
Abstract
Background:
Iodine intake is associated with various thyroid diseases and serum thyrotropin (TSH) levels. The aim of this study was to investigate iodine intake and its impact on the distribution of serum TSH levels using nationwide data from Korea, a country known to be iodine replete.
Methods:
The sixth Korean National Health and Nutrition Examination Survey (2013–2015) is a nationwide, cross-sectional survey of the Korean general population. Participants were selected using two-stage stratified cluster sampling of the population and housing census data. A total of 6564 participants aged ≥10 years who underwent thyroid function tests and urinary iodine level measurements during the survey were included in this study.
Results:
The median urinary iodine concentration (UIC) was 299.3 μg/L (interquartile range 158.8–699.8), suggesting more than adequate iodine intake in Korea. With high-iodine intake in all age groups and in both females and males, the TSH reference interval in the Korean reference population was right-shifted at 0.62–6.84 mIU/L. The prevalence of overt and subclinical hypothyroidism in Korea according to this reference interval was 0.73% and 3.12%, respectively, and was significantly associated with nutritional iodine status (p = 0.011 and p < 0.001, respectively).
Conclusions:
This first nationwide survey demonstrates more than adequate iodine intake and a right-shifted distribution of serum TSH levels in the Korean general population. Nutritional iodine status is important for determining serum TSH levels and is associated with a high prevalence of hypothyroidism. Nutritional iodine status might need to be considered when establishing TSH reference intervals of populations in iodine-replete areas.
Introduction
I
Korea is a known to be an iodine-replete area with high seaweed consumption. The median urinary iodine concentration (UIC) in Korea ranges from 300 to 1000 μg/L according to previous studies (10 –12), which is considerably higher than the recommendation by the World Health Organization (WHO) (13) and also higher than most other countries (14,15). One recent study using routine health check-up data in Korea demonstrated that the serum thyrotropin (TSH) reference interval of the reference population ranged from 0.73 to 7.06 mIU/L and was higher than that of other countries (16). These right-shifted TSH levels might be associated with the excess iodine intake in the Korean population. However, the results of that study might be biased, and there have been no national epidemiologic data evaluating iodine intake and thyroid function in Korea.
The first nationwide survey for thyroid function and iodine intake was recently conducted in Korea. The sixth Korean National Health and Nutrition Examination Surveys (KNHANES) took place from 2013 to 2015 and measured serum TSH, free thyroxine (fT4), antithyroid peroxidase antibody (TPOAb) titers, and UICs in the Korean general population (17). This study aimed at investigating the iodine intake status and its impact on the TSH reference interval and thyroid dysfunction in the Korean population. These data might be helpful in demonstrating the impact of long-term excessive iodine intake on thyroid function.
Materials and Methods
Study cohort
The KNHANES is a nationwide, cross-sectional survey conducted by the Korea Centers for Disease Control and Prevention (KCDC) that used stratified, multistage clustered probability sampling to select a representative sample of the civilian, non-institutionalized Korean population. The KNHANES is an ongoing surveillance system that assesses the health and nutritional status of Koreans, and it provides data about the prevalence of major chronic diseases in Korea as far back as 1998.
In KNHANES VI (2013–2015), research participants were selected using two-stage stratified cluster sampling of the population and housing census data. Among them, about 2400 persons aged ≥10 years were selected for laboratory tests of thyroid function and UIC by stratified subsampling with consideration for sex and age in each year. Finally, a total of 6564 participants underwent thyroid function tests and UIC measurements in KNHANES VI (2013–2015).
The KNHANES obtained written informed consent from every participant prior to completing the survey, and secondary anonymized data were used for analysis. The study protocol was approved by the Institutional Review Board of the Asan Medical Center, Seoul, Korea.
Measurement of TSH, fT4, TPOAb, and UIC
For analysis of serum TSH, fT4, and TPOAb, approximately 15 mL of blood was collected from each participant. After separation of the serum within 30 min, the samples were then transferred and analyzed within 24 h.
Serum TSH, fT4, and TPOAb levels were measured with an electrochemiluminescence immunoassay (Roche Diagnostics, Mannheim, Germany). Briefly, TSH was measured with an E-TSH kit (Roche Diagnostics), and the reference range in the manual was 0.35–5.50 mIU/L. Serum fT4 was measured using an E-Free T4 kit (Roche Diagnostics), and the reference range was 0.89–1.76 ng/mL. TPOAb were measured with an E-Anti-TPO (Roche Diagnostics), and the reference range for TPOAb in humans is <34.0 IU/mL. The measurements of TSH, fT4, and TPOAb met the criteria of the College of American Pathologists. UICs were measured by an inductively coupled plasma mass spectrometry (ICP-MS; PerkinElmer, Waltham, MA) using an iodine standard (Inorganic Venture, Christiansburg, VA) (17).
Definitions
Participants were classified into six groups according to UIC, which is a well-established indicator of iodine intake. Participants with a UIC ≥1000 μg/L were defined as having extremely excessive iodine intake, 300–999 μg/L as moderately excessive iodine intake, 200–299 μg/L as more than adequate iodine intake, 100–199 μg/L as adequate iodine intake, 50–99 μg/L as mildly deficient iodine intake, and <50 μg/ as moderately to severely deficient iodine intake. This classification is mainly adopted from the WHO recommendation, (13) and the excessive iodine intake group was subdivided into two groups: extremely excessive and moderately excessive iodine intake.
The disease-free population was defined as participants with no prior history of thyroid disease or thyroid cancer and no history of taking medicines that could influence thyroid function. The reference population was selected from the disease-free population as participants who were not pregnant, had no family history of thyroid disease, tested negative for TPOAb, and had serum fT4 levels within the reference range (0.89–1.76 ng/dL). Because a health interview regarding the history of thyroid disease was not conducted in participants aged 10–18 years, it was assumed that those young participants did not have any prior history of thyroid disease. The definitions of the disease-free and reference populations were adopted from a previous study that analyzed thyroid functions in the U.S. population using the National Health and Nutrition Examination Survey (NHANES) III (18). The definition of the reference population was also in accordance with the National Academy of Clinical Biochemistry (NACB) guidelines (19). The TSH reference interval was determined as the 2.5th–97.5th percentiles of the serum TSH levels of the reference population.
Thyroid dysfunction, including hypothyroidism and hyperthyroidism, were defined as follows. Subclinical hypothyroidism was defined as high serum TSH levels >97.5th percentile of serum TSH levels with normal fT4 levels. Overt hypothyroidism was defined as high serum TSH levels >97.5th percentile of serum TSH levels with low fT4 levels (<0.89 ng/dL). Subclinical hyperthyroidism was defined as low serum TSH levels <2.5th percentile of serum TSH levels with normal fT4 levels. Overt hyperthyroidism was defined as low serum TSH levels <2.5th percentile of serum TSH levels with high fT4 levels (>1.76 ng/dL). The prevalence of hypothyroidism and hyperthyroidism was evaluated by using the reference intervals of serum TSH obtained from this study and the reference interval in the manual of the kit (Roche Diagnostics).
Statistics
R program v3.2.1, R studio v0.98.1091, and the R libraries survey and Cairo (R Foundation for Statistical Computing;
Results
Baseline characteristics of the participants
The baseline characteristics of the 6564 participants included in this study are shown in Supplementary Table S1 (Supplementary Data are available online at
Weighted UICs of the Korean population
Weighted UICs were assessed according to the age and sex of subjects. The median UIC was 299.3 μg/L (IQR 158.8–699.8 μg/L) after weighting sample values. UICs were constantly high in all age groups, and no definite trend changes according to the age group were observed, but the median UICs were significantly different according to the age group (p = 0.035). Participants >70 years had the highest UICs (median 442.5 μg/L), and the youngest age group (aged 10–18 years) also had high UICs (median 432.2 μg/L; Fig. 1). The median UIC was not different between males and females (p = 0.96). Furthermore, UIC was not different according to body mass index, smoking status, or socioeconomic status (p = 0.06, p = 0.82, and p = 0.36, respectively).
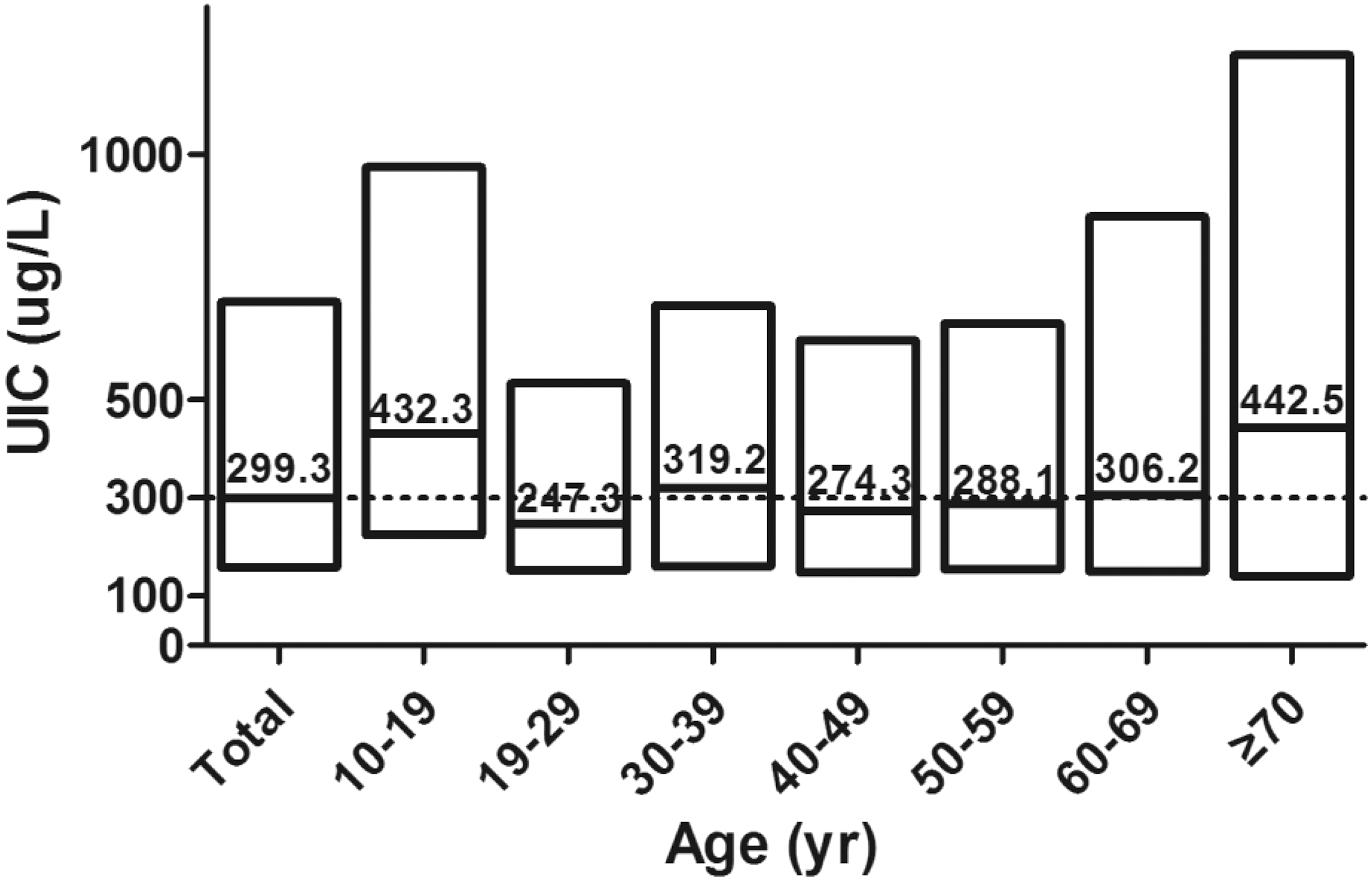
Urinary iodine concentrations (UIC) according to age. The box plot present the interquartile ranges of UIC. The value and the line in the box plot present the median UIC in each group. The median UIC in the total population was 299.3 μg/L.
Weighted serum TSH and fT4 levels according to UICs
Serum TSH and fT4 levels were assessed according to UIC (six categories) in the total, disease-free, and reference populations (Table 1 and Supplementary Table S2). With the increase of UICs, serum TSH levels tended to increase and serum fT4 levels tended to decrease. This trend was statistically significant in the total, disease-free, and reference populations (p < 0.001, p < 0.001, and p < 0.001, respectively). In the reference population, the median serum TSH level was 2.23 mIU/L, and the TSH reference interval was between 0.62 and 6.84 mIU/L. The median fT4 level of the reference population was 1.24 ng/dL. When the reference population was subclassified according to UIC, the median and 97.5th percentile of the serum TSH levels were the highest in the extremely excessive iodine intake group at 2.47 mIU/L and 8.83 mIU/L, respectively. In the moderately to severely deficient iodine intake group, the median and 97.5th percentile of the serum TSH levels were the lowest at 1.95 mIU/L and 4.85 mIU/L, respectively. The distribution of serum TSH levels according to UIC is also shown in Figure 2. Serum TSH levels were left-shifted in the iodine-deficient groups (Fig. 2A) and were right-shifted in the iodine-excessive groups (Fig. 2B) compared with those in the adequate iodine intake group.
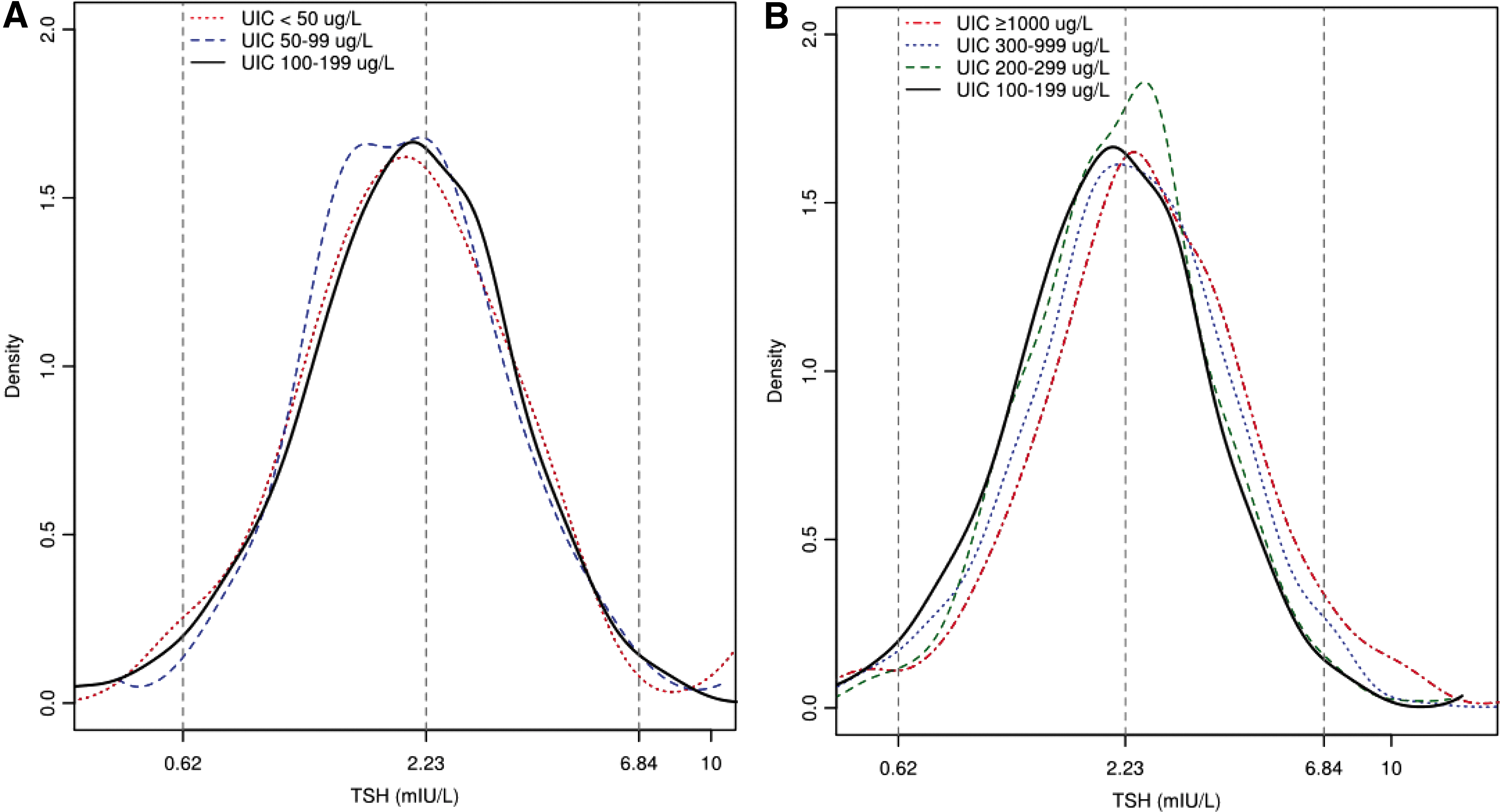
Distribution of serum thyrotropin (TSH) levels according to iodine nutrition status. (
TSH values are presented as medians (2.5th–97.5th percentile range [mIU/L]). fT4 values are presented as medians (2.5th–97.5th percentile range [ng/dL]). p-Values were estimated by linear regression analysis.
TSH, thyrotropin; fT4, free thyroxine; UIC, urinary iodine concentration.
Weighted prevalence of thyroid dysfunction according to UICs
The prevalence of thyroid dysfunction was assessed according to UICs in the Korean population. The reference interval of serum TSH in this study was between 0.62 and 6.84 mIU/L, whereas the TSH reference interval of the kit was between 0.35 and 5.50 mIU/L. According to the reference interval, the prevalence of overt and subclinical hypothyroidism was 0.73% and 3.12 %, respectively (Table 2). The prevalence of overt and subclinical hypothyroidism was significantly increased by the increase of UIC (p = 0.011 and p < 0.001, respectively). The prevalence of overt and subclinical hypothyroidism was highest in the extremely excessive iodine intake group at 1.78% and 5.50%, respectively (Fig. 3). The prevalence of overt and subclinical hyperthyroidism was 0.56% and 2.96%, respectively. The prevalence of overt and subclinical hyperthyroidism did not differ according to UIC (p = 0.30 and p = 0.63, respectively).
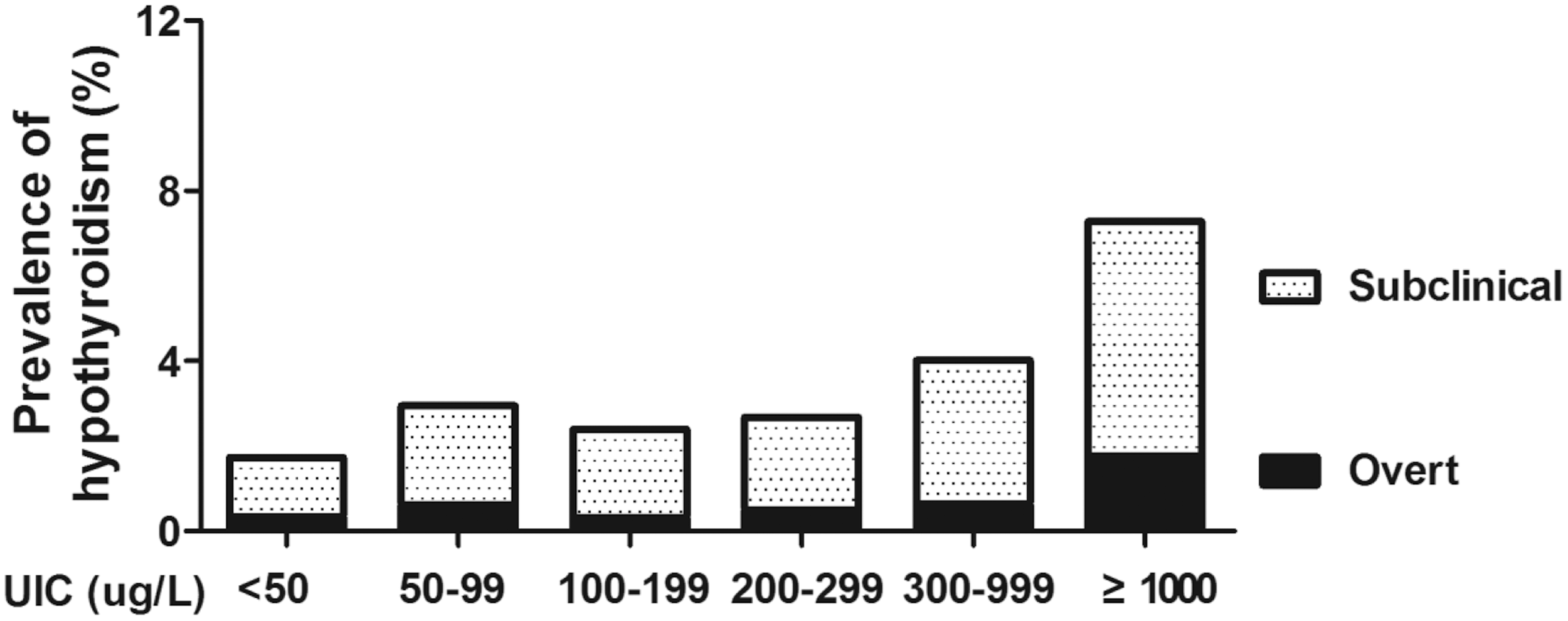
Prevalence of hypothyroidism in the Korean population according to iodine nutrition status. Nutritional iodine status was classified into six groups: moderately to severely deficient iodine intake (UIC <50 μg/L), mildly deficient iodine intake (UIC 50–99 μg/L), adequate iodine intake (UIC 100–199 μg/L), more than adequate iodine intake (UIC 100–299 μg/L), moderately excessive iodine intake (UIC 300–999 μg/L), and extremely excessive iodine intake (≥1000 μg/L). The reference interval of serum TSH was between 0.62 and 6.84 mIU/L in this study.
Data shown represent the prevalence. p-Values were estimated by chi-square test.
When the reference interval of serum TSH established by the manufacturer of the kit was applied, the prevalence of overt hypothyroidism was 0.77%, and the prevalence of subclinical hypothyroidism was 5.79% (Supplementary Table S3). The prevalence of overt and subclinical hypothyroidism also significantly increased with the increase in UIC (p = 0.015 and p < 0.001, respectively) and was the highest in the extremely excessive iodine intake group.
Discussion
This is the first nationwide study to evaluate the nutritional iodine status of Koreans in association with thyroid function. The median UIC was 299.3 μg/L in the Korean general population, which is higher than that of other countries (4,15). A high UIC in all age groups suggests a lifelong high-iodine intake in Koreans.
With the high-iodine intake, the distribution of serum TSH levels in Korea was significantly right-shifted compared to that in other countries, and the TSH reference interval was between 0.62 and 6.84 mIU/L (1,7,18). The prevalence of overt and subclinical hypothyroidism, irrespective of the TSH reference interval, was significantly associated with the nutritional iodine status and was the highest in the extremely excessive iodine intake group (2,8). The prevalence of subclinical hypothyroidism decreased using the reference interval of serum TSH compared to the reference interval of the kit. This disparity in the prevalence of subclinical hypothyroidism was most pronounced in the extremely excessive iodine intake group. A previous cohort study from Korea reported that the prevalence of subclinical hypothyroidism in Korea was high at 11.7% (20). On the contrary, after using the Korean TSH reference interval in this study, the prevalence of subclinical hypothyroidism in Korea was not different from other countries (2,18,21,22).
The findings confirm that nutritional iodine status is an important factor in determining the prevalence of thyroid disease and the TSH reference interval of a population. These data also suggest that the nutritional iodine status needs to be considered when establishing TSH reference intervals of populations in iodine-replete areas. The NACB criteria only recommend considering the presence of personal or family history of thyroid dysfunctions, goiter, medications associated with thyroid function, or thyroid autoantibodies when establishing TSH reference intervals in a population (19). One previous study suggested the use of age, sex, and race/ethnicity-specific TSH reference intervals (23). Another possible approach may be to exclude participants with excessive iodine intake, especially with extremely excessive iodine intake, when establishing TSH reference intervals of a population. Furthermore, the regular monitoring of the nutritional iodine status of a population is needed, and iodine intake should be maintained at an adequate level because excessive iodine intake may lead to an increase in hypothyroidism in a population.
The iodine intake status assessed by UIC confirmed the more than adequate to excessive iodine intake in all age groups in Korea. Teenagers and participants aged ≥70 years had a higher prevalence of excessive iodine intake compared to other age groups. The reason for this phenomenon could not be determined. A previous study reported that the major source of dietary iodine in Korea was seaweed, which contributes about 66% of the iodine intake (24). Koreans traditionally use sea tangle or kelp as a basic ingredient in soup and frequently consume brown seaweed soup and laver (10,12). The dietary habits of teenagers and older adults may be most affected by the traditional cultural habits of high-iodine intake compared to other age groups.
When the present results were directly compared with the NHANES III study, some similar findings were found between the two studies (18). The TSH levels of the reference population were lower than those of the total or disease-free population. Even though the previous study from NHANES III used urinary iodine to creatinine ratio as a marker of iodine nutrition, it also reported that the TSH level was not a sensitive indicator of iodine deficiency.
This study has limitations. Because of its cross-sectional study design, a cause-and-effect relationship could not be confirmed. Furthermore, urinary iodine levels vary daily and only reflect recent changes in iodine status (13). This study focused on the nutritional iodine status and did not evaluate the effect of age and sex on thyroid function. However, nutritional iodine status did not present any trend changes according to age and sex, and their confounding effect might be minimal. Because thorough thyroid exams done by clinicians were not conducted in this survey, it was not possible to assess whether participants in this study had a goiter. As a result, the TSH reference intervals in this study might not meet the criteria of the NACB (19). Moreover, the study did not assess the iodine intake of pregnant women due to a lack of data. However, the study is of value because it is based on nationwide data representative of the Korean population and could thus be generalized to the Korean population.
In conclusion, the first nationwide survey in Korea revealed a high-iodine intake (median UIC 299.3 μg/L) and a right-shifted distribution of serum TSH levels in the Korean general population. The TSH reference interval in this study was between 0.62 and 6.84 mIU/L. Nutritional iodine status appears to be an important factor for determining serum TSH levels, and it is associated with a high prevalence of hypothyroidism. The findings suggest that the nutritional iodine status should be considered when establishing TSH reference intervals of populations in iodine-replete areas.
Footnotes
Acknowledgments
This study was supported by a grant (No. 2017-298) from the Asan Institute for Life Sciences, Asan Medical Center, Seoul, Korea.
Author Disclosure Statement
The authors have nothing to disclose.