
Abstract
Background:
In order to establish whether thyroglobulin autoantibodies (TgAb) influence the metabolic clearance of thyroglobulin (Tg) in humans, serum Tg and TgAb were correlated shortly after radioiodine (131I) treatment.
Methods:
Samples were collected from 30 consecutive patients undergoing 131I activity for Graves' hyperthyroidism at the time of treatment and every 15 days thereafter, up to 90 days. Tg and TgAb were measured by immunometric assays (functional sensitivities: 0.1 ng/mL and 8 IU/mL).
Results:
Tg was detectable in all patients at day 0. Tg concentrations rose from a mean of 33.2 ng/mL [confidence interval (CI) 17.8–61.0 ng/mL] at day 0 to a mean of 214.6 ng/mL [CI 116.9–393.4 ng/mL] at day 30 and then steadily decreased, reaching the lowest concentration at day 90 (M = 10.9 ng/mL [CI 5.5–20.9 ng/mL]). Compared to their levels at day 0 (M = 23.6 IU/mL [CI 10.5–52.9 IU/mL]), TgAb remained stable through day 15 and then gradually increased up to a mean of 116.6 IU/mL [CI 51.9–262.2 IU/mL] at day 90. Patients were then split into two groups according to their TgAb status at day 0: undetectable (<8 IU/mL; 9 patients) or detectable (≥8 IU/mL; 21 patients) TgAb. Compared to the other cohort, patients with detectable TgAb showed significantly lower Tg concentrations at day 0 (M = 20.3 ng/mL [CI 10.1–40.2 ng/mL] vs. M = 101.8 ng/mL [CI 36.6–279.8 ng/mL]), similar at day 15, lower levels at day 30 (M = 146.5 ng/mL [CI 74.3–287.8 ng/mL] vs. M = 514.8 ng/mL [CI 187.8–1407.9 ng/mL]), at day 45 (M = 87.5 ng/mL [CI 43.1–176.6 ng/mL] vs. M = 337.9 ng/mL [CI 120.1–947.0 ng/mL]), at day 60 (M = 61.6 ng/mL [CI 31.0–121.4 ng/mL] vs. M = 255.8 ng/mL [CI 79.0–823.8 ng/mL]), and at day 75 (M = 24.5 ng/mL [CI 11.9–49.2 ng/mL] vs. M = 249.5 ng/mL [CI 63.5–971.1 ng/mL]), and similar levels at day 90. Patients with detectable TgAb showed a lower (M = 182.5 ng/mL [CI 92.0–361.0 ng/mL] vs. M = 514.8 ng/mL [CI 187.8–1407.9 ng/mL]) and an earlier (day 15 vs. day 30) peak of Tg. The mean Tg concentration was lower in patients with detectable TgAb than in those with undetectable TgAb (area under the curve: 17,340 ± 16,481 ng/mL vs. 36,883 ± 44,625 ng/mL; p = 0.02).
Conclusions:
TgAb influence the changes in Tg concentrations observed immediately after 131I treatment, inducing lower levels and an earlier peak of Tg. These observations indicate that TgAb significantly influence the metabolic clearance of Tg, supporting the concept that their interference in the measurement of Tg is mainly due to an in vivo effect.
Introduction
S
To establish whether TgAb influence Tg metabolic clearance in humans, serum Tg and TgAb were correlated shortly after radioiodine (131I) treatment for Graves' hyperthyroidism. 131I damages thyroid cells and releases Tg from thyroid follicles, causing a transient rise in serum Tg (11 –14).
Materials and Methods
Study group
After obtaining signed informed consent, sera samples were collected from 30 consecutive patients undergoing treatment with 131I (555 MBq) because of Graves' hyperthyroidism at the Endocrinology Unit, University Hospital of Pisa, Italy, between February 2013 and September 2013. The Institutional Review Board of the Endocrinology Unit approved the study. All patients had been treated with methimazole, which was discontinued five to seven days before 131I treatment. Samples were collected at the time of 131I treatment (day 0; 30 patients) and at 15 days (25 patients), 30 days (28 patients), 45 days (24 patients), 60 days (24 patients), 75 days (21 patients), and 90 days (27 patients) afterwards. Free thyroxine (fT4), free triiodothyronine (fT3), thyrotropin (TSH), Tg, TgAb, thyroperoxidase autoantibodies (TPOAb), and TSH-receptor autoantibodies (TRAb) were determined at all time points. Thyroid ultrasound was performed at day 0, day 30, day 60, and day 90. Treatment with methimazole was restarted in patients showing persistent thyrotoxicosis, while treatment with levothyroxine (LT4) was initiated when patients became hypothyroid. Although they had mild Graves' ophthalmopathy, all patients were treated with oral prednisone (20–30 mg/daily; 0.4–0.5 mg/kg body weight daily, which was then tapered and discontinued within three months) to prevent the possible exacerbation of the eye condition.
Serum assays
fT4 and fT3 were measured by fT4 and fT3 reagent packs (Ortho-Clinical Diagnostics, Inc., Rochester, NY; reference range 7.0–17.0 pg/mL and 2.7–5.7 pg/mL, respectively). TSH was determined using Immulite 2000 (Euro/DPC, Gwynedd, United Kingdom; reference range 0.4–3.6 μIU/mL). Tg was measured by an IMA (Access Thyroglobulin assay; Beckman Coulter, Inc., Fullerton CA; functional sensitivity 0.1 ng/mL). TgAb were measured using AIA-Pack 2000 TgAb (functional sensitivity 8 IU/mL; positive cutoff 30 IU/mL), and TPOAb were measured using AIA-Pack 2000 TPOAb (analytical sensitivity 3 IU/mL; positive cutoff 10 IU/mL), both by Tosoh Corporation (Tokyo, Japan). TRAb were measured using the Brahms TRAk human RIA assay (Hennigsdorf, Germany; analytical sensitivity 1 IU/mL; cutoff 1.5 IU/mL).
Neck ultrasound
Neck ultrasound was performed using a Technos (Esaote Biomedica, Genova, Italy) ultrasound with a 7.5 MHz linear transducer. The volume of each thyroid lobe was calculated with the ellipsoid formula: width (mm) × length × thickness × 0.52 (mL).
Statistical analysis
Descriptive data are presented as median and interquartile range (IQR; 25th–75th percentiles). Repeated-measures mixed models were used to analyze the time courses of Tg and TgAb levels over time using an autoregressive covariance structure (i.e., AR). Prior to analysis, both Tg and TgAb were log transformed to approximate a normal distribution, and results are reported as geometrical means with confidence intervals (CI). The Spearman's correlation coefficient (ρ) was employed to assess the association between Tg and TgAb at each time point. Statistical significance was considered for p-values <0.05.
Results
Changes in concentrations of thyroid hormones and TSH, levels of TPOAb and TRAb, and thyroid volume
Table 1 shows the changes in the concentrations of fT4, fT3, and TSH, the levels of TPOAb and TRAb, and the thyroid volumes after 131I treatment. At the end of the study, 21 patients were being treated with LT4 because of hypothyroidism, while three patients required treatment with methimazole because of transient thyrotoxicosis during the study. The levels of TPOAb and TRAb progressively rose, while the thyroid volumes gradually decreased after 131I treatment.
Data at the time of 131I treatment (day 0; 30 patients); follow-up at 15 days (25 patients), 30 days (28 patients), 45 days (24 patients), 60 days (24 patients), 75 days (21 patients), and 90 days (27 patients) is reported.
No patient received levothyroxine or methimazole at day 0 and day 15. One patient was taking LT4 at day 30, one patient was taking methimazole and three patients were taking LT4 at day 45, three patients were on methimazole and nine patients on LT4 at day 60, two patients were treated with methimazole and 18 patients with LT4 at day 75, and 21 patients were on LT4 at day 90.
TSH, thyrotropin; TPOAb, thyroperoxidase autoantibodies; TRAb, TSH-receptor autoantibodies; 131I, radioiodine; GD, Graves' disease; fT4, free thyroxine; fT3, free triiodothyronine; LT4, levothyroxine.
Changes in Tg concentrations and TgAb levels
Tg was detectable in all patients at day 0. The concentrations of Tg rose from a mean of 33.2 ng/mL [CI 17.8–61.0 ng/mL] at day 0 to a mean of 214.6 ng/mL [CI 116.9–393.4 ng/mL] at day 30 and then steadily decreased, and they were substantially lower (M = 10.9 ng/mL [CI 5.5–20.9 ng/mL]) at day 90 than at day 0 (Fig. 1).
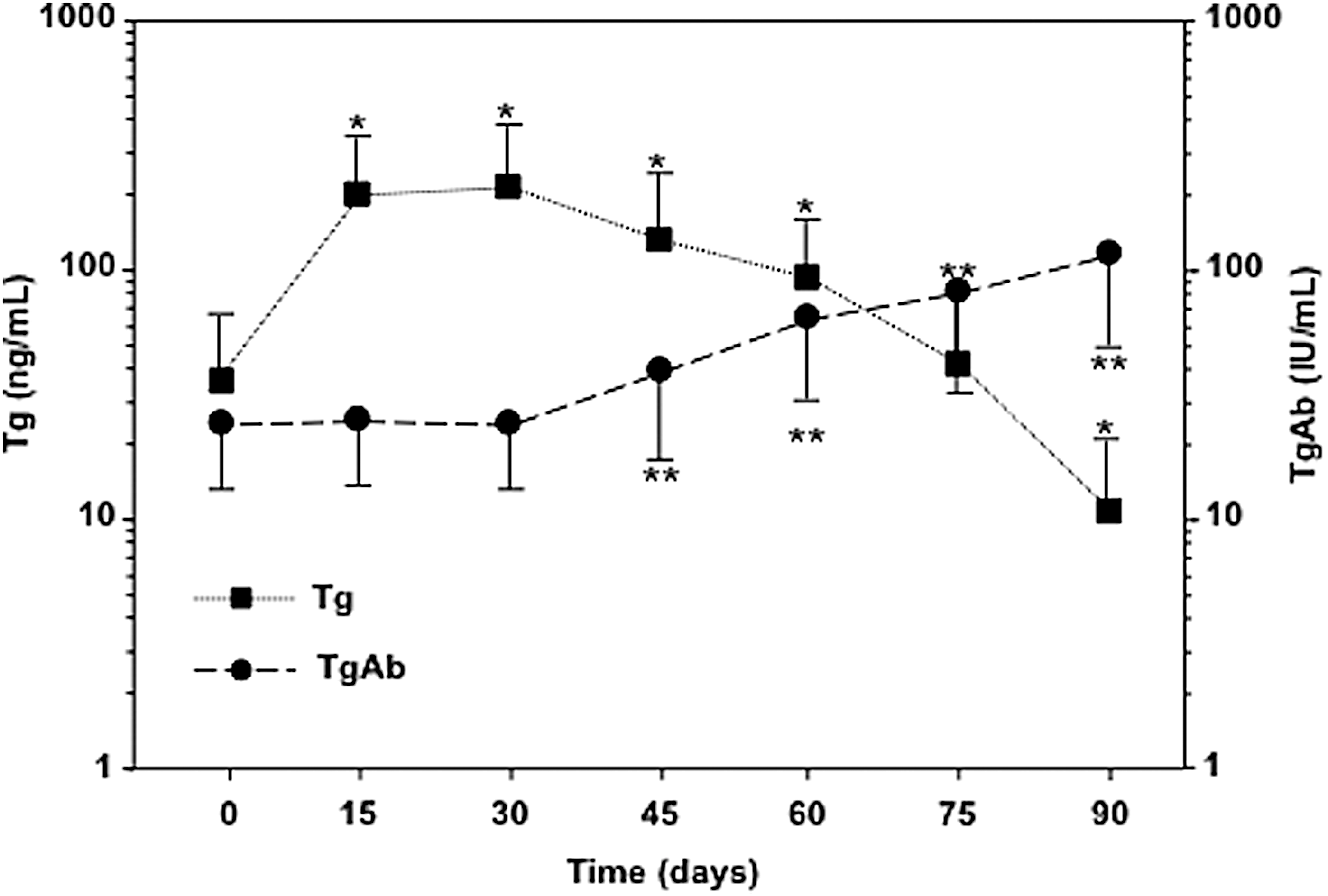
Changes in thyroglobulin (Tg) concentrations and thyroglobulin autoantibodies (TgAb) levels in patients with Graves' hyperthyroidism after radioiodine (131I) treatment. Day 0: 30 patients; day 15: 25 patients; day 30: 28 patients; day 45: 24 patients; day 60: 24 patients; day 75: 21 patients; day 90: 27 patients. *p < 0.05 versus Tg concentrations at day 0 (p < 0.001 at days 15, 30, and 45; p = 0.001 at days 60 and 90). **p < 0.05 versus TgAb levels at day 0 (p = 0.02 at day 45; p < 0.001 at days 60, 75, and 90). Geometric means with confidence intervals (CI) are shown.
Compared to their levels at day 0 (M = 23.6 IU/mL [CI 10.5–52.9 IU/mL]), TgAb remained stable through day 30 (M = 24.1 IU/mL [CI 10.8–54.1 IU/mL]) and then gradually increased up to a mean of 116.6 IU/mL [CI 51.9–262.2 IU/mL) at day 90 (Fig. 1).
Correlation between Tg concentrations and TgAb levels
A significant inverse correlation was observed between TgAb levels and Tg concentrations at all time points, except at day 15 (Fig. 2).
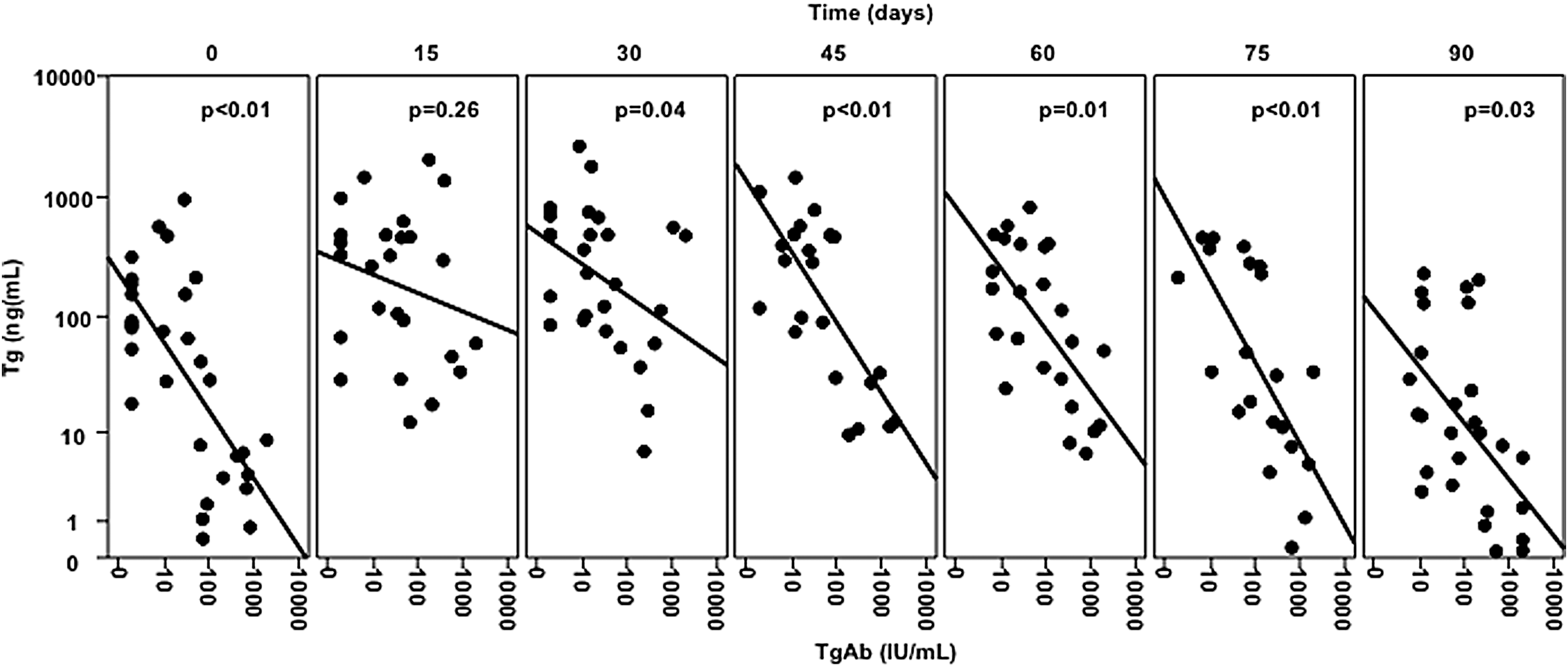
Correlations between TgAb levels and Tg concentrations in patients with Graves' hyperthyroidism after 131I treatment. Day 0: 30 patients; day 15: 25 patients; day 30: 28 patients; day 45: 24 patients; day 60: 24 patients; day 75: 21 patients; day 90: 27 patients.
Changes in Tg concentration according to the initial TgAb level
Patients were split into two groups according to their TgAb status at day 0: undetectable (<8 IU/mL; 9 patients) or detectable (≥8 IU/mL; 21 patients). Thyroid volume at day 0 was similar in the two groups: 16.0 ± 8.0 mL (median ± IQR) in patients with undetectable TgAb versus 19 ± 9.8 mL in patients with detectable TgAb (p = 0.47). Neither age nor thyroid function influenced Tg levels in patients with undetectable TgAb.
Compared to those with undetectable TgAb, patients with detectable TgAb showed significantly lower Tg concentrations at day 0 (M = 20.3 ng/mL [CI 10.1–40.2 ng/mL] vs. M = 101.8 ng/mL [CI 36.6–279.8 ng/mL]), similar levels at day 15 (M = 182.5 ng/mL [CI 92.0–361.0 ng/mL] vs. 247.5 ng/mL [CI 85.3–714.6 ng/mL]), lower levels at day 30 (M = 146.5 ng/mL [CI 74.3–287.8 ng/mL] vs. 514.8 ng/mL [CI 187.8–1407.9 ng/mL]), at day 45 (M = 87.5 ng/mL [CI 43.1–176.6 ng/mL] vs. 337.9 ng/mL [CI 120.1–947.0 ng/mL]), at day 60 (M = 61.6 ng/mL [CI 31.0–121.4 ng/mL] vs. 255.8 ng/mL [CI 79.0–823.8 ng/mL]), and at day 75 (M = 24.5 ng/mL [CI 11.9–49.2 ng/mL] vs. 249.5 ng/mL [CI 63.5–971.1 ng/mL]), and similar levels at day 90 (M = 7.3 ng/mL [CI 3.2–15.4 ng/mL] vs. M = 26.7 [CI 9.1–74.6 ng/mL]; Fig. 3). Compared to patients with undetectable TgAb, patients with detectable TgAb showed a lower (M = 182.5 ng/mL [CI 92.0–361.0 ng/mL] vs. M = 514.8 ng/mL [CI 187.8–1407.9 ng/mL]) and earlier peak (day 15 vs. day 30) of Tg. In both groups, the lowest Tg concentrations were observed at day 90 (M = 7.3 ng/mL [CI 3.2–15.4 ng/mL] and 26.7 ng/mL [CI 9.1–74.6 ng/mL]).
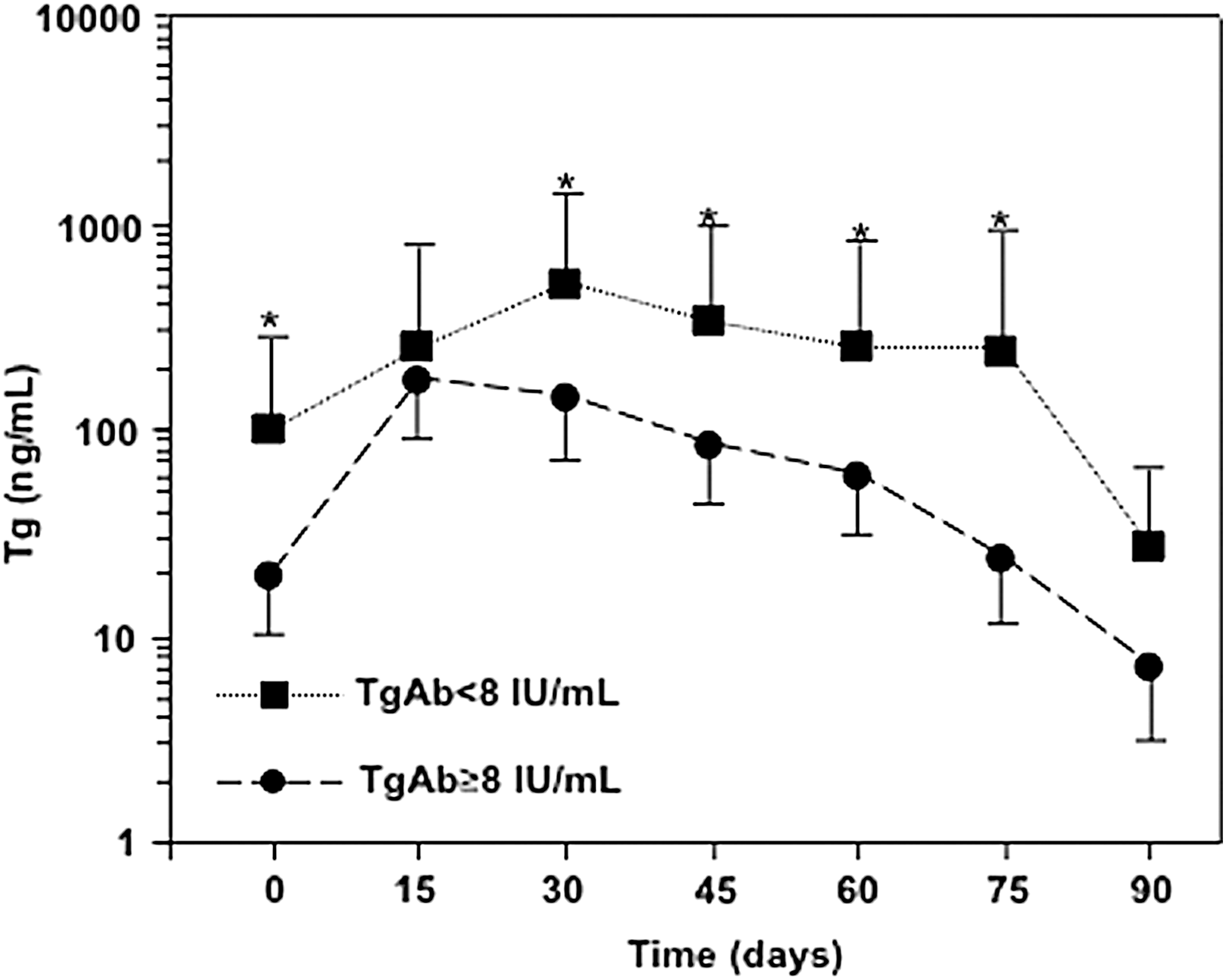
Changes in Tg concentrations in patients with Graves' hyperthyroidism after 131I treatment according to initial TgAb status: undetectable (<8 IU/mL; 9 patients) or detectable (≥8 IU/mL; 21 patients). *p < 0.05 between the two groups (p = 0.01 at day 0; p = 0.04 at days 30, 45, and 60; p = 0.003 at day 75). Geometric means with CI are shown.
The overall (from day 0 to day 90) Tg concentration was more than twice as high in patients with undetectable TgAb than in those with detectable TgAb (fold change = 2.82, p = 0.009 by mixed models; Fig. 4A and B). Accordingly, the mean 90-day area under the curve of Tg concentrations was higher in patients with undetectable TgAb (36,883 ± 44,625 ng/mL) than in patients with detectable TgAb (17,340 ± 16,481 ng/mL; p = 0.02; Fig. 4C).
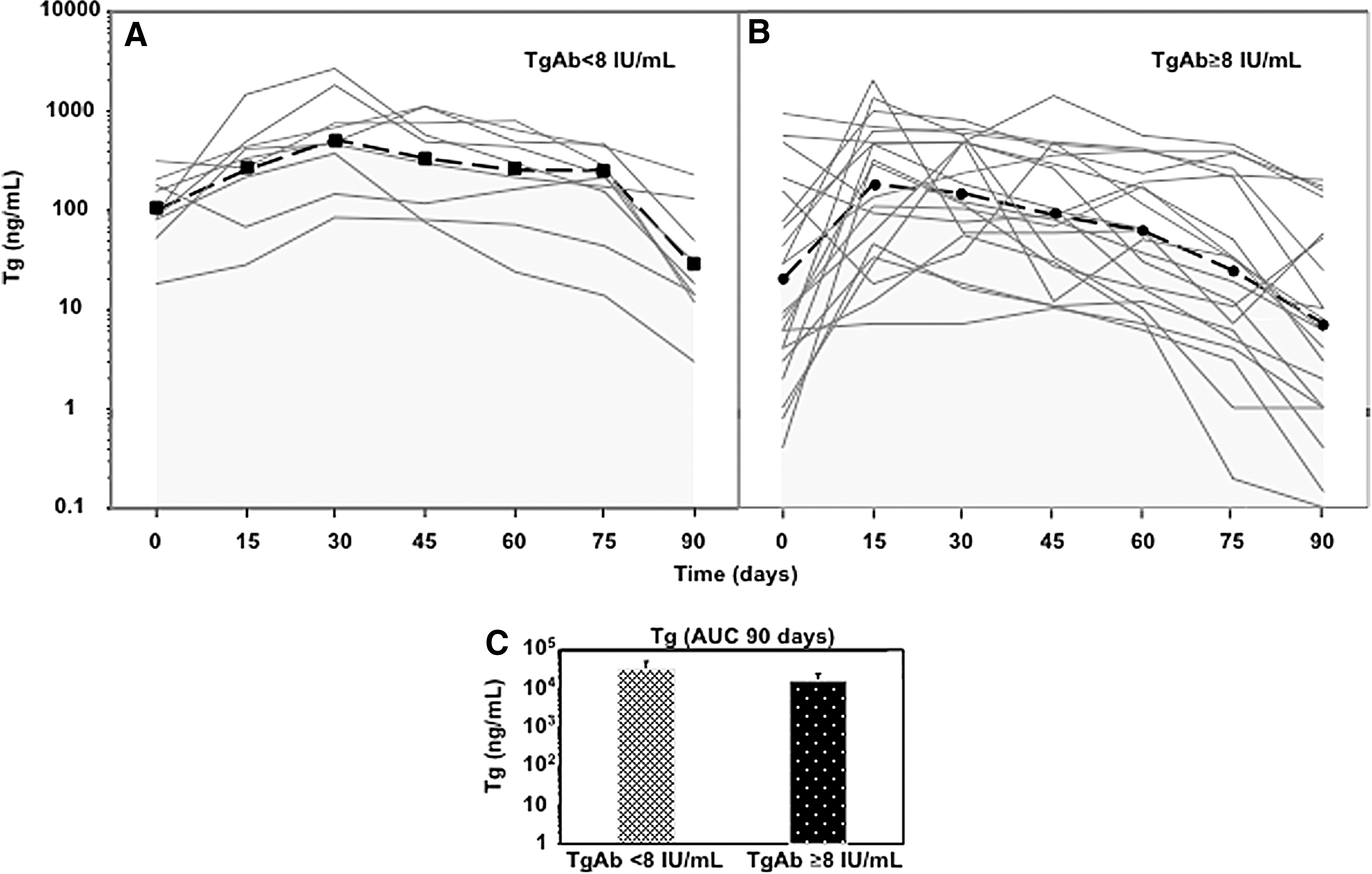
Individual and overall changes in Tg concentrations in patients with Graves' hyperthyroidism after 131I treatment according to initial TgAb status: (
Discussion
Tg is the specific marker of thyroid tissue, being produced by normal thyroid follicular cells and differentiated cancers originating from follicular cells. Along with ultrasound and imaging, follow-up of DTC patients consists in serial measurements of Tg (1). A major drawback in the measurement of Tg is interference from coexistent TgAb (6,15,16). TgAb are a marker of autoimmune thyroid diseases (17 –20), and 7.5–25% of DTC patients show positive TgAb (2-4) as expression of an associated autoimmune thyroid disease or an immune reaction to thyroid carcinoma (6,21,22). Tg concentrations and the heterogeneity of Tg and TgAb are factors contributing to the discordant results of Tg measurements in TgAb-positive patients (5 –7,9,23,24).
IMAs are the most sensitive methods for Tg measurement currently available (1,9). In the presence of TgAb, Tg values are lower than expected or even undetectable when measured by IMAs (5,6,24). These results are usually considered as falsely low Tg results. Tg radioimmunoassays, proposed as methods that are more resistant to TgAb interference, can yield falsely positive or falsely negative Tg results, depending on Tg concentrations and TgAb levels (5,6,8,9,25,26). The two other methods suggested in the past as resistant to TgAb interference, namely Tg recovery and Tg measurement by epitope-specific monoclonal TgAb, did not succeed in solving the problem (2,15). Tandem mass spectrometry, the latest methodology proposed, seems of limited efficacy as well (8,9,27). According to many recovery studies showing interference related to epitope masking (28), it has recently been confirmed that interference of TgAb in the measurement of Tg in vitro depends on both the Tg concentration and the TgAb levels (7). The relative contribution of in vitro (masking of epitopes) versus in vivo (TgAb-mediated Tg clearance) factors responsible for TgAb interference with Tg measurements may be variable and patient specific.
An accelerated metabolic clearance of Tg in TgAb-positive animals due to its greater elimination from the bloodstream was demonstrated in experimental autoimmune thyroiditis (10). Some indirect clinical evidence suggests that this phenomenon plays a role in humans as well (6,29).
Since 131I induces a rise in Tg (11 –14), Tg and TgAb concentrations were correlated in patients shortly after 131I treatment for Graves' hyperthyroidism in order to evaluate the influence of TgAb on the metabolic clearance of Tg in humans. After 131I therapy, both TPOAb and TRAb rose from day 60, while thyroid volumes decreased from day 30 onward. As an effect of the damage of thyroid cells and its release into the bloodstream, Tg rose, reaching a peak at day 30, and then it fell to reach its lowest concentration at day 90. TgAb remained stable through day 30 and then rose, peaking at day 90. Tg concentrations and TgAb levels were inversely correlated at almost all time points: the higher the TgAb values, the lower the Tg concentrations. The changes in Tg concentration were therefore specular to those in TgAb levels.
To evaluate the in vivo effect of TgAb better, the patients were then subdivided into two groups according to their initial TgAb status: undetectable or detectable. Although thyroid volume was similar in the two cohorts, at day 0, Tg concentrations were significantly lower in the group with detectable TgAb. At day 15, Tg levels rose to a higher degree in the group with undetectable TgAb, reaching concentrations that were comparable to the other group. At day 30, Tg concentrations continued to rise in the group with undetectable TgAb, while they started to decline in the group with detectable TgAb. The differences in Tg concentrations reflect two opposite events: the release into the bloodstream of Tg from the thyroid after 131I damage, and its enhanced metabolic clearance induced by TgAb. It is worth recalling that the levels of TgAb did not change up to day 30, and that day 15 was the only time point in which Tg concentrations and TgAb levels did not inversely correlate with each other. Consistent with the effect of TgAb on Tg clearance, from day 45 to day 75, Tg concentrations were higher in the group with undetectable TgAb than in the other group. Therefore, patients with detectable TgAb showed a lower and earlier peak and a lower mean concentration of Tg. At day 90, Tg levels were similar in the two groups because thyroid destruction by 131I was the predominant effect at this time point. Neither age nor thyroid function influenced Tg levels in patients with undetectable TgAb. However, these observations need to be confirmed in a larger study group.
The changes in Tg concentrations and TgAb levels that were observed are similar to the effects previously reported in a small cohort of patients evaluated for six months after 131I treatment for Graves' hyperthyroidism (13).
The half-life of Tg could not be calculated in this study because of the prolonged release of Tg into the bloodstream induced by 131I. The half-life of Tg has been estimated to range from 3.7 hours to 4.3 days in humans (30 –34). Clearance of Tg from the circulation varies with the state of glycosylation, asialo-Tg being cleared more rapidly from the circulation of rats (half-life of 6–40 minutes) than its sialylated counterpart (half-life of 5.1–15 hours) (35). Also, binding of bovine asialo-Tg to thyroid and liver membrane preparations has been documented (36), and it has been shown that clearance of Tg from the circulation by the liver occurs by endocytosis in macrophages (37).
It has recently been reported that the rise in TgAb immunoglobulin G (IgG) observed after 131I treatment for Graves' hyperthyroidism is restricted to IgG1 and IgG3 (29). IgG3 and, to a lesser extent, IgG1 are the strongest activators of the classical complement pathway. The C3b fragments released after complement activation interact with CR1 on erythrocytes to take the immune complexes out of the plasma. In the spleen and liver, the immune complexes are captured by complement and IgG receptors localized on the resident macrophage and dendritic cells. IgG1 and IgG3 show high-affinity binding to FcγRI and IgG3 to FcγRIIIA. FcγRI and FcγRIIIA are stimulatory receptors, expressed on monocytes/macrophages. FcγRI and FcγRIIIA are also expressed in dendritic cells and natural killer cells, respectively. IgG1 bind also to FcRn, which is expressed on monocytes/macrophages, neutrophils, and dendritic cells (38). Macrophages are the most efficient professional phagocytes and, when activated, internalize immune complexes. The rise in IgG1 and IgG3 levels seems to respond to the task of removing the large bulk of Tg released into the circulation after the thyroid damage induced by 131I.
The present findings, in addition to previous data, support the concept that in patients with TgAb, the lower than expected Tg concentrations observed when Tg is measured by IMA and tandem mass spectroscopy (2,6,8,9,27) is mainly due to a truly low Tg concentration. In spite of its active secretion by thyroid tissue, serum Tg is low or undetectable because it is removed at a faster rate from the circulation when TgAb coexist.
In conclusion, TgAb lessen the rise in Tg concentration that is induced by thyroid damage due to 131I treatment. This observation indicates that TgAb interference on Tg measurements is mainly due to its ability to remove Tg from the circulation, supporting the role of TgAb in the metabolic clearance of Tg. This consideration strongly supports the notion that the finding of undetectable Tg concentrations by IMA in DTC patients with coexistent TgAb is not due to mere analytical interference. It is foreseeable that any further attempt to overcome this limitation would prove unsuccessful.
Footnotes
Acknowledgments
These studies were supported by the grant “Rientro dei cervelli” n. 311 from MIUR and University of Pisa to F.L.
Author Disclosure Statement
The authors have nothing to disclose.