
Abstract
Objective:
To evaluate the efficacy and prognostic validity for disease-specific survival (DSS) of the eighth edition American Joint Committee on Cancer/Union for International Cancer Control tumor-node-metastasis (TNM) staging system (TNM-8) compared to the seventh edition (TNM-7) in patients with differentiated thyroid carcinoma (DTC).
Methods:
The seventh and eighth editions of the TNM staging system were applied to 1613 DTC patients who underwent thyroid surgery between 1996 and 2003. The proportion of variation explained and Harrell's c-index were evaluated to compare the predictive capability of DSS.
Results:
The mean age of the patients was 44.7 years, and the median follow-up period was 11.2 years. When TNM-8 was applied, 63% of T3 and 3% of N1b DTCs were downgraded to T1/T2 and N1a, respectively. About 38% of patients were downstaged according to TNM-8. The 10-year DSS rates in TNM-7 stages I, II, III, and IV were 99.7%, 98.2%, 98.8%, and 83.2%, respectively. Those in TNM-8 stages I, II, III, and IV were 99.6%, 95.4%, 72.3%, and 48.6%, respectively. The proportion of variation explained values of TNM-7 and TNM-8 were 6.0% and 7.0%, respectively. The Harrell's c-index of TNM-7 was 0.86 and that of TNM-8 was 0.88.
Conclusions:
A significant number of patients were reclassified to lower stages with the application of TNM-8 compared to TNM-7. Applying TNM-8 could improve the accuracy of the staging system for predicting DSS in patients with DTC.
Introduction
C
In the seventh edition of the TNM staging system (TNM-7), the presence of both minimal and massive extrathyroidal extension (ETE) was an important factor in the definition of T3 tumors (10). However, several studies revealed similar clinical outcomes of patients with minimal ETE and those with no ETE (3,4). Overstaging of DTC was a concern for patients with minimal ETE, including microscopic invasion when their primary tumor size was ≤4 cm. In the eighth edition of TNM staging system (TNM-8), T3 was defined as a primary tumor >4 cm in greater dimension limited to the thyroid (T3a) or gross ETE invading strap muscles only (T3b) (9). A significant number of patients with minimal ETE can thus be reclassified as T1 or T2 under TNM-8 based on the primary tumor size.
In addition, the cutoff age for patients with DTC changed from 45 to 55 years in TNM-8 (9). There is increasing evidence that a cutoff age of 45 years has led to overstaging in many patients with DTC, and using 55 years as a cutoff value in the TNM staging system may prevent overstaging in low-risk patients (5,6). This new classification can also provide a more realistic assessment of disease mortality in high-risk patients. A significant number of patients between the ages of 45 and 55 years can be reclassified to stage I or II by applying TNM-8.
This study aimed to evaluate the efficacy and prognostic validity of TNM-8 compared to TNM-7 for predicting disease-specific survival (DSS) of patients with DTC. It also evaluated how many patients would be affected by the new changes in the TNM staging system in a large cohort of patients with DTC.
Materials and Methods
Patients
This historical cohort study included 1613 consecutive patients with DTC who underwent initial thyroid surgery at the Asan Medical Center (Seoul, Korea) between January 1996 and December 2003. All patients had pathologically proven papillary thyroid carcinoma (PTC) or follicular thyroid carcinoma (FTC) including Hürthle cell carcinoma (HCC). Patients with poorly differentiated carcinomas or anaplastic carcinomas in their thyroids were excluded from this study. DSS was defined as the time from the date of surgery until last censoring or death caused by DTC. The study protocol was approved by the Institutional Review Board of the Asan Medical Center.
Surgical treatment and radioactive iodine ablation
From 1996 to 2003, the physicians and surgeons involved in the management of thyroid cancer patients at the authors' institution remained mostly the same and shared protocols to maintain uniform treatment and follow-up across patients. Prophylactic central compartment node dissection (CCND) was routinely performed, while therapeutic central and lateral neck dissection was performed in patients with clinically apparent lateral cervical lymph node (LN) metastasis, as previously reported (11,12). CCND usually involved level VI. LN dissection of level VII was undertaken only in patients with suspected metastasis in that area. The extent of CCND was cranially delineated to the superior thyroid arteries and the thyroid cartilage, caudally to the innominate vein, laterally to the carotid sheaths, and dorsally to the prevertebral fascia. Lateral neck LN dissection included levels II, III, and IV. LN dissection of level I and V were done only for suspected metastatic LNs (11,13). Radioactive iodine (RAI) remnant ablation after total thyroidectomy was performed if indicated two to three months after the initial surgery according to the protocol established by the Department of Endocrinology and Metabolism of the Asan Medical Center (14).
Follow-up protocol
The follow-up protocol after initial treatment for DTC has been previously reported (15 –17). Briefly, patients took levothyroxine for thyrotropin suppression and were regularly followed with physical examinations and measurements of thyroid function, serum thyroglobulin (Tg), serum anti-Tg antibody, and neck ultrasound every 6–12 months. Diagnostic RAI whole-body scans (WBSs) with measurement of the serum-stimulated Tg level were also performed 12–24 months after the initial therapy in patients who underwent total thyroidectomy and RAI remnant ablation. Additional diagnostic imaging studies, such as computed tomography, magnetic resonance imaging, or 18F-fluorodeoxyglucose-positron emission tomography were also performed as needed (16).
Statistical analyses
All statistical analyses were conducted using R v3.10 (R Foundation for Statistical Computing, Vienna, Austria;
The proportion of variation explained (PVE) in the Cox proportional hazard model was calculated to compare the relative validity of each TNM classification (18). PVE (%) values range from 0 to 100; larger numbers suggest better predictability. PVE was determined using the following mathematical formula: PVE = 1 – exp(–G 2/n), where G 2 is the maximum likelihood ratio that is determined by analysis using the chi-square test associated with the null hypothesis, and n is the total number of valid cases in the study (19). Furthermore, the predictive capacity of each TNM classification was evaluated using Harrell's c-index (20). A model with perfect predictive capacity (sensitivity and specificity of 100%) would have a Harrell's c-index of 1.00. A category that exhibited a higher Harrell's c-index was considered to exhibit a more accurate predictive capacity.
Results
Baseline characteristics of patients with DTC
The baseline clinical and pathological characteristics of the 1613 patients with DTC are listed in Table 1. The mean age of patients was 44.7 ± 12.3 years, and 1414 (88%) patients were female. The pathological subtype was PTC in 1526 (95%) patients, and 5% of patients had FTC, including HCC. The mean primary tumor size was 2.0 ± 1.4 cm, and 458 (28%) patients had microcarcinomas (primary tumor size ≤1 cm). According to the definitions of the AJCC/UICC TNM-7 and TNM-8 staging systems, microscopic ETE and gross ETE were found in 513 (32%) and 303 (19%) patients, respectively. Cervical LN metastases were present in 901 (56%) patients, and 29 (2%) patients had distant metastases of DTC at initial treatment. A total of 1312 (81%) patients underwent total thyroidectomy, and 1264 (78%) patients received RAI therapy. The median follow-up period until censoring or death was 11.2 years (IQR 8.8–13.3 years), and the 10-year DSS rate was 98%.
Values are shown as the mean ±standard deviation or n (%).
DTC, differentiated thyroid cancer; PTC, papillary thyroid cancer; FTC, follicular thyroid cancer; RAI, radioactive iodine.
Changes in T and N classifications from TNM-7 to TNM-8
Based on TNM-7, the number of patients in T1, T2, T3, and T4 classifications were 534 (33%), 210 (13%), 774 (48%), and 95 (6%), respectively (Table 2). When TNM-8 was applied, the number of patients in T1 and T2 classifications increased to 895 (55%) and 339 (21%), respectively. The 490 (63%) patients with T3 classification were downstaged to T1 (n = 361; 47%) and T2 (n = 129; 17%) by TNM-8. No change in the number of patients with T3 and T4 between TNM-7 and TNM-8 was observed in this study.
TNM, tumor-node-metastasis; TNM-7, seventh edition of TNM staging system; TNM-8, eighth edition of TNM staging system.
Applying TNM-8, the N classification was changed to N1a in five patients who were originally classified as N1b according to TNM-7 due to their level VII LN metastases. Among the 165 patients with N1b disease by TNM-8, 18 (11%) patients had lateral LN metastasis only, without central LN metastasis.
Comparison of the number of patients in each stage according to TNM-7 and TNM-8
Based on TNM-7, the numbers of patients in stages I, II, III, and IV were 969 (60%), 63 (4%), 460 (29%), and 121 (7%), respectively. When TNM-8 was applied, the number of patients in stage I increased to 1360 (84%) because 391 (24%) patients were downstaged to stage I (Table 3). The number of patients in stage II also increased to 211 (13%) because 153 (9%) patients and 38 (2%) patients were downstaged from stages III and IV, respectively. The number of patients in stage III by TNM-7 decreased to 30 patients by TNM-8. All these patients were downstaged from stage IV to stage III using TNM-8. Only 12 patients were classified as stage IV by TNM-8, whereas 121 patients were classified as stage IV by TNM-7.
Comparison of DSS according to TNM-7 and TNM-8 in patients with DTC
In TNM-7, the 10-year DSS rates for T1, T2, T3, and T4 classifications were 99.2%, 99.5%, 98.4%, and 86.6%, respectively (Table 4 and Fig. 1A). Patients with T4 classification had a significantly poorer DSS compared to those with T1 classification (HR = 18.4 [CI 6.6–51.1]; p < 0.001). DSS was not significantly different between T1, T2, and T3 classifications. When TNM-8 was applied, the 10-year DSS rates for T1, T2, T3, and T4 classifications were 99.0%, 99.0%, 98.5%, and 86.6%, respectively (Fig. 1B). Only patients with T4 classification had a significantly poorer DSS compared to those with T1 classification in TNM-8 (HR = 15.1 [CI 6.7–34.1]; p < 0.001).
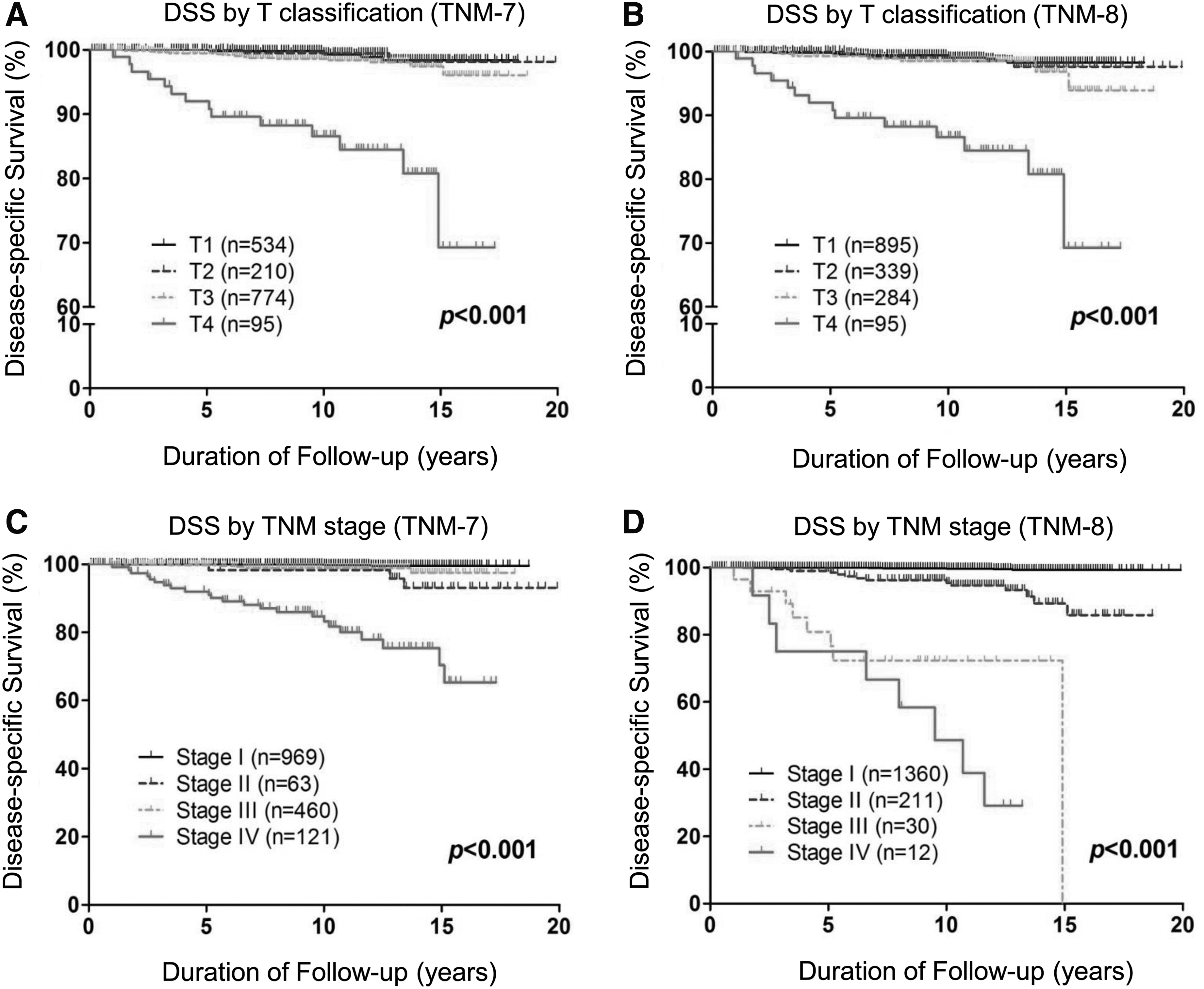
DSS curves of patients with DTC according to T classification and TNM stage. DSS curves according to the T classification of TNM-7 (
DSS, disease-specific survival; HR, hazard ratio; CI, confidence interval; PVE, proportion of variation in survival time explained.
In both TNM-7 and TNM-8, patients with N1b findings had significantly poorer DSS compared to those classified as N0.
DSS was significantly different according to TNM-7 and TNM-8, as shown in Figure 1C and D (p < 0.001 and p < 0.001, respectively). Using TNM-7, the 10-year DSS rates of staged I, II, III, and IV were 99.7%, 98.2%, 98.8%, and 83.2%, respectively (Table 4, upper panel). Patients in stages II, III, and IV had significantly poorer DSS compared to those in stage I. However, the HR of stage II was 11.9 [CI 2.4–59.3] whereas that of stage III was 4.5 [CI 1.1–18.0].
When TNM-8 was applied, the 10-year DSS rates of stages I, II, III, and IV were 99.6%, 95.4%, 72.3%, and 48.6%, respectively (Table 4, lower panel). Patients in stages II, III, and IV had a significantly poorer DSS compared to those in stage I. The HRs of stages II, III, and IV were 14.4 [CI 5.5–38.0], 108.3 [CI 37.2–315.3], and 232.6 [CI 79.6–680.3], respectively.
The PVE and Harrell's c-index of TNM-7 and TNM-8 were calculated to compare the relative predictability of DSS in patients with DTC. The PVE values of TNM-7 and TNM-8 were 6.0% and 7.0%, respectively. The Harrell's c-index of TNM-7 was 0.86 and that of TNM-8 was 0.88.
Discussion
The TNM staging system attempts to account for the most basic parameters of cancer, and it is also useful for determining the extent of disease, providing guidance for treatment planning, and predicting survival (21,22). AJCC/UICC TNM staging is recommended for all DTC patients based on its usefulness in predicting disease mortality, whereas the initial risk stratification of the American Thyroid Association is recommended for predicting risk of disease recurrence and/or persistence (1). This study compared the seventh and eighth edition of the TNM staging system in 1613 patients with DTC. When TNM-8 was applied, 38% of patients were reclassified into lower TNM stages, and 63% of patients with T3 classification were restaged as T1 or T2. The 10-year DSS rates of stages I, II, III, and IV were 99.6%, 95.4%, 72.3%, and 48.6%, respectively, by TNM-8. The PVE and Harrell's c-index values were higher in TNM-8 than they were in TNM-7. These findings suggest that TNM-8 had better predictability for DSS compared to TNM-7 because the newly revised TNM staging system could reduce the number of patients in stages III and IV.
A notable change in TNM-8 is the definition of the T3 classification of thyroid cancer (9). According to TNM-8, T3 is defined as the presence of gross ETE invading strep muscle only, regardless of the primary tumor size (10). The presence of ETE was observed in 5–45% of patients with DTC and has been recognized as an important prognostic factor in patients with DTC (23 –25). In the sixth edition of the AJCC/UICC TNM staging system, ETE began to be classified as minimal or massive ETE (10). Minimal ETE was defined as extension into the sternothyroid muscle or parathyroid soft tissues, and massive ETE as cancer invasion into the subcutaneous soft tissues, larynx, trachea, esophagus, or recurrent laryngeal nerve (10). According to previous studies, ETE has different implications depending on its extent. Studies have shown that massive ETE is associated with significantly worse survival in patients with DTC, and minimal ETE also has prognostic significance (23,26). However, some studies have reported similar clinical outcomes of patients with or without microscopic minimal ETE (3,4,27). Clinical outcomes, including persistence and recurrence of disease and mortality, are unlikely to be affected by microscopic ETE in patients with DTC (27). Therefore, overstaging of DTC with microscopic ETE was a concern in the previous AJCC/UICC TNM staging system because overstaging can lead to overtreatment in patients with low-risk DTC. When the primary tumor size of DTC was ≤4 cm, only patients with gross ETE were classified as T3, and those with microscopic ETE could be T1 or T2 staging in TNM-8. In this study, 63% of patients with T3 classification by the TNM-7 definition were reclassified as T1 or T2 by that of TNM-8.
The most significant change in TNM-8 is the definition of the cutoff age, which increased from 45 to 55 years (9). Age at diagnosis of DTC has been considered to be an important prognostic factor for survival and has been consistently included in the majority of staging systems in DTC (2,10,28 –31). The cutoff age of 45 years has been included as a non-anatomic variable for the staging of DTC since the second edition of the AJCC/UICC TNM staging system, published in 1983 (2,10). However, recent studies have suggested that 45 years of age may not be the most statistically robust cutoff value for the TNM staging system (5,7,8,32). Increasing evidence has suggested that a cutoff age of 45 years leads to overstaging in a significant number of patients. Two multi-institutional studies suggested that 55 years is the most relevant cutoff age for TNM staging of DTC for preventing overstaging in low-risk patients and providing a more practical estimate of prognosis in high-risk patients (5,6). In this study, 431 (27%) patients were between 45 and 55 years of age, and their TMN stage was reclassified as stage I or II with the application of TNM-8.
In this study, patients with stage I or II DTCs exhibited favorable prognosis, regardless of whether TNM-7 or TNM-8 was applied. The 10-year DSS rates in patients with stages I and II according to TNM-7 were 99.7% and 98.2%, respectively. The corresponding rates according to TNM-8 were 99.6% and 95.4%, respectively. However, the DSS of patients with stages III and IV according to TNM-8 were poorer than those by TNM-7. Based on TNM-7, the 10-year DSS rates in patients with stages III and IV DTC were 98.8% and 83.2%, respectively. When TNM-8 was applied, the 10-year DSS rates in patients with stages III and IV DTC were 72.3% and 48.6%, respectively. Considering the superior predictive validities for DSS in both PVE and Harrell's c-index, the application of TNM-8 has a clinical benefit of more precise risk stratification for determining the intensity and extent of initial treatment, as well as preventing overtreatment in lower-risk patients with DTC.
This study has some notable limitations. First, there is a possibility of selection bias, since the study patients were recruited from a single tertiary referral institution. However, the surgical procedures, pathologic examinations, and patient follow-up were highly uniform throughout the entire study period. Second, the patients who were considered as advanced stage DTC using the previous TNM staging system were likely to have received more aggressive treatment. Therefore, there is a possibility of potential bias, which might have led to a better DSS in such patients. In spite of these limitations, this study is based on a large cohort of DTC patients with a relatively long follow-up, and thus it has valuable implications in evaluating the efficacy and prognostic validity of DSS of TNM-8 compared to TNM-7.
This study provides a clinical validation of the new AJCC/UICC TNM staging system for DTC. Applying TNM-8 did result in the downstaging of 38% of patients with DTC compared to TNM-7 in the patient cohort. TNM-8 had relatively better predictability for DSS than TNM-7 when PVE and Harrell's c-index were evaluated between the two staging systems. Taken together, these findings suggest that the changes brought forth in TNM-8 have improved the clinical usefulness of the TNM staging system in terms of predicting mortality and determining proper treatment intensity for patients with DTC.
Footnotes
Acknowledgments
This study was supported by a grant (no. 2017-598) from the Asan Institute for Life Sciences, Asan Medical Center, Seoul, Korea.
Author Disclosure Statement
No authors have any conflicts of interest in relation to this manuscript.