
Abstract

Iodine is an essential micronutrient for thyroid hormone production. Adequate maternal thyroid hormone in pregnancy is important for fetal neurodevelopment, and even mild iodine deficiency in pregnant women has been linked to lower cognitive function in their children (1). Pregnant women have increased dietary iodine requirements due to increased thyroid hormone production, transfer of iodine to the fetus, and increased urinary iodine losses. Lactating women need a higher iodine intake because iodine secreted in breast milk is essential for child nutrition. The World Health Organization recommends 250 μg/day of iodine intake while pregnant or breast-feeding, higher than the 150 μg/day recommended for nonpregnant adults (2). Although the general U.S. population is iodine sufficient, recent data demonstrate that U.S. pregnant women are currently mildly iodine deficient (1). The American Thyroid Association (ATA) recommends that women who are planning pregnancy, pregnant, or lactating take supplements containing 150 μg of iodine/day (1). The addition of iodine to prenatal multivitamins and supplements (PNVs) is not mandatory in the United States. Leung et al. assessed commercially available U.S. PNVs in 2009 and found that only 51% contained iodine (3). In January 2015, the Council for Responsible Nutrition (CRN), a U.S. trade group for supplement manufacturers, recommended that multivitamin/multi-mineral supplements intended for pregnant or lactating women in the United States should include at least 150 μg of iodine per daily dose (PDD) (4).
To assess the current iodine content of commercially available U.S. PNVs, we identified a total of 386 PNVs (234 [61%] nonprescription and 152 [39%] available by prescription) using the National Institutes of Health Dietary Supplement Label Database, the Natural Medicines Database, and the U.S. National Library of Medicine DailyMed database. Iodine content and sources were obtained from product labels. Of these, 237 (61%) PNVs contained iodine: 167 (71%) nonprescription and 70 (46%) prescription PNVs (Fig. 1). The mean iodine content was 165.7 μg PDD (median 150 μg PDD; range 10–450 μg PDD). The majority of the PNVs with iodine (n = 212; 89%) included at least 150 μg of iodine PDD. The most common source of iodine was potassium iodide (n = 151; 64%), followed by kelp (n = 61; 26%) and other sources such as yeast (n = 7; 3%). Fifty-four PNVs were marketed by members of CRN. Most of these PNVs (n = 50; 93%) contained at least 150 μg of iodine PDD.
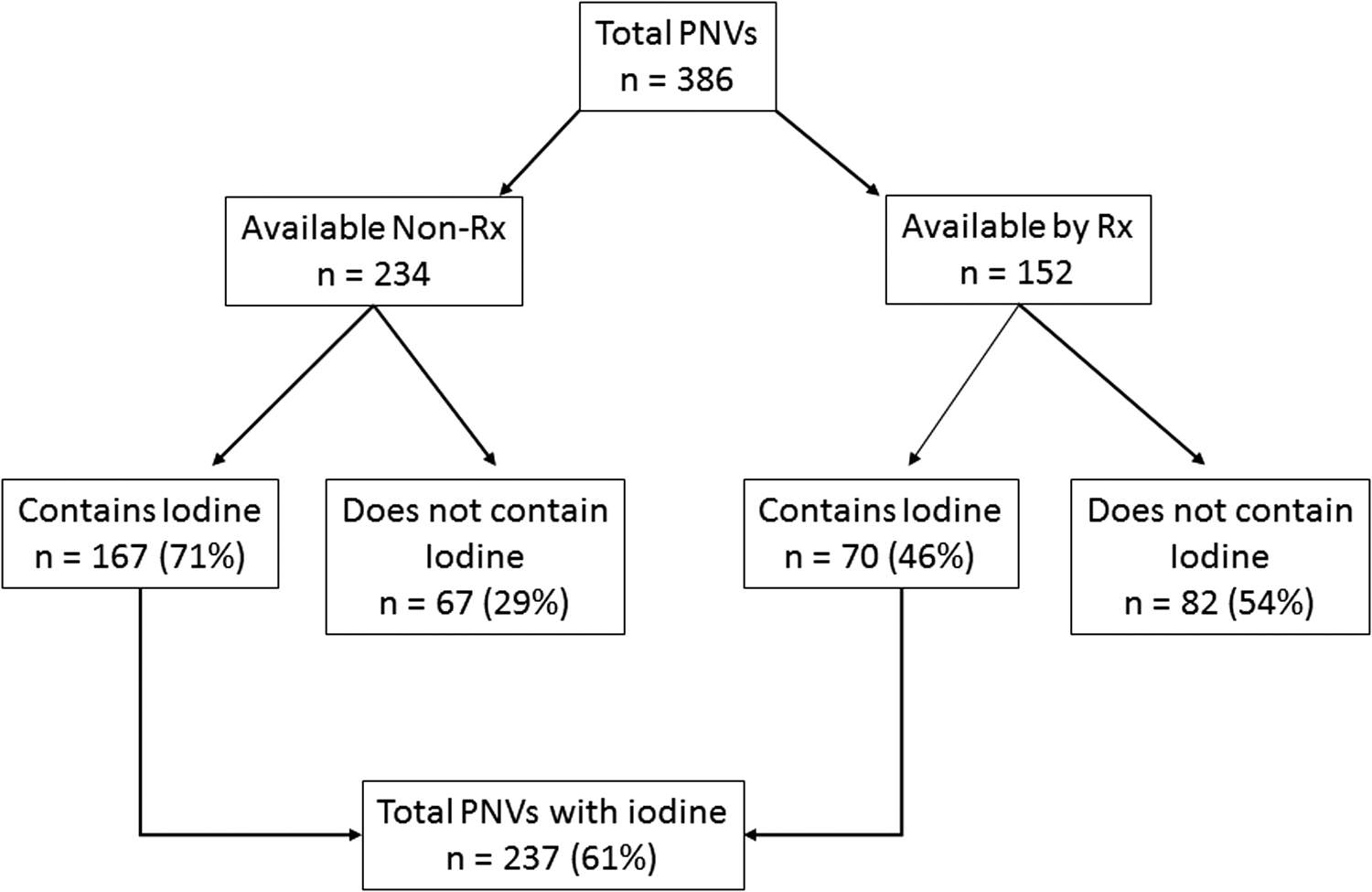
The proportions of U.S. prenatal vitamins and supplements containing iodine. PNVs, prenatal vitamins and supplements; Non-Rx, nonprescription; Rx, prescription.
The proportion of U.S. PNVs containing iodine increased modestly since 2009, although a direct comparison of data was not possible due to the different methodology used to identify PNVs. Nearly all of the PNVs marketed by CRN member companies included at least 150 μg of iodine PDD, demonstrating the impact of industry self-regulatory initiatives on trade association members. The data do, however, indicate that additional efforts are needed to ensure widespread adoption of the CRN recommendations. The wide range of iodine PDD (from 10 to 450 μg in iodine-containing PNVs) raises concern for potential iodine excess, which could negatively impact thyroid health. The success of the ATA and other medical societies' efforts to protect the developing fetus from the negative effects of iodine insufficiency is dependent on industry's commitment to manufacture and market PNV that provide 150 μg of iodine PDD. Healthcare providers can provide further support by ensuring that any PNV they recommend includes the recommended amount of iodine.
Footnotes
Author Disclosure Statement
No competing financial interests exist.