
Abstract
Background:
Follicular variant of papillary thyroid carcinoma (FVPTC) is traditionally divided into infiltrative and encapsulated types. Adding to this classification, noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) represents a reclassification of a subset of cases (encapsulated tumors without lymphovascular or capsular invasion). The purpose of this study was to assess the role of ultrasound (US) in predicting tumor invasiveness in FVPTC.
Methods:
From January 2014 to May 2016, preoperative US examinations were performed on 151 patients with 152 FVPTCs who underwent surgery. Based on a pathologic analysis, the FVPTCs were categorized into three groups: NIFTP, invasive encapsulated FVPTC (iE-FVPTC), or infiltrative FVPTC (I-FVPTC). Each nodule was categorized based on the US pattern according to the Korean Thyroid Imaging Reporting and Data System (K-TIRADS) and the American Thyroid Association (ATA) guidelines. The correlation between tumor invasiveness and the K-TIRADS or ATA category was investigated using Spearman's rank correlation coefficient.
Results:
Among the 152 FVPTCs, there were 48 (31.6%) NIFTPs, 60 (39.5%) iE-FVPTCs, and 44 (28.9%) I-FVPTCs. US characteristics of the FVPTCs differed significantly according to tumor invasiveness (p ≤ 0.030). Tumor invasiveness showed a significant positive correlation with K-TIRADS (tumors of all sizes: r = 0.591, p < 0.001; tumors ≥1.0 cm: r = 0.427, p < 0.001) and ATA categories (tumors of all sizes: r = 0.532, p < 0.001; tumors ≥1.0 cm: r = 0.466, p < 0.001). According to both K-TIRADS and ATA guidelines for all-sized tumors, the most common subtype was NIFTP in low-suspicion nodules (52.6% and 51.6%), iE-FVPTC in intermediate-suspicion nodules (52.7% and 54.2%), and I-FVPTC in high-suspicion nodules (82.5% and 69.4%). After surgery, lymph node metastases were confirmed in two (4.2%) NIFTP cases, three (5.0%) iE-FVPTC cases, and eight (18.2%) I-FVPTC cases (p = 0.001). The results of the BRAF mutation analysis were not significantly different between the groups (p = 0.507).
Conclusions:
Increasing tumor invasiveness from NIFTP to iE-FVPTC to I-FVPTC is positively correlated with the level of suspicion on US using both K-TIRADS and ATA guidelines.
Introduction
F
High-resolution ultrasound (US) examination of thyroid nodules is well known for its high performance in discriminating between benign and malignant lesions. For many years, there have been numerous different guidelines and recommendations outlined by different organizations for the management of thyroid nodules detected on US (7 –11). The Korean Thyroid Imaging Reporting and Data System (K-TIRADS) and the American Thyroid Association (ATA) guidelines were most recently revised in 2016 and 2015, respectively.
Previous studies (12,13) have shown associations between malignant US features, BRAF mutation, and unfavorable clinicopathologic characteristics in FVPTC. Meanwhile, in a multicenter study using K-TIRADS, non-NIFTP lesions demonstrated a significantly higher rate of “high suspicion of malignancy” on US than NIFTP did (14). However, to the authors' knowledge, no studies have examined the relationship between US findings of FVPTC and the degree of tumor invasiveness from NIFTP to iE-FVPTC to I-FVPTC. Therefore, the purpose of this study was to assess the role of US in predicting tumor invasiveness in FVPTC using the K-TIRADS categories and the ATA classification.
Materials and Methods
Study population
This retrospective study was approved by the Institutional Review Board (IRB) of the Samsung Medical Center, and the IRB gave a waiver of informed consent for the use of data. A total of 168 patients with 169 FVPTCs who underwent US examinations before surgery between January 2014 and May 2016 were included in the study. Patients who had a small cancer (≤0.5 cm; n = 12), multiple thyroid nodules with a lack of correlation between US findings and pathological findings (n = 4), and an incidental PTC within benign hyperplasia (n = 1) were excluded. Therefore, the study included 151 patients with 152 FVPTCs. There were 39 men (M age = 49.6 years; range 21–70 years) and 112 women (M age = 49.0 years; range 17–76 years), with an overall mean age of 49.1 years (range 17–76 years). The mean tumor size was 1.7 cm (range 0.6–5.6 cm).
US examinations and US image analyses
All thyroid US examinations were performed with a 5–12 MHz linear array transducer (iU22; Philips Medical Systems, Bothell, WA) by eight radiologists (four faculty members, four fellows) with 1–10 years of experience in thyroid imaging.
All US images were retrospectively reviewed and interpreted with consensus by two faculty radiologists (S.Y.H. and J.H.S.) who were blinded to the clinicopathologic characteristics. Each nodule was categorized based on the US pattern according to the 2016 revised K-TIRADS (8) and the 2015 revised ATA (7) guidelines.
All thyroid nodules were described in terms of composition, internal echogenicity, orientation, margin, shape, calcifications, halo, and vascularity on Doppler scan. The internal composition was categorized as solid (no obvious cystic content), predominantly solid (≤50% of the cystic portion), predominantly cystic (>50% of the cystic portion), or cystic (no obvious solid content). The echogenicity was categorized as marked hypoechoic, hypoechoic, isoechoic, or hyperechoic. The orientation was classified as parallel or nonparallel. The margin was classified as smooth, ill-defined, microlobulated, or spiculated. The shape was categorized as round to oval or irregular. If calcifications were present, they were classified as microcalcifications (≤1 mm in size), macrocalcifications (>1 mm in size with posterior shadowing), or rim calcifications. A halo was determined to be present when a hypoechoic rim surrounding a thyroid nodule was observed. When Doppler images were available for review, the vascularity patterns of thyroid nodules were categorized into four types: type 1, absence of nodule vascularity; type 2, perinodular vascularity only; type 3, mild intranodular vascularity with or without perinodular vascularity (vascularity <50%); and type 4, marked intranodular vascularity with or without perinodular vascularity (vascularity >50%).
For the final K-TIRADS categorization (8), thyroid nodules were classified into five groups: category 1, no nodule; category 2, benign nodule (spongiform, pure cyst, or partially cystic nodule with comet tail artifact); category 3, low suspicion nodule (partially cystic or isohyperechoic nodule without any of the three suspicious US features: microcalcification, nonparallel orientation, or spiculated/microlobulated margin); category 4, intermediate suspicion nodule (solid hypoechoic nodule without any of the three suspicious US features or partially cystic or isohyperechoic nodule with any of the three suspicious US features); category 5, high suspicion nodule (solid hypoechoic nodule with any of the three suspicious US features).
According to the ATA guidelines (7), thyroid nodules were classified as high, intermediate, low, or very low suspicion of malignancy. High-suspicion nodules were defined as solid hypoechoic nodules or partially cystic nodules with a solid hypoechoic component and at least one suspicious US feature (e.g., irregular margins [i.e., microlobulated or spiculated], microcalcifications, taller-than-wide shape [i.e., nonparallel orientation], disrupted rim calcifications with extrusive hypoechoic soft-tissue component, or findings of extrathyroidal extension). Intermediate-suspicion nodules were defined as hypoechoic solid nodules with smooth margins without microcalcifications, taller-than-wide shape, or extrathyroidal extension. Low suspicion nodules were defined as iso- or hyperechoic solid nodules or partially cystic nodules with eccentric uniformly solid areas without microcalcifications, irregular margins, taller-than-wide shape, or extrathyroidal extension. Very low suspicion nodules were defined as spongiform or partially cystic nodules without any of the US features described in the high-, intermediate-, or low-suspicion categories. It was not possible to categorize a small proportion of thyroid nodules specifically into one of the four categories (e.g., heteroechoic nodules with or without any other suspicious US features and iso- or hyperechoic nodules with at least one of the other suspicious US features), and these nodules were therefore classified as “not specified.”
Data and statistical analyses
Pathologic results from surgical specimens were considered the standard of reference. An experienced thyroid cancer pathologist reviewed all surgical specimens without knowledge of imaging findings and clinical information, and then diagnosed tumor invasiveness. Based on the pathologic analysis, FVPTCs were categorized into three groups (NIFTP, iE-FVPTC, or I-FVPTC) (6).
The chi-square or Fisher's exact test was used for categorical variables. For continuous variables, analysis of variance was utilized. The correlation between tumor invasiveness and the K-TIRADS or ATA category was investigated for tumors of all sizes and tumors ≥1.0 cm in size using Spearman's rank correlation coefficient. Analyses were performed with SAS software v9.4 (SAS Institute, Cary, NC). All tests were two-sided, and a p-value of <0.05 was considered indicative of a statistically significant difference.
Results
Of a total of 152 FVPTCs, there were 48 (31.6%) NIFTPs, 60 (39.5%) iE-FVPTCs, and 44 (28.9%) I-FVPTCs. Table 1 summarizes the clinicopathologic characteristics of the patients and nodules. I-FVPTC nodules were significantly smaller than NIFTP or iE-FVPTC nodules (M = 1.2 ± 0.7 cm, range 0.6–4.0 cm vs. 1.8 ± 1.2 cm, range 0.6–5.6 cm, or 1.9 ± 1.2 cm, range 0.6–5.4 cm, respectively; p = 0.007). The most common results of preoperative fine-needle aspiration (FNA) were atypia of undetermined significance/follicular lesion of undetermined significance (AUS/FLUS; Bethesda category III) in both the NIFTP and iE-FVPTC groups, and suspicious for malignancy (Bethesda category V) in the I-FVPTC group. Following surgery, lymph node metastases were confirmed in two (4.2%) NIFTP cases, three (5.0%) iE-FVPTC cases, and eight (18.2%) I-FVPTC cases (p = 0.001). In the two cases of lymph node metastasis in the NIFTP group, there was a single metastasis that measured <0.2 cm. The tumor sizes of these two NIFTP cases were 0.7 cm and 1.3 cm. The BRAF mutation analysis results did not significantly differ between the groups (p = 0.507).
Data are number of nodules. The numbers in parentheses are percentages.
A p-value of <0.05 was considered statistically significant.
There were two cases of single lymph node micrometastasis in the NIFTP group (size of the largest metastasis: <0.2 cm).
FVPTC, follicular variant of papillary thyroid carcinoma; NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; iE-FVPTC, invasive encapsulated FVPTC; I-FVPTC, infiltrative FVPTC; SD, standard deviation; FNA, fine-needle aspiration; AUS/FLUS, atypia of undetermined significance/follicular lesion of undetermined significance; FN/SFN, follicular neoplasm/suspicion for a follicular neoplasm.
All US characteristics of the FVPTCs differed significantly according to tumor invasiveness (p ≤ 0.030; Table 2). The representative US findings of NIFTP were solid composition (77.1%), isoechogenicity (54.2%), smooth margins (89.6%), parallel orientation (93.8%), round-to-oval shape (97.9%), and no calcifications (72.9%; Fig. 1). The most common findings of iE-FVPTC on US were solid composition (85.0%), hypoechogenicity (40.0%), smooth margins (75.0%), parallel orientation (86.7%), round to oval shape (85.0%), and presence of a halo (61.7%; Fig. 2). Meanwhile, solid composition (97.7%), hypoechogenicity (45.5%), spiculated margins (38.6%), parallel orientation (54.5%), irregular shape (54.5%), macrocalcifications (40.9%), and absence of halo (88.6%) were demonstrated most frequently in I-FVPTC (Fig. 3).
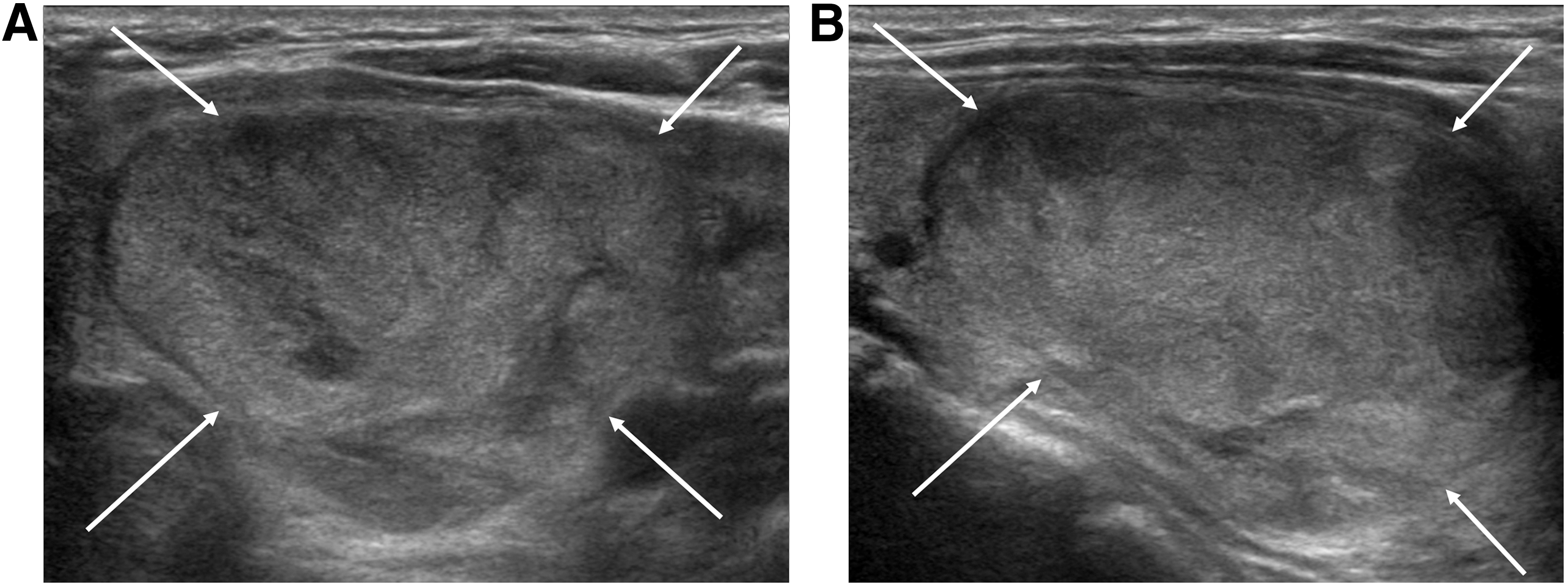
A 44-year-old man with a noninvasive follicular thyroid neoplasm with papillary-like nuclear features in the left thyroid lobe. Transverse (
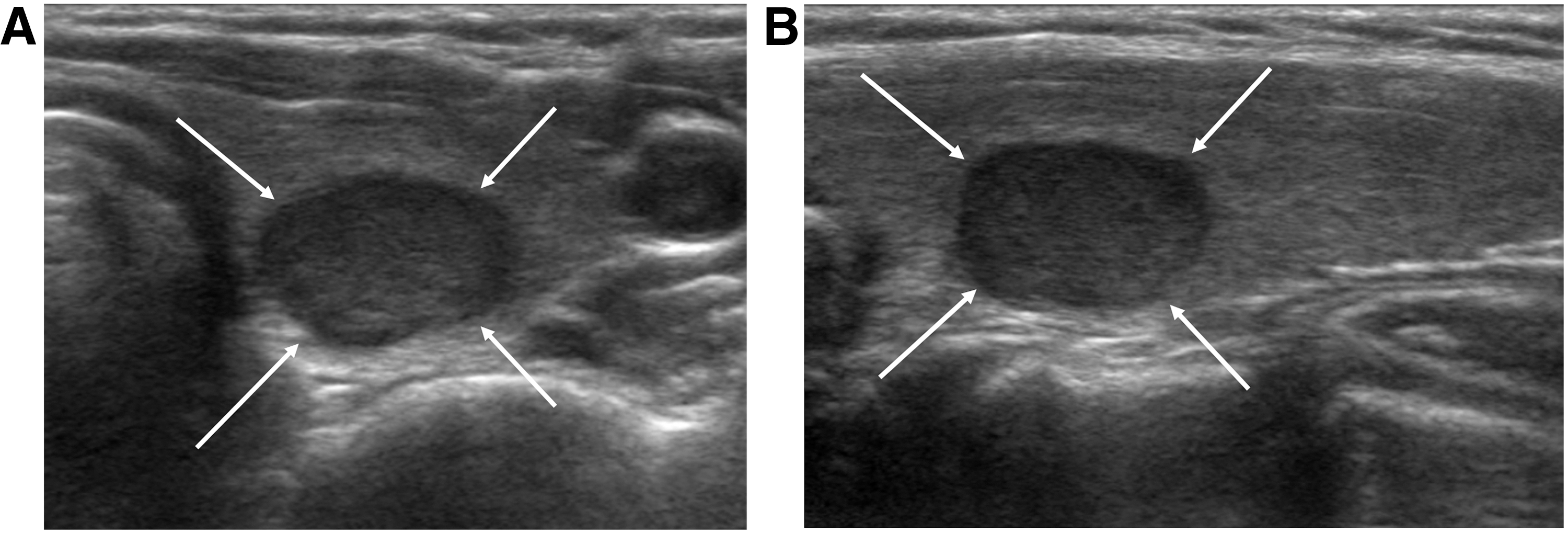
A 45-year-old woman with an invasive encapsulated follicular variant of papillary thyroid carcinoma in the right thyroid lobe. Transverse (
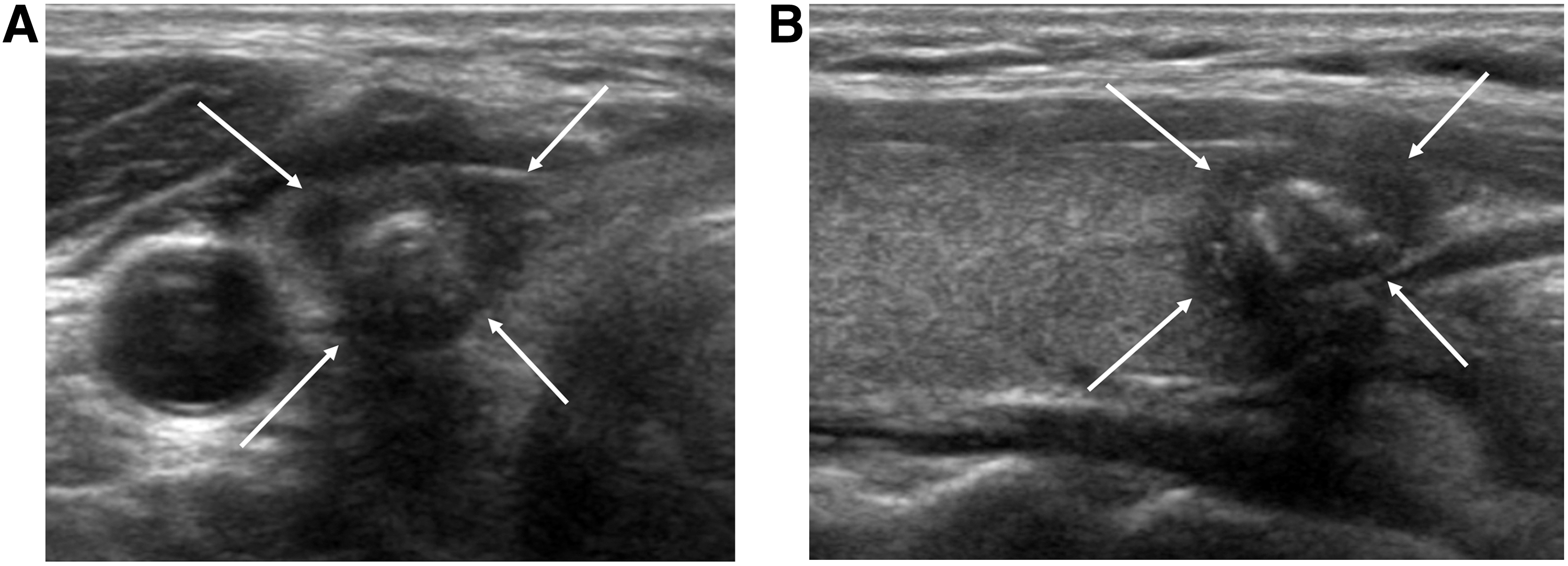
A 45-year-old woman with an infiltrative follicular variant of papillary thyroid carcinoma in the left thyroid lobe. Transverse (
Data are number of nodules. The numbers in parentheses are percentages.
A p-value of <0.05 was considered statistically significant.
Type 1, absence of nodule vascularity; type 2, perinodular vascularity only; type 3, mild intranodular vascularity with or without perinodular vascularity (vascularity <50%); and type 4, marked intranodular vascularity with or without perinodular vascularity (vascularity >50%).
Table 3 presents the relationship of tumor invasiveness to K-TIRADS category and ATA category. In assessment of the ATA categories, 17/152 (11.2%) FVPTCs were classified as “not specified” pattern for all sized tumors and 7.8% (6/77) for tumors ≥1.0 cm. Tumor invasiveness showed a significant positive correlation with K-TIRADS (all-sized tumors, r = 0.591, p < 0.001; tumors ≥1.0 cm, r = 0.427, p < 0.001) and ATA categories (all-sized tumors, r = 0.532, p < 0.001; tumors ≥1.0 cm, r = 0.466, p < 0.001). According to both K-TIRADS and ATA guidelines for all-sized tumors, the most common subtype was NIFTP in low-suspicion nodules (52.6% and 51.6%, respectively), iE-FVPTC in intermediate-suspicion nodules (52.7% and 54.2%, respectively), and I-FVPTC in high-suspicion nodules (82.5% and 69.4%, respectively; Figs. 1–3).
Data are number of nodules. The numbers in parentheses are percentages.
A p-value of <0.05 was considered statistically significant.
K-TIRADS, Korean Thyroid Imaging Reporting and Data System; ATA, American Thyroid Association.
Discussion
Previous studies have reported that iE-FVPTC has an indolent behavior and is genetically distinct from I-FVPTC (15 –18). Recently, in addition to those studies, Nikiforov et al. suggested a sub-classification, NIFTP, describing tumors without lymphovascular or capsular invasion that have a very low risk of malignancy as well as adverse outcomes (6). However, at the same time, there is the potential for overtreatment because of nuclear features that overlap those of I-FVPTC (19,20). Earlier studies demonstrated that malignant US features are associated with unfavorable clinicopathologic characteristics in FVPTC (12,13). This is consistent with the results of a previous study (14), which demonstrated that the malignancy risk predicted by K-TIRADS was significantly higher in non-NIFTP lesions than in NIFTP. The present study divided FVPTCs into three groups based on tumor invasiveness and investigated the correlation between tumor invasiveness and K-TIRADS category or ATA classification.
According to this analysis, US features differed significantly between the three FVPTC groups, and there was a significant positive correlation between tumor invasiveness and US categories for predicting malignancy. In this study, the representative US finding of I-FVPTC was an irregular hypoechoic solid mass with spiculated margins and calcifications, an US description that has already been well established through previous studies as characteristic of thyroid malignancy (8,21 –23). It also demonstrated that FVPTC had a tendency to present as a round to oval isoechoic solid mass with smooth margins and parallel orientation on US when diagnosed as NIFTP. These dichotomous findings of FVPTCs are in agreement with those described in previous studies (12,14,24 –26).
In the present study, the most frequent FNA results were AUS/FLUS (Bethesda category III) in both the NIFTP and iE-FVPTC groups and suspicious for malignancy (Bethesda category V) in the I-FVPTC group, respectively. According to recent studies (19,27 –32), NIFTPs can be diagnosed as AUS/FLUS, follicular neoplasm/suspicious for follicular neoplasm, or even suspicious for malignancy (Bethesda category III, IV, and V) on cytology. As a result, cytology is not reliable as the sole diagnostic method for predicting subtypes of FVPTCs.
The literature to date has indicated a lack of BRAF mutations in patients with nodules classified as NIFTP according to current criteria (6). In the current study, three (6.3%) NIFTP cases with a BRAF mutation and two (4.2%) NIFTP cases with micrometastases in central lymph nodes were found. Of these, two cases with a BRAF mutation and one with lymph nodal micrometastasis were tumors <1 cm in size. However, no association was observed between BRAF mutation and lymph node metastasis in the NIFTP group. Nikiforov et al. demonstrated that NIFTP has an indolent course with little metastatic potential (6). The ATA Thyroid Nodules and Differentiated Thyroid Cancer Guidelines Task Force recommended the adoption of this new terminology, but also expressed the need of further retrospective studies to validate the study by Nikiforov et al. (33). In a recent study, Zhao et al. found that one (2.0%) of their NIFTP cases was associated with a BRAF mutation (34). Additional studies with larger numbers of patients will be needed to determine the clinical significance of the presence of a BRAF mutation in NIFTP.
In the present study, I-FVPTC nodules were significantly smaller than NIFTP or iE-FVPTC nodules. Both K-TIRADS and ATA guidelines suggested size criteria for FNA based on the US findings (7,8). These recommendations could influence the mean size of thyroid nodules in the FVPTC subtype groups. According to both guidelines, thyroid nodules <1 cm in size are not generally recommended as candidates for FNA, even when they demonstrate high suspicion features on US, and thyroid FNA is recommended for low-suspicion nodules when they are ≥1.5 cm in size. In the studies describing NIFTP, all tumors were ≥1 cm in size. However, in this study, NIFTPs <1 cm in size accounted for 45.8% of cases. It has not yet been established in the literature whether it is appropriate to classify tumors <1 cm in size accurately as NIFTP.
There are several limitations to this study. First, the retrospective data collection may have introduced a substantial case selection bias. The study population included only cases that were diagnosed after surgery. The histologic subtype of FVPTCs can be determined after pathologic evaluation of surgical specimens. Second, 17 (11.2%) FVPTCs were not classified in the assessment of the ATA categories. Certain US findings are not clearly specified in the ATA classification, such as heteroechoic nodules with or without any other suspicious US features and iso- or hyperechoic nodules with at least one other suspicious US feature. However, the K-TIRADS categorization could be applied to all FVPTC lesions in the present study. The K-TIRADS category of all 17 FVPTCs, which were not classified by the ATA guidelines, was 4, the intermediate-suspicion category. Among these, six (35.3%) were NIFTPs, seven (41.2%) were iE-FVPTCs, and four (23.5%) were I-FVPTCs.
In conclusion, increasing tumor invasiveness from NIFTP to iE-FVPTC to I-FVPTC is positively correlated with the level of suspicion on US using both K-TIRADS and ATA guidelines.
Footnotes
Author Disclosure Statement
The authors declare that there is no conflict of interest in relation to this manuscript.