
Abstract
Background:
The association between Graves' disease (GD) and thymic hyperplasia (TH) was first described in 1912 and has been reported numerous times thereafter. TH associated with GD presents as an incidental mediastinal mass on chest X-ray or computed tomography (CT). The pathogenesis of TH in the setting of GD is unclear but seems to involve a complex interplay of hormonal and immunological mechanisms.
Summary:
Here, the effect that thyroid hormones and autoimmunity have on thymic growth and size is reviewed. The authors' experience, along with a review of published case reports, reveals that general physicians may be unfamiliar with this association. This lack of familiarity may result in an aggressive management course, including surgical intervention, along with its associated risks and costs. The differential diagnosis and diagnostic workup of thymic enlargement associated with GD is discussed in light of the available clinical evidence.
Conclusion:
Recent literature confirms the generally benign nature of TH associated with GD, and supports a conservative approach for the diagnostic workup and initial management. Practical management recommendations for thymic enlargement associated with GD have been formulated and are presented here.
Introduction
G
GD and other autoimmune thyroid diseases are thought to result from a loss of self-tolerance, leading to the generation of auto-reactive T cells and immunoglobulins directed against autoantigens. In GD, in addition to the TSH-R, other thyroidal antigenic targets include thyroid peroxidase, thyroglobulin (3), insulin-like growth factor 1 receptor (4), and others (5 –7). The production of anti-TSH-R antibodies by B lymphocytes is likely the result of a T-cell-mediated immune response. T-cell maturation and self-tolerance occur in the thymus. Self-tolerance is known to be impaired in patients with autoimmune diseases (8).
While well documented in the literature and well known to thyroidologists, the association between GD and thymic hyperplasia (TH) remains largely unrecognized in routine clinical practice, per the authors' review. It is hypothesized that this is likely the result of appropriately limited thoracic radiological evaluations for most patients with GD, as well as a lack of awareness of this association among general physicians. Here, an illustrative case of TH associated with GD is presented. The available literature is also reviewed regarding its pathophysiology, and evidence is provided to support a conservative approach to the management of these patients.
Search Strategy and Selection Criteria
Data for this review were identified by searches of PubMed and MEDLINE, using the search term “thymic hyperplasia,” “Graves' disease,” and “thymus and autoimmune disease.” Only articles published in English were included.
Illustrative Case
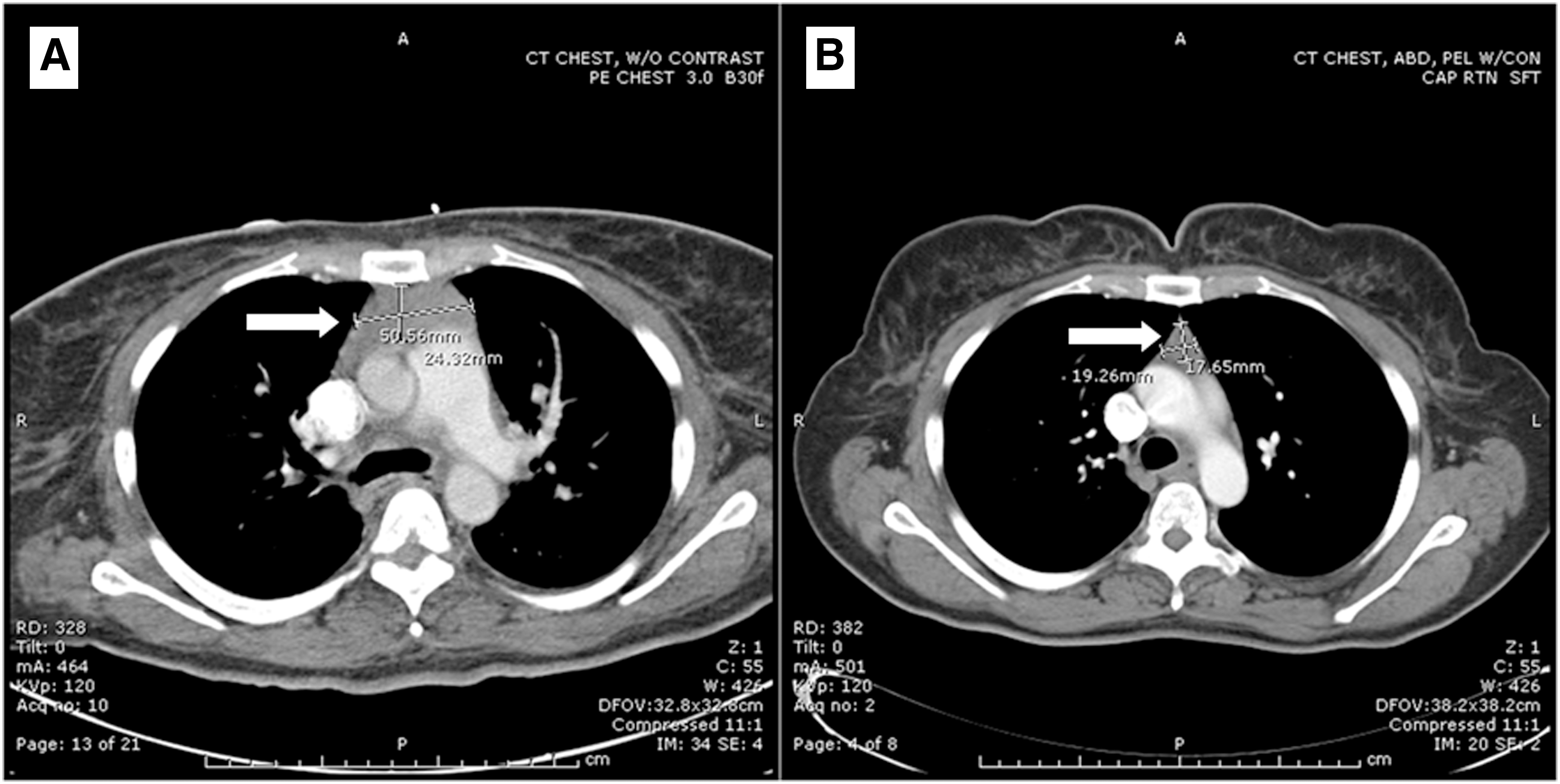
A 49-year-old female presented with progressive substernal chest pain of approximately one month duration, as well as a two-month history of dyspnea on exertion, palpitations, tremor, night sweats, and a 30 lb weight loss. On exam, the thyroid gland was diffusely enlarged to approximately twice its normal size, and thyroid function tests as well as thyroid-stimulating immunoglobulin (TSI) and radioactive iodine (RAI) uptake and scan were consistent with severe thyrotoxicosis due to GD. No signs or symptoms of GD-associated ophthalmopathy or dermopathy were noted. A computed tomography (CT) angiogram of the chest performed to evaluate the chest pain revealed a solid, homogenous, anterior mediastinal mass measuring 5.5 cm × 2.4 cm × 2.1 cm (Fig. 1A) with axillary, subcarinal, perivascular, pretracheal, and cardiophrenic adenopathy. The patient was admitted to the hospital and evaluated by a pulmonary and cardiothoracic surgeon who scheduled a diagnostic biopsy and possible excision of the mediastinal mass in order to exclude thymoma or lymphoma. The procedure was delayed at the request of the endocrine service, since TH associated with GD was anticipated to regress with treatment of GD, and the patient was discharged home on antithyroid drugs (ATD). The patient received RAI therapy for GD 13 weeks after initial presentation.
(
Six months after initial presentation the patient was biochemically and clinically euthyroid. A repeat CT scan of the chest, abdomen, and pelvis revealed a 1.9 cm × 1.7 cm × 1.3 cm soft-tissue anterior mediastinal density with normal concave mediastinal contour (Fig. 1B), which corresponds to an 85% volumetric regression. The mediastinal adenopathy had resolved. The patient was reevaluated in a multidisciplinary conference where the pulmonary and cardiothoracic surgery services concluded that given regression of the mass, surgical intervention will no longer be pursued.
Review
Diagnosis of TH
The thymus is a specialized organ of the immune system. Histologically, it can be divided into a central medulla and a peripheral cortex. Cells in the thymus can be divided into stromal cells (cortical and medullary epithelial and dendritic cells) and cells of hematopoietic origin (developing T cells). The cortical and medullary epithelial cells form a reticular network throughout the thymus. While epithelial cells are more abundant in the medulla compared to the cortex, overall, epithelial cells do not contribute significantly to thymic volume (9,10).
TH refers to gross, diffuse, and symmetric enlargement of the thymus and has been defined by weight (11 –13), size (14 –18), or pathologic criteria (13,19,20). Histologically, TH is divided into two subtypes (13): (i) true TH (TTH), which is microscopic hyperplasia of cortical and medullary parenchyma associated with a grossly enlarged thymus, and (ii) thymic lymphoid hyperplasia (TLH), which is characterized by increased formation of lymphoid follicles in the thymic medulla. The diagnosis of TLH is meaningful only when accompanied by clinical evidence of autoimmune disease. TLH is not limited to GD and is seen in other autoimmune diseases such as myasthenia gravis, progressive systemic sclerosis, rheumatoid arthritis, and systemic lupus erythematosus (SLE) (21 –25). Furthermore, TLH alone may not lead to gross thymic enlargement (13,16,19).
An appreciation of the microscopic features of TH is important. Although both TTH and TLH can co-exist in the same gland, it appears that each has a different pathogenesis and incidence. Unfortunately, with rare exceptions, most published case reports and review articles refer to TH simply as massive thymic enlargement seen on a chest radiograph (CXR) or chest CT without reference to weight, size, or histologic definitions. This has resulted in great heterogeneity in what has been defined as TH and reported in the literature.
Incidence of TH in GD
True Thymic Hyperplasia
TTH always presents with an enlarged thymus gland (13,19,20). Its incidence is likely to parallel the incidence of radiographically diagnosed thymic enlargement. The true incidence of radiographic TH in GD is not known, since a study diagnosing the condition in a cohort of unselected patients with GD has not been performed.
Thymic Lymphoid Hyperplasia
TLH is seen in only 1–2% of normal individuals (26,27) but is a common finding in patients with hyperthyroidism. Michi and Gunn (28) obtained thymic biopsies on 143 patients undergoing thyroidectomy for various reasons and found that 38% of patients with thyrotoxicosis had histological evidence of TLH. Likewise, Simpson et al. (29) performed thymic biopsies on 158 female patients with primary thyrotoxicosis who were undergoing thyroidectomy. Fifty-one female patients undergoing partial thyroidectomy for nontoxic nodular goiter served as controls. The authors found that at all ages, the lymphoid component of the thymus in thyrotoxic patients was greater (p < 0.001) than in patients with nontoxic nodular goiter.
Pathogenesis of TH
The association between GD and TH was first described by Matti in 1912 (10) and later by Halsted (30) in 1914. A debate as to whether TH represents the cause of GD or is a consequence of GD continued for many years. Halsted went as far as to attribute certain clinical and laboratory features of GD to TH. He, as well as others, suggested performing thymectomy to cure GD but attained conflicting results (29). In 1971, Van Herle et al. (31) removed a hyperplastic thymus from a patient with GD and showed that thymectomy had no effect on thyroid hormone levels. Furthermore, long-acting thyroid stimulator and TSH were not detected in the saline extract of the thymus, suggesting that the thymus was not the source of a thyroid-stimulating factor, as was previously believed. When considering other autoimmune diseases, thymectomy has a variable effect on their course. Certain subgroups of patients with myasthenia gravis, ulcerative colitis, polymyositis, pure red-cell aplasia and multiple sclerosis may benefit from thymectomy (32). However, it is of questionable benefit in patients with rheumatoid arthritis and autoimmune hemolytic anemia. On the other hand, SLE may worsen or the disease may be triggered after thymectomy (32).
GD is associated with both TTH and TLH via putative thyroid excess and autoimmune mechanisms, respectively. The pathogenesis of each will now be discussed separately.
Thyroid hormone excess and TTH
Several animal and human studies support the hypothesis that thyroid hormone induces TTH predominantly via stimulation of the thymic cortex.
First, in 1924, David Marine et al. (33) showed that thyroidectomy hastened normal, age-related thymic involution in rabbits younger than seven months of age. In 1951, Marder (34) provoked thymic involution in immature female mice by administering adrenocortical hormone and then demonstrated an increase in thymic weight when these mice were treated with thyroxine. In 1959, Höhn (35) studied hens, and reported increases in thymic weight, cortical thickness, as well as cortical and medullary vascularity after administration of thyroxine. Likewise, Warner (36) noted regeneration of atrophic thymic cortex in adult chickens after administration of thyroid hormone. In 1975, Simpson et al. (29) compared thymic histology between two groups of hyperthyroid patients undergoing surgery. The authors examined age-related thymic involution in those treated preoperatively with ATD compared to those treated with propranolol. Age-related involution of total thymic parenchyma was less in the propranolol-treated compared to the ATD-treated group. This difference was attributed to cortical involution seen in the ATD treatment group, since involution of the medulla was similar in both groups, supporting the hypothesis of an effect of thyroid hormone predominantly on the thymic cortex. In further support of this hypothesis, Scheiff et al. (10) demonstrated the effect of thyroid hormone on the thymic epithelial cells for the first time, and noted an absolute increase in the number of epithelial cells in the cortex and medulla. The authors did, however, also note proliferation of cortical lymphocytes, while medullary lymphocytes were unaffected by thyroid hormone. However, neither germinal center development nor proliferation of Hassel bodies, both hallmarks of TLH, could be detected after triiodothyronine administration. Therefore, the effect of thyroid hormone on thymic epithelial cells and cortical lymphocytes requires further investigation to elucidate the complex pathophysiology of TH associated with GD.
The exact mechanisms via which thyroid hormones exert influence on thymic growth remain unclear. It is known that thymic epithelial cells produce hormone-like substances that are required for T-lymphocyte differentiation and function. In 1986, Fabris (37) showed that in humans, thyroid hormone could modulate the secretion of a thymic factor called thymulin. Plasma thymulin levels were found to be elevated in hyperthyroid subjects and low in hypothyroid individuals when compared to normal subjects. This suggested that thyroid hormone may possibly influence thymic function via modulation of thymic hormone levels.
In summary, these studies provide evidence supporting an effect of thyroid hormone on thymic tissue, preferentially the epithelial component and cortical lymphoid tissue, sparing the medullary lymphoid component.
Autoimmunity and TLH
In addition to GD, several other autoimmune diseases are associated with the development of TLH. These include myasthenia gravis (21), progressive systemic sclerosis (22), rheumatoid arthritis (23), and SLE (24,25). In fact, the diagnosis of TLH cannot be made outside the context of autoimmune disease. Furthermore, while thyroid hormone does not exert effects on medullary lymphoid tissue, the presence of medullary lymphoid follicles is well documented in GD as well as other autoimmune diseases. This suggests an autoimmune-mediated basis for TLH.
GD is associated with anti-TSH-R immunoglobulin G (IgG) antibodies (Abs), which are thought to activate the thyroidal TSH-R, causing thyroid epithelial cell hyperplasia and thyrotoxicosis. The TSH receptor, however, is also found in extrathyroidal human and mammalian tissues, including the thymus. In 1996, Murakami et al. (38) first identified TSH-Rs in the human thymus by polymerase chain reaction amplification, Northern blot, Western blot, and immunohistochemistry. These findings are supported by others who have shown the presence of normal and variant TSH-R mRNA, expression of thyroid-related genes, and TSH-R protein (8,39,40) in the human thymus. Thymic TSH-Rs have been shown to be functional (41). It is possible therefore that anti-TSH-R Abs may exert a direct effect on thymic cells via activation of the TSH-R.
Additionally, circulating IgG Abs, with binding affinity to normal thymocytes and the ability to evoke a mitogenic response, have been detected in some patients with GD (42).
Summary of the pathogenesis of TH
Based on the available data, it appears that the TH seen in patients with GD has both a thyroid hormone–dependent and immunologic pathogenesis. Thyroid hormones appear to affect the cortex predominantly (TTH), while immunological mechanisms may be responsible for the formation of medullary lymphoid follicles (TLH).
In conclusion, TH associated with GD appears to be caused by a complex interplay of both hormonal and immunological factors. More investigation is needed to elucidate fully the mechanisms involved and to clarify the role of each in the pathogenesis of TH.
Evaluation of GD-associated thymic enlargement
The thymus enlarges continuously from birth until puberty, followed by a progressive regression, called age-related involution. When thymic enlargement is observed on X-ray, the subsequent management course is controversial. The possibility of malignancy exists, with the greatest observed risk for malignancy (59%) occurring between the ages of 20 and 40 years. The risk for younger and older patient groups drops to approximately 30% (43).
Differential diagnosis
In many cases, the discovery of an anterior mediastinal mass prompts a surgical resection via median sternotomy. Although it is important to consider the possibility of malignancy, other benign and autoimmune conditions that can cause an increase in thymic size must also be considered.
The differential diagnosis for an anterior mediastinal mass includes lymphoma, germ-cell tumor, mesenchymal tumor, thyroid or parathyroid masses, metastatic tumors, thymomas, and TH. TH also occurs with Addison's disease and after adrenalectomy in all age groups. In addition, gonadectomy has been shown to delay thymic involution in both males and females (33). These endocrine causes of thymic enlargement, though rare, should be excluded when evaluating an anterior mediastinal mass (Fig. 2). Thymic enlargement diagnosed outside the context of GD should prompt appropriate evaluation for other autoimmune diseases associated with TH and thymoma when signs or symptoms are suggestive of their presence.
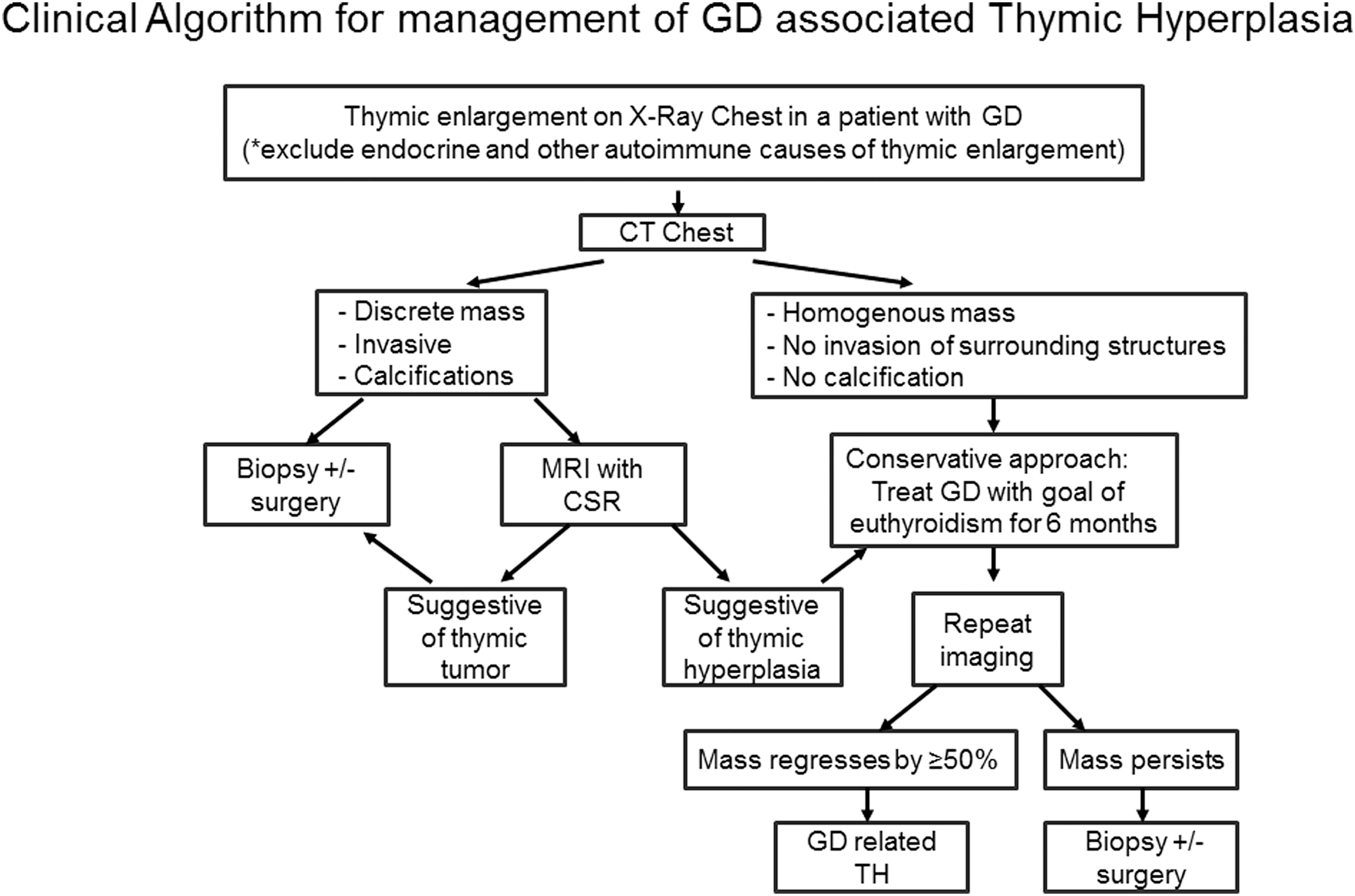
Suggested algorithm for the clinical evaluation of thymic enlargement associated with GD. Potential individual patient variations should be taken into consideration. *See section: Differential Diagnosis.
Symptomatology
One recently published study retrospectively examined 109 thymectomies, of which 36 yielded diffuse thymic enlargement. This group of 36 patients with diffuse enlargement was further subclassified based on symptoms into 18 symptomatic (chest discomfort, shortness of breath, and pain) and 18 asymptomatic cases. Within the asymptomatic group, none had a pathological diagnosis that would have required surgery (8 normal, 10 hyperplasia), while four (22%) in the symptomatic group harbored a lymphoma. Of the remaining 73 cases noted to harbor a discrete mass in the thymus, both symptomatic and asymptomatic patients had a higher rate of pathological diagnosis warranting resection (symptomatic 53%, asymptomatic 42.8%) (44).
Thirteen (including the authors' own) case reports of GD-associated thymic enlargement presenting with symptoms of pain, neck fullness or shortness of breath (Fig. 3) were reviewed. Of these 13, nine were observed without surgical intervention, and all regressed on follow-up imaging (40,45 –49) (two of the nine were biopsy-proven TH) (40,46). Two of the 13 patients underwent thymectomy, with a final histologic diagnosis of TH (50,51), and the two remaining cases were lost to follow-up (42,45) (one of the two cases was biopsy-proven TH; Fig. 3) (42). Based on these limited data, symptoms in the context of thymic enlargement associated with GD do not appear to portend a higher risk for pathology warranting surgery.
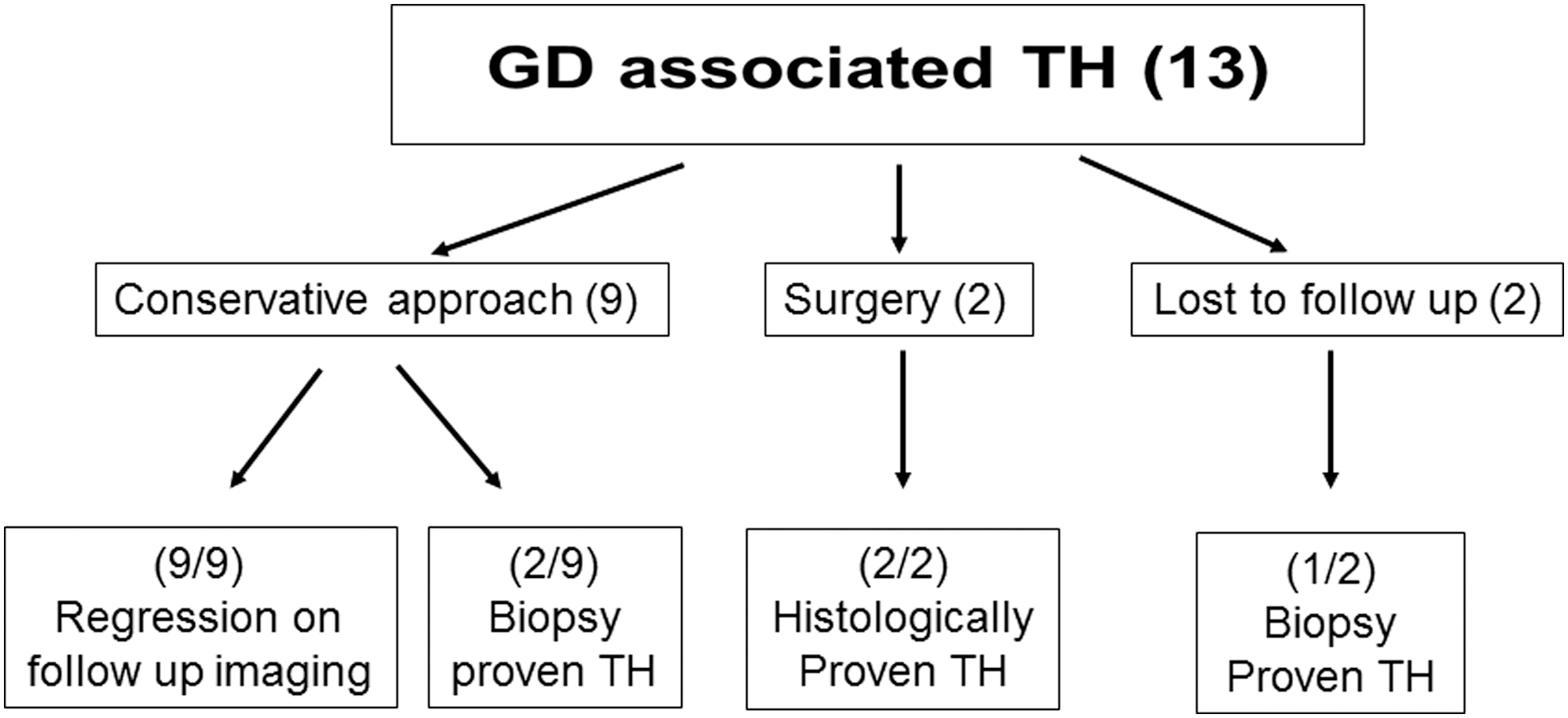
Outcome of 13 individual cases of GD-associated thymic enlargement, presenting with symptoms of neck pain, neck fullness, or shortness of breath.
Imaging studies
Whenever an anterior mediastinal mass is seen on CXR, CT is the follow-up imaging of choice, as it helps to: (i) differentiate between benign cystic and solid tumors, (ii) define the extent of disease, (iii) differentiate between thymomas and TH in the context of myasthenia gravis, and (iv) assess thymic thickness identifying an infiltrative processes (TH and lymphoma) (15,16). If suspicious radiological features are present on CT, then the use of magnetic resonance imaging (MRI) with chemical shift ratio (CSR) should be performed where available in an attempt to differentiate TH from thymic tumors. CSR is determined by comparing the signal intensity of the thymus to that of a paraspinal muscle. A comparison of patients with TH (n = 23) to a thymic tumor subgroup (n = 18) demonstrated a lower CSR in the TH group (mean CSR ± SD = 0.614 ± 0.130) compared to the thymic tumor group (mean CSR ± SD = 1.026 ± 0.039; p < 0.001). The lower CSR in the hyperplastic group is due to normal fat infiltration of the hyperplastic thymus, which is absent in thymic tumors (52). Another study prospectively compared CSR and signal intensity index between 30 subjects with TH and 62 subjects with anterior mediastinal tumors (53). The test distinguished between the two groups with reported respective sensitivities and specificities of 100% for signal intensity index (cutoff 8.92%) and 100% and 96.7% for CSR (cutoff 0.849).
It is reassuring that all 12 reported cases of GD-associated TH evaluated by surgical pathology (13,20,31,46,50,51,54 –57) and all five evaluated by thymic biopsy (42,46,58 –60) were confirmed to be benign. The benign nature of GD-associated TH is also suggested by a radiological study by Murakami et al. (38) who demonstrated a statistically significant decrease in mean thymic size and thymic density in 13 patients with GD after 5–24 months of treatment with ATD.
After an exhaustive literature search including 47 cases, only one published case of invasive thymoma associated with GD could be found (61). Thus, the association of thymoma with GD appears to be rare. Compared to GD, other autoimmune diseases associated with TH show a higher incidence of thymomas. Thymoma was noted in 10–15% of myasthenia gravis cases, 1.5–10% of SLE, and 5% of pure red-cell aplasia patients; pemphigus, polymyositis, and pernicious anemia also have known associations with thymomas (32,62).
Effect of treatment of GD on radiologically evident TH
A CT study of 13 patients with GDs compared thymic size and density at baseline and after treatment with ATD. The study showed a decrease in size (p < 0.001) and density (p < 0.01) of the thymus in all 13 patients studied (38). The mean thymic area decreased by 56%, suggesting that treatment of GD leads to regression of TH. In six other individual cases where thymic volume or area was measured before and after ATD drug therapy, thymic volume or area decreased between 33% and 90% and by an average of 62% (40,45,59,63,64). Yacoub et al. (50) reviewed 21 published case reports of GD-associated anterior mediastinal masses and separated them based on those who underwent surgical resection (eight case reports) and observation on ATD treatment (13 case reports). Of the eight patients who underwent a thymectomy, seven had benign TH and one had a benign thymolipoma. One patient received a thymectomy eight weeks after initiating treatment for hyperthyroidism due to an absence of regression of the anterior mediastinal mass. This patient was found to have benign TH but unfortunately incurred phrenic nerve paralysis during the procedure. The anticipated regression of TH after treatment of GD was not observed in this subject likely due to the short duration of treatment (less than six months) or to noncompliance with treatment, resulting in failure to achieve a euthyroid state (50). Of the 13 patients who were observed while receiving treatment for GD, the thymus regressed in all, with follow-up ranging from six weeks to two years (50). In six of these cases, follow-up scans were performed at six months, and regression of TH was seen in all cases. Unfortunately, many individual cases reports (n = 12) describe “dramatic regression” or disappearance of mass without quantifying the regression (46,47,49,54,58,60,65 –68). In the present patient, the anterior mediastinal mass showed an 85% regression by volume within six months of initiating drug treatment for hyperthyroidism.
A total of 47 published case reports of GD-associated TH were reviewed, 17 of which had histologic or biopsy proven TH (noted above) and 31 of which showed regression on radiological follow-up (38,40,45 –47,49,54,58 –60,63 –68), providing reassurance of the benign nature of TH associated with GD.
Management recommendations
Although CXR is not routinely indicated for evaluating mediastinal mass in GD, if a mediastinal mass is seen on CXR in the context of a diagnosis of GD, CT of the neck and chest should be performed to characterize the thymus (Fig. 2). If the thymic mass is homogenous, does not invade surrounding structures, lacks calcification, and is non-cystic and thus consistent with TH, it is reasonable to proceed with treatment of the hyperthyroidism, as clinically indicated, utilizing the appropriate treatment modality.
If any suspicious radiological feature such as calcification, discrete mass, or invasion into surrounding structures is present on CT, then the use of MRI with CSR (where available) should be considered in an attempt to differentiate TH from thymic tumors (Fig. 2). A thymic biopsy may be considered at this point in settings where MRI with CSR is not available. Treatment of the hyperthyroidism should of course be instituted concurrently.
When the likelihood of malignancy is low and findings are consistent with a diagnosis of TH in the context of GD, it is reasonable to treat the hyperthyroidism for at least six months before a follow-up CT is performed (Fig. 2). It is important to achieve a euthyroid state for this duration, as noncompliance may delay resolution of the GD associated TH (50,54,59). At six months, the majority of cases of GD-associated TH will show regression in area or volume of ≥50%, reassuring the physician of the diagnosis. If significant regression, as described, is not seen after six months of euthyroidism, then thymic biopsy may be considered, even when the index of suspicion is low. The result of the biopsy will then dictate further management. Potential individual patient variations should be taken into consideration, and a multidisciplinary team approach including surgeons, radiologists, endocrinologists, and the primary-care physician is highly recommended in such cases.
Conclusion
In conclusion, it is important for clinicians to recognize the association of TH with GD. Based on this review, it was found that this condition is most often benign, regresses with the treatment of GD, and does not require surgical intervention. Therefore, the finding of TH in association with GD warrants a conservative approach, medical treatment, and radiological follow-up.
Footnotes
Acknowledgments
We would like to acknowledge Tauseef Haider, MD, and Marelle Yehuda, MD, for their manuscript review and constructive comments.
Author Disclosure Statement
The authors have no disclosures to report.