
Abstract

Although the marked effects of anti-programmed cell death (PD)-1 antibody in cancer treatment have created new possibilities in immunotherapy (1), this treatment can be complicated by the development of autoimmune disease in some patients, and the incidence of thyroid dysfunction has been estimated to be about 7% (1). However, the pathogenesis of autoimmune disease associated with the suppression of PD-1 function remains unclear. Recently, we managed a patient with Hashimoto's disease who showed changes in the percentage of follicular helper T cells (Tfh) (2,3), a helper T-cell subset that characteristically express PD-1 after anti-PD-1 antibody therapy. Such changes suggest the involvement of these cells in the development of anti-PD-1-induced autoimmune disease. We report here our findings.
The patient was a 63-year-old man who was started on nivolumab (a human IgG4 anti-PD-1 monoclonal antibody) for recurrent lung cancer. The patient was positive for antithyroid peroxidase (anti-TPO) antibodies (510 IU/mL; reference range <16 IU/mL) and antithyroglobulin (anti-Tg) antibodies (572 IU/mL; reference range <28 IU/mL) before the initiation of nivolumab therapy, but had normal thyroid function (thyrotropin [TSH]: 3.71 μIU/mL [range 0.34–6.50 μIU/mL]; free thyroxine [fT4]: 1.08 ng/dL [range 0.97–1.79 ng/dL]), and thyroid ultrasonography showed no abnormalities (Fig. 1A). Nivolumab therapy was discontinued after two doses due to inadequate response. Discontinuation of the treatment was followed by a change in autoantibody levels (anti-TPO antibody: 561 IU/mL; anti-Tg antibody: 2239 IU/mL) after two weeks, together with reduced internal echo intensity on thyroid ultrasonography (Fig. 1B). These changes were associated with further increases in autoantibody levels (anti-TPO antibody: >600 IU/mL; anti-Tg antibody: >4000 IU/mL) at three months after therapy. Repeat ultrasonography showed evidence of thyroid atrophy and hypoechogenicity (Fig. 1C). Due to marked hypothyroidism, as indicated by a TSH of 146 μIU/mL and a fT4 of 0.13 ng/dL, treatment with levothyroxine was initiated. Thereafter, the patient's condition progressed to permanent hypothyroidism, necessitating continuation of levothyroxine. TSH receptor antibody and thyroid-stimulating antibody were negative both before and after nivolumab therapy.
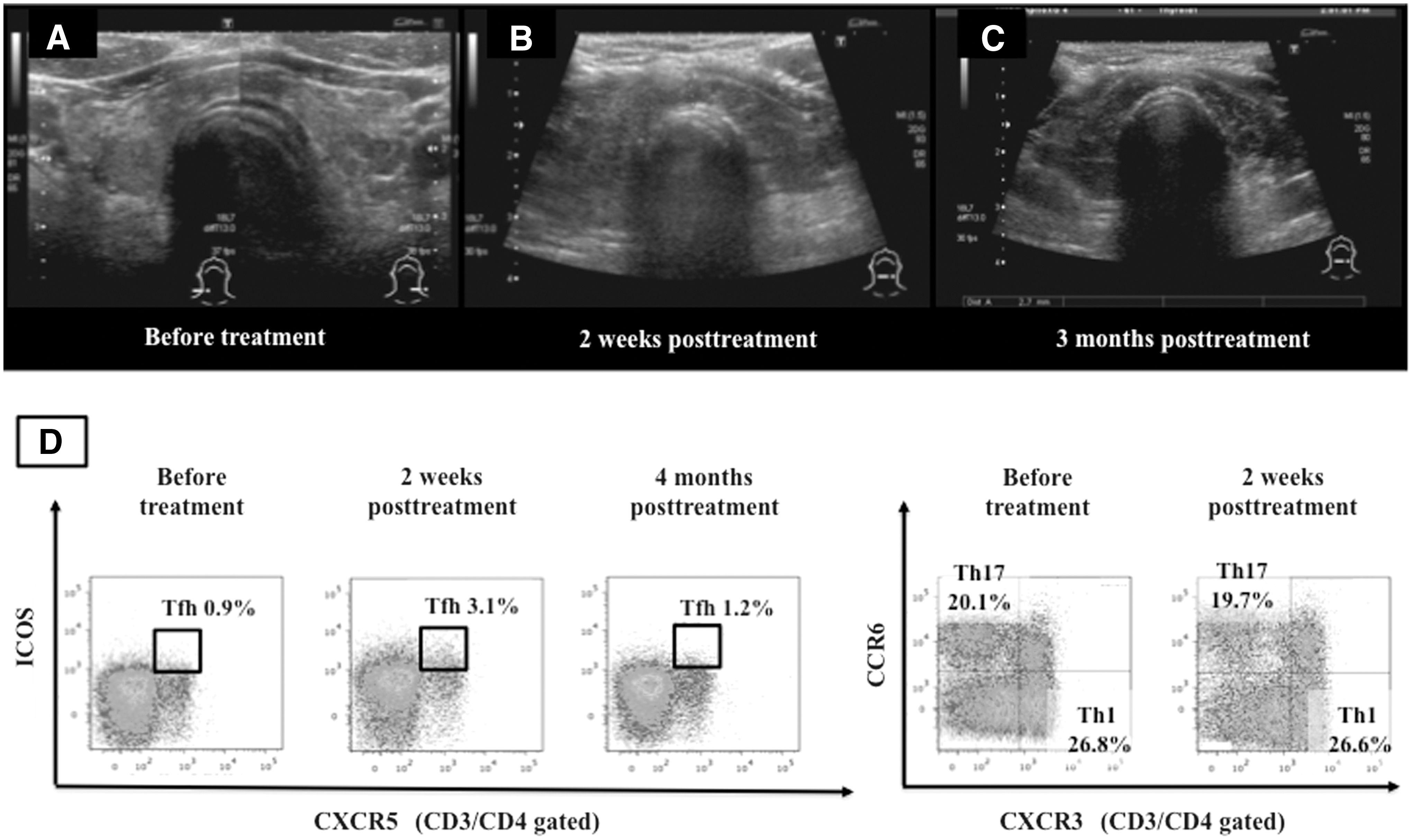
Thyroid sonography and results of flow cytometric analysis of peripheral blood mononuclear cells. Thyroid sonography before (
Flow cytometric analysis of peripheral blood lymphocytes showed similar proportions of Th1 cells (CD4+CXCR3+CXCR6−) and Th17 cells (CD4+CXCR3−CCR6+) at baseline and at two weeks after anti-PD-1 antibody therapy. In contrast, the proportion of Tfh cells (CD4+CXCR5+ICOShigh) increased markedly from 0.9% at baseline to 3.1% at two weeks after treatment (Fig. 1D). Furthermore, the proportion of Tfh cells continued to decrease (to 1.2%) at four months after treatment.
Tfh cells are helper T cells that express CXCR5 and ICOS, produce interleukin 21, and control the maturation and activation of B cells and production of antibodies. In general, PD-1 is highly expressed in Tfh cells, and these cells bind to programmed death ligand-1 (PD-L1) and PD-L2 on antigen-presenting cells, and are subject to inhibitory signals. Our patient showed an increased proportion of Tfh cells, as well as an overproduction of thyroid autoantibodies following nivolumab therapy. It is presumed that the latter therapy suppressed the PD-1/PD-L1 inhibitory signals in Tfh cells, facilitating the proliferation of Tfh cells and production of autoantibodies. To our knowledge, this is the first report describing an increase in the proportion of Tfh cells due to antibodies inhibiting PD-1 and PD-1 ligands as being involved in the mechanism underlying the development of autoimmune disease. Considered together with previous findings of increases in Tfh cells in the peripheral blood of patients with Hashimoto's disease (4), our report strongly suggests the involvement of Tfh cells in the development of Hashimoto's disease.
Footnotes
Author Disclosure Statement
All authors declare no conflict of interest in association with this report.