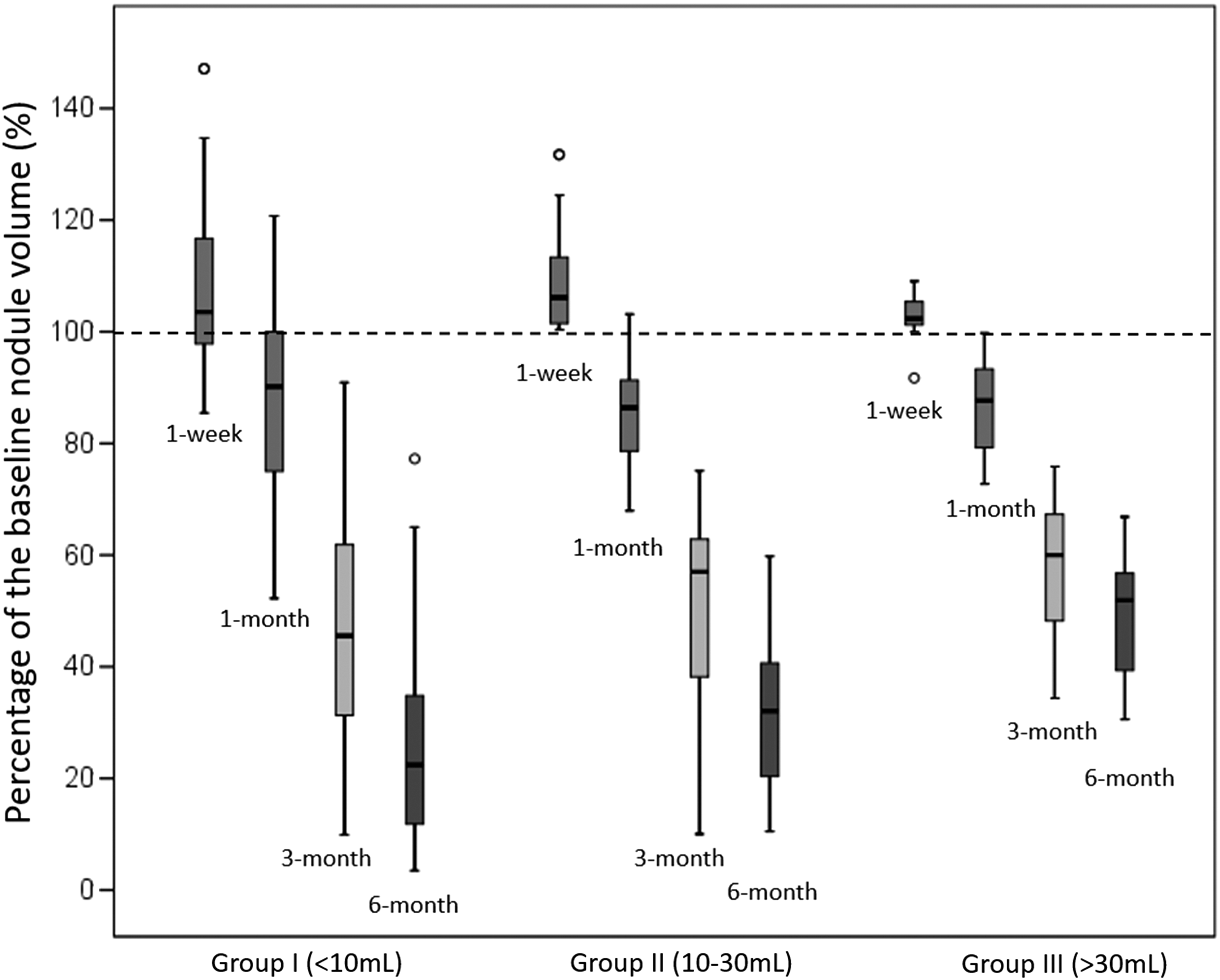
Boxplots of the six-month percentage change from the baseline volume between those with pre-ablation nodule volume <10 mL (n = 31), 10–30mL (n = 27), and >30 mL (n = 15).
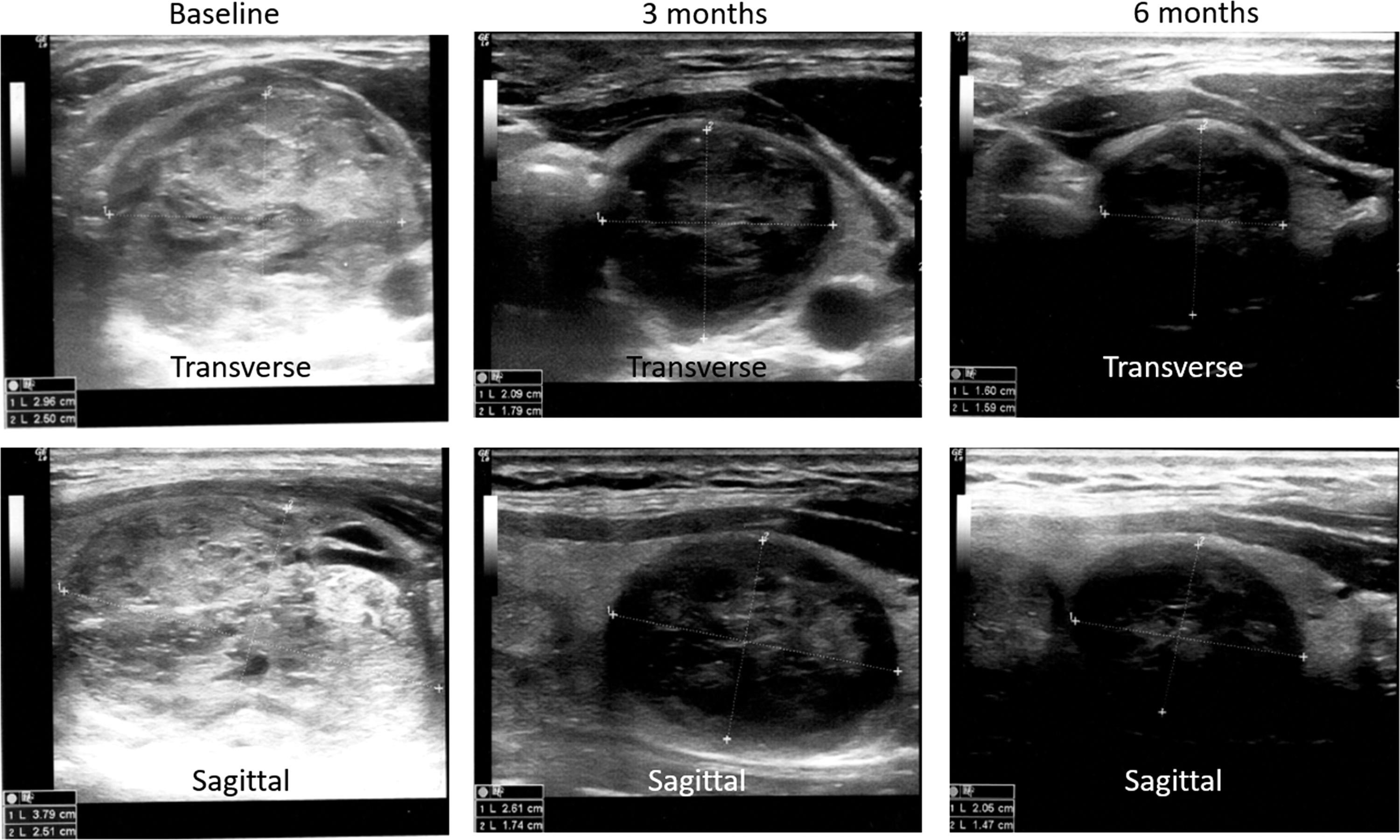
The transverse and sagittal ultrasound images obtained at baseline (before treatment) and at three and six months following HIFU treatment.
Statistically significant values are shown in bold.
Group I vs. group III.
Group II vs. group III.
Volume of a nodule (mL) = (width [in cm] × length [in cm] × depth [in cm]) × (π/6), where π was taken as 3.1416.
By Mann–Whitney U-test.
By chi-square test.
VRR, volume reduction ratio calculated by (baseline volume – volume at visit)/(baseline volume) × 100.
Consistent with these serial USG volume changes, every patient in each group had a lower WHO grade six months following HIFU (p < 0.001). In group I, of the seven patients with WHO grade 3, two (50.0%) became grade 1a while five became grade 1b. In group II, of the 16 patients with WHO grade 3, two patients with WHO grade 2 became grade 1a and the rest became grade 1b. In group III, of the 11 with grade 3, seven became WHO grade 2 and four became WHO grade 1b.
Serum TSH at six months did not significantly change from baseline in groups I (p = 0.246), II (p = 0.138), or III (p = 0.556; Table 3).
Correlation between pre-ablation nodule volume and treatment parameters
There was a significant correlation between pre-ablation nodule volume and total energy delivered (r = 0.781; p < 0.001) and also between pre-ablation nodule volume and total ablation time (r = 0.379; p < 0.001). Also, there was an inverse correlation between pre-ablation nodule volume and mean energy (kJ) per milliliter (r = −0.615; p < 0.001).
Factors leading to ablation success at six months
In univariate analysis, pre-ablation nodule volume >30 mL (odds ratio [OR] = 7.813 [confidence interval (CI) 1.908–32.258]; p = 0.004) and lower total energy per nodule volume (OR = 3.313 [CI 1.113–9.688]; p = 0.029) were significant risk factors for impaired ablation success (see Table 4). There were significant inverse correlations between six-month volume reduction and pre-ablation nodule volume (r = −0.448; p < 0.001) and between six-month volume reduction and energy per nodule volume (r = −0.511; p < 0.001). However, when both factors were entered into the logistic regression model, neither factor was significant (p > 0.05). For pre-ablation nodule volume, using an optimal cutoff of 21 mL (as determined by ROC), those with a nodule volume ≤21 mL had a significantly greater chance of ablation success at six months than those with a nodule volume >21 mL (90.6% vs. 35.0%; p < 0.001). Similarly, for total energy per nodule volume, using an optimal cutoff of 0.76 kJ/mL (by ROC), those who received ≥0.76 kJ/mL had a significantly greater chance of ablation success at six months than those who received <0.76 kJ/mL (92.3% vs. 35.0%; p < 0.001).
Using an optimal cutoff of 8.2 mL (by ROC), those with an initial nodule volume ≤8.2 mL had a significantly greater chance of ablation success than those with an initial volume >8.2 mL (100% vs. 25%; p < 0.001). Statistically significant values are shown in bold.
Entered as a dichotomized variable (>50% or ≤50%); there were 18 (81.8%) patients who achieved ablation success.
Discussion
To date, the present study is one of the largest series on the use of HIFU ablation treating symptomatic benign thyroid nodules. The data show that the overall median six-month nodule shrinkage was 68.3% (range 22.77–96.50%) from baseline with a single HIFU treatment. This appears comparable to that of other thermal ablation techniques in treating solid or predominantly solid benign thyroid nodules when only a single treatment was applied (8 –10).
In agreement with the initial hypothesis, the data show that the extent of nodule shrinkage at six months for larger-sized nodules (i.e., nodule volume >30 mL) was significantly less than that with nodules with a volume ≤30 mL (p < 0.001). In fact, there was a clear inverse association between pre-ablation size and extent of nodule shrinkage (r = −0.448; p < 0.001). By ROC analysis, this study was able to show that for nodules ≤21 mL, a single application of HIFU ablation had almost a 91% chance of achieving >50% nodule shrinkage at six months, while for nodules >21 mL, the chance dropped to just 35% (or one in three treatments achieving successful ablation). This percentage is similar to a previous study evaluating RFA as a form of thermal ablation (17). In that particular study, the authors found that for nodules >20 mL, almost three-quarters required additional ablations because of a less than optimal response following initial RFA ablation (17). If one is to translate nodule volume into a single nodule dimension, a 20 mL nodule would roughly translate into a 3.4 cm spherical nodule. This information is clinically relevant, as it would help clinicians to manage patient expectations better before treatment.
One explanation for this association between pre-ablation volume and efficacy is related to the fact that the current USG-guided HIFU device does not generally allow complete ablation in an area >3.5–4.0 cm (because of the mechanical limits of the device). Therefore, for a nodule >5–6 cm in dimension, some parts of the nodule are often left unablated. This is also the precise reason why the energy per volume (kJ/mL) in group III was the lowest in the three groups.
One point worth highlighting is that although the total energy delivered increased with the nodule volume, the increase in energy does not match the increase in nodule volume, and therefore there was a progressive fall in energy per nodule volume from group I to III (Table 2). However, despite this fall in energy per volume, the nodules in group II still appeared to have comparable treatment responses and a rate of ablation success compared to group I (85.0% vs. 83.9%; p = 0.102). Therefore, one could argue that the current treatment approach is capable of treating nodules up to 30 mL without a significant drop in efficacy. Also, one can also argue that the nodules of the patients in group I might have been overtreated and could have received less energy for a similar efficacy. This finding is consistent with some studies that showed that higher energy delivery may not always translate into greater nodule shrinkage. Perhaps a prospective study could be conducted to find out what the optimal (lowest) energy level in HIFU ablation is without compromising efficacy.
In the future, in order to achieve a higher percentage of successful ablation of nodules >30 mL, one possible solution may be to perform two sequential treatments in the same session, with one ablating one part of the nodule and the other ablating the other part of the nodule. An alternative would be to ablate the index nodule in different directions (i.e., multidimensional HIFU treatment). However, given the relatively long ablation time (with a median of 82 minutes) per treatment, these options might prove prohibitive. An alternative would be either to apply an additional treatment three to six months after the initial treatment when the rate of nodule shrinkage has begun to stabilize (17,18) or to alter the current ablation strategy from ablating only the central layer of the nodule to the circumferential layer of the nodule in order to improve the ablation efficiency (19).
Although thermal ablation of cytologically benign thyroid nodules has been available for more than 10 years (5), it remains unclear how thermally treated nodules behave in the longer term. Therefore, at least half-yearly USG assessment is recommended in the first three years and yearly assessment thereafter. It also remains uncertain how this ablation may affect subsequent surgical dissection and complications when a patient eventually requires an open cervical thyroidectomy at a later time point. In theory, it is possible that the ablation itself could induce intense scarring and fibrosis around the nodule (and the thyroid gland), making subsequent dissection more difficult and risky. Further studies are required to address some of these issues.
Lastly, several shortcomings of this study should be acknowledged. First, this was a non-randomized study, and selection biases could have influenced some of the results. Second, the study was relatively small, and therefore the results are prone to type II errors.
Conclusion
Patients who underwent a single session of HIFU ablation as treatment for their symptomatic benign thyroid nodule had significant (median = 68.3%; range 22.77–96.50%) nodule volume reduction on USG at six months. However, the extent of nodule shrinkage at six months for larger-sized nodules (i.e., nodule volume >30 mL) was significantly less than for nodules with a volume ≤30 mL (p < 0.001). Both pre-ablation nodule volume and lower total energy per nodule volume were significant determinants in ablation success. For larger-sized nodules, additional HIFU treatment(s) three to six months after initial treatment might be preferred over sequential treatment within the same session.
Footnotes
Acknowledgments
We would like to thank Dr. Vivian Man for helping with the clinical and ultrasound assessments. Also we would like to thank Mr. Yu Ming Sing and Ms. Li Wing Kar for their help with data collection.
Author Disclosure Statement
The authors declare that they have no competing interests and nothing to disclose.