
Abstract
Background:
The retinoblastoma (RB) transcriptional corepressor 1 protein functions to slow cell-cycle progression. Inactivation of RB by reduced expression and/or hyperphosphorylation allow for enhanced progression through the cell cycle. Murine models develop medullary thyroid carcinoma (MTC) after generalized loss of RB. However, RB expression in MTC has only been evaluated in a small number of tumors, with differing results. The objective of this study was to determine whether reduced expression of RB and/or overexpression of hyperphosphorylated RB predict MTC aggressive behavior.
Methods:
Formalin-fixed, paraffin-embedded primary thyroid tumors and lymph node metastases from MTC patients were evaluated for calcitonin, RB, and phosphorylated RB (pRB) expression by immunohistochemistry. Two expert pathologists evaluated the slides in a blinded manner, and the immunohistochemistry results were compared to disease-specific survival as a primary endpoint.
Results:
Seventy-four MTC samples from 56 patients were analyzed in this study, including 51 primary tumors and 23 lymph node metastases. The median follow-up time was 6.75 years after surgery (range 0.64–24.30 years), and the median primary tumor size was 30 mm (range 6–96 mm). Sixty-six percent of cases were classified as stage IV. RB nuclear expression was diffusely present in 88% of primary tumors and 78% of lymph node metastases. Nuclear pRB expression was present in 22% of primary tumors and 22% of lymph node metastases. On univariate analysis, reduced RB (<75% tumor cell staining) trended with lower MTC-specific survival for primary tumor and metastatic nodes (primary tumor hazard ratio = 3.54 [confidence interval 0.81–15.47], p = 0.08; and lymph node hazard ratio = 4.35 [confidence interval 0.87–21.83], p = 0.05). For primary tumors, multivariable analysis showed that low nuclear RB expression was independently associated with worse disease-specific (p = 0.01) and overall (p = 0.02) survival. pRB levels were not associated with survival for either primary tumor or lymph node metastases.
Conclusions:
Reduced RB expression is associated with decreased patient survival in univariate and multivariable analyses, independent from patient age at surgery or advanced TNM stage. Future studies involving larger MTC patient populations are warranted to determine if lower RB expression levels may serve as a biomarker for aggressive disease in patients with MTC.
Introduction
M
MTC can occur in a hereditary manner as part of the Multiple Endocrine Neoplasia Type 2 (MEN2) syndromes, accounting for 25% of MTC cases, whereas sporadic tumors represent 75% of cases (1). Nearly all hereditary and ∼40% of sporadic MTC cases are caused by germline or somatic activating mutations in RET, respectively (1). RET encodes a receptor tyrosine kinase (9), which is activated by binding of glial cell line–derived neurotrophic factor (GDNF) family of ligands, which are pre-bound to GDNF-family receptor alpha proteins. Homodimerization and transphosphorylation of RET occurs after the binding of its ligands. This event activates multiple downstream pathways such as RAS/MAPK, PI3K/AKT, JAK/STAT, and PKC (10).
Because approximately 60% of sporadic MTCs do not harbor RET mutations, additional oncogenic drivers have been investigated (11). Somatic mutations in the rat sarcoma viral oncogene homolog gene (RAS) have been described in MTC, with a frequency ranging from 18% to 81% (12 –15) depending on the population. It has been reported in some studies that sporadic MTCs harboring somatic RET mutations, particularly the most common mutations at codon 918, have a more aggressive course, but this has not been confirmed in all populations (16 –18). Modifiers or predictors of more aggressive MTC beyond clinical parameters remain an important area for both predictive testing and in order to identify new therapeutic targets.
One candidate alternative pathway for MTC development is the CDK/RB cell-cycle regulatory pathway (Fig. 1). The retinoblastoma (RB1) tumor suppressor has been reported to be mutated in many human cancers such as sarcomas, glioblastomas, and small-cell and non-small-cell carcinomas of the lung, among others (19 –23). Multiple studies in mice involving genetic inactivation of the RB pathway have shown that neuroendocrine cells exhibit specific sensitivity to loss of cell-cycle regulation. It has been demonstrated, for example, that germline heterozygous loss of rb and other members of the pathway. including cyclin dependent kinase inhibitors (CDKIs) p18 and p27, results in a high rate of MTC in mice (24). Concomitant loss of p18 and p27 increases the incidence of MTC occurrence in RET transgenic mice (25 –29). In addition, homozygous deletion of Rb1 in the mouse thyroid in a p53 null background produces an aggressive MTC phenotype (30). Furthermore, overactivation of CDK5 in mice resulted in a MTC phenotype through an RB-mediated mechanism (31). In sporadic and hereditary MTC, loss of a section of the p arm of chromosome 1 that includes the genes encoding p18 and E2F2 has been commonly found (25 –27). These reports together suggest that the CDK/RB pathway may be important in the development of human MTC.

CDK/RB pathway and its regulators. Retinoblastoma (RB) is phosphorylated through G1 phase by cyclin/CDK complexes, resulting in inactivation. Hyperphosphorylated RB by CDKs releases E2F transcription factors, allowing for cell-cycle progression. Activated RET can induce MAPK activation, which increases cyclin D production. Both families of CDKIs are negative regulators of the pathway. Activation of p53 promotes p21 transcription, further inhibiting cell-cycle progression.
RB functions to regulate progression through the cell cycle (32), as depicted in Figure 1. Post-translational inactivation of RB through phosphorylation by cyclin kinases leads to release of E2F transcription factors from their binding to RB, and to progression of the cell cycle. To date, only a single frameshift mutation in RB has been reported in 54 human MTCs in the COSMIC database and/or reported in the literature (33). Somatic inactivating p18 mutations have been found in a subset of human MTC samples (26), as has p18 loss of heterozygosity (LOH) (34). Additionally, SNP genotyping in MTC patients found an association of p27 and p16 variants with MTC (35). A number of small immunohistochemistry (IHC) studies have been performed to determine RB protein expression in thyroid neoplasms, including MTC tissue samples, with RB presence varying from 29% to 100% (36 –39). Some of these studies correlated RB positivity to benign neoplasms (39), while others found no association with the clinical course in MTC samples (37). The present study tested the hypothesis that RB inactivation, through either reduced nuclear expression or inactivation by hyperphosphorylation, is associated with poor outcomes in a larger series of patients with MTC.
Materials and Methods
Tissue and clinical data
Patients who underwent surgical intervention for the treatment of MTC at the University of Texas MD Anderson Cancer Center (MDACC) and the Ohio State University (OSU) between 1989 and 2010 and who had tissue available for evaluation were included in this retrospective Institutional Review Board–approved study. Tissues selected for evaluation included primary tumor and/or metastatic lymph nodes. Corresponding clinical data were retrieved from prospectively maintained databases within the Departments of Surgical Oncology at MDACC and the Thyroid Cancer Unit at OSU, including patient demographics, surgical details, pathology findings, imaging results, laboratory results, and disease course through the follow-up period of this study. RET germline testing to include exons 10, 11, and 13–16 was performed in all patients in CLIA-approved laboratories as part of patient care. Sporadic MTC cases were defined by lack of germline RET mutations, clinical evaluation, and the absence of family history. TNM staging was based on the 7th edition of the American Joint Committee on Cancer criteria (40). Pathology variables included the greatest dimension of primary tumor size, presence or absence of extrathyroidal extension, lymphovascular invasion in the primary tumor, the presence or absence of nodal metastases, and the presence or absence of gross invasion into adjacent structures (determined by histology and surgeon's notes). The presence or absence of distant metastases was determined by the treating thyroid cancer specialty physician, including imaging as indicated. During the time frame of this study, standardized reporting of all thyroid pathology was exclusively performed or re-reviewed by head and neck specialized pathologists.
Immunohistochemistry evaluation
RB immunohistochemical analysis was performed in a CLIA setting using an automated immunohistochemistry staining system and the protocol utilized for routine patient care in other tumor types, RB antibody (#9309; Cell Signaling Technology, Danvers, MA; 1:100 dilution). In the case of phosphorylated (pRB), Vector kits (Vector Laboratories, Inc., Burlingame, CA) were used, according to the manufacturer's instructions. Briefly, the MTC tissue slides were deparaffinized using xylene, hydrated using a graded ethanol sequence (100%, 95%, and 70% ethanol), and incubated in 3% hydrogen peroxide solution for 10 min after microwave treatment for 5.5 min in a citrate-based antigen unmasking solution. The slides were incubated in pRB (Ser807/811) antibody (#9308; Cell Signaling Technology; 1:100 dilution) overnight at 4°C after blocking for 30 min with horse serum from the Vectastain Universal Quick Kit. A biotinylated, universal pan-specific secondary antibody was applied for 1 h, followed by streptavidin/peroxidase staining for 10 min, and incubation for 2 min in diaminobenzidine substrate (DAB Peroxidase Substrate Kit). Counterstaining was performed with hematoxylin for 2 min.
Prior to staining, a hematoxylin and eosin (H&E) section was reviewed for every tumor for block selection by the institution's expert pathologists (P.E.W. and M.D.W.). Following staining, the IHC slides were reviewed for quality control and initially evaluated at each institution (P.E.W. at OSU and M.D.W. at MDACC). In a joint review, both expert pathologists scored the slides for RB and, on different days, pRB. In rare cases where the pathologists differed in their scoring, slides were reevaluated jointly to achieve a consensus score. The entire slide was scanned at 4 × magnification, looking for overall quality of staining and homogeneity versus heterogeneous areas. A percentage of staining was then estimated, accounting for all of the tissue on each slide. Additional assessment then proceeded at 20 × magnification, analyzing 10 fields of view to refine the percentage of nuclear staining in all of the cancer cells per field. IHC guidelines for clinical ER/PR testing, which are the standards of care for biomarker assessment and were the guidelines followed in the evaluation of RB and pRB in this study, denote multiple key points, including review of control tissues, reporting percentage of cells with nuclear assessment either estimation or quantitation (image analysis or manual), and review of the entire slide to assess the tumor-containing areas (41).
RB evaluation followed standard clinical evaluation, with scoring nuclear expression (any intensity) in each tumor as a percent of tumor cells staining from 0% to >90%. As a tumor suppressor gene, the most common patterns that occur clinically are full diffuse expression, >90% of tumor cells with nuclear expression (normal pattern of expression), or near to total loss of tumor cell RB expression, as seen with tumor suppressor gene loss or silencing. An internal positive control was also evaluated in all cases and must be present in order to report tumor cell loss (i.e., RB expression in blood vessels or lymphocytes).
Evaluation of pRB was also performed for the percent of tumor cells with nuclear immunostaining, irrespective of intensity. Each tumor was evaluated for the percent of tumor nuclei staining from 0% (no staining) to 100% nuclear staining, in 10% increments. The entire tissue sample on each slide was reviewed for the determination of pRB and RB expression. The pathologists were blinded to the clinical information pertaining to each case during all phases of the IHC evaluation.
To estimate the relationship between nuclear RB expression and proliferation, mitotic counts were performed for all cases on H&E slides by counting the mitotic cells present in 10 high power fields (hpf), defined as 400 × magnification (10 × objective and 40 × lens). The tumor slides were initially scanned for a mitotic “hotspot” where mitoses were identified, and then 10 fields in that region were counted and reported as mitoses per 10 hpf. This evaluation was performed by P.E.W. for the OSU cases and by M.D.W. for the MDACC cases.
RETM918T somatic gene mutation analysis in sporadic MTC tumor samples
Targeted mutation detection of a somatic RETM918T mutation was performed through the Characterized Cell Line Core facility at MDACC or through the CLIA-certified molecular genetics laboratory in the Department of Pathology at the Ohio State University using tumor-derived genomic DNA from patients without germline RET mutations. This mutation is associated with aggressive MTC behavior in most cohorts (42).
Statistical analyses
For statistical analysis, threshold levels to define positivity and negativity for both RB and pRB were based on the recent literature (36,37,39,43 –45) and on the biological function of RB. Investigators have used a range of scoring systems to determine RB and pRB positivity. These include the use of positive cutoffs based on any staining versus no staining, different percentages of positive nuclei, or estimates of weak, moderate, and strong staining (36,37,39,43 –45). Given the variability in the literature regarding cutoff values to define positivity, ≥75% of nuclear staining was considered RB-positive, given the known importance of haploinsufficiency of RB1 on tumor progression and the estimated nature of IHC. For pRB, three cutoffs were estimated to be ≥50%, ≥20%, and ≥10% based on the existing literature.
A dichotomous approach comparing groups based on RB and pRB expression with three cutoff values was implemented. Three main analyses were performed for three classes of comparisons: (i) RB-positive (≥75%) versus RB-negative (<75%); (ii) pRB-positive versus pRB-negative using the three different cutoffs (≥50% vs. <50%; ≥20% vs. <20%; and ≥10% vs. <10%); and (iii) both RB-positive (≥75%) and pRB-negative (<50%, <20%, and <10%) vs. either RB-negative (<75%) or pRB-positive using the three different cutoffs (≥50%, ≥20%, and ≥10%) to reflect genomic and post-translational causes of loss of RB function. For each comparison level, patient groups were compared by Fisher's exact tests for extrathyroidal extension, invasion into adjacent structures, lymphovascular invasion, the presence or absence of distant metastases, presence of synchronous or metachronous distant metastases, use of systemic therapy, and somatic RETM918T mutational status. A Wilcoxon rank sum test was used to compare the largest tumor size between groups. The Kaplan–Meier estimator was used to compare both all-cause and MTC-specific mortality. Log-rank tests were used to compare survival curves between each categorization and cutoff. Hazard ratios were estimated by Cox proportional hazard models.
For the MTC specific survival analyses, patients who died of causes other than MTC were censored at the time of death. Survival time was measured from the date of surgery to the date of death or last follow-up. In analyses of MTC disease-specific survival (DSS), death due to MTC was considered an event, while death from other or unknown causes was considered a censored observation. In analyses of OS, all deaths were considered events. A multivariable Cox model was fit adjusting for age at surgery and also cancer stage for primary tumors (22/23 lymph node samples were from stage IV cancers, the other was from stage III; therefore, there was not enough variability to include cancer stage in the lymph node models). For MTC mortality in primary tumors, cancer stages I–III were combined versus stage IV in the models. Kappa statistics were calculated for paired primary and lymph node results from the same patient for RB and pRB (10%) positivity. The kappa statistic measured concordance and can range from −1 to 1. For mitotic count analysis, quartiles were calculated from the counts data, and the upper quartile (75th percentile) was used as a cutoff for high mitotic count.
Results
Demographic data
Data were included from 56 patients with MTC during the time period 1989–2010. Seventy-four tumor samples were analyzed, comprising 51 primary tumors (31 from MDACC and 20 from OSU) and 23 lymph node sections (all from MDACC). In 18 patients, paired tumor and lymph node metastases were evaluated. In 33 cases, only primary tumors were analyzed, and in five cases, only lymph node metastases were available for analysis. Primary tumor and lymph node metastases were evaluated separately, and demographic details for the whole population are described in Table 1.
RET codon mutations: M918T (1), C620S (1), C634R (1), V804M (2), and C609Y (1); one patient with unknown mutation but classified clinically as consistent with hereditary MTC.
MEN2, Multiple Endocrine Neoplasia Type 2; AJCC, American Joint Committee on Cancer; MTC, medullary thyroid carcinoma.
Lymphovascular invasion was present in 19/45 primary tumors. The primary MTC tumor size was a median of 30 mm (range 6–96 mm; data available for 47/51 primary tumor cases) and 42 mm (range 12–70 mm; data from the five unpaired lymph node cases). All patients were tested for germline RET mutations in exons 8 and 11–16 using CLIA-approved laboratory methods. There were five hereditary MTC cases in the primary tumor group and three in the lymph node case group. Specific mutations are noted in Table 1. Tissue for somatic RETM918T mutational testing, the most common somatic RET mutation in MTC, was available for 35/51 sporadic primary tumor cases, and 19 out of these 35 were positive for somatic RETM918T .
Reduced nuclear RB and DSS in MTC
Primary tumors
Eighty-eight percent of primary tumor slides stained positive for RB (≥75% cutoff), while 22% were pRB-positive (≥10% cutoff; Table 2). Figure 2 shows representative immunostaining results. On univariate analysis, there was a trend toward association between reduced nuclear RB and decreased MTC-specific patient survival (Fig. 3). The hazard ratio (HR) for DSS using the RB-positive versus RB-negative status for primary tumor cases was 3.54 ([confidence interval (CI) 0.81–15.47]; Fig. 3A; p = 0.08), and for OS, it was 1.83 ([CI 0.49–6.91]; Fig. 3B; p = 0.37).
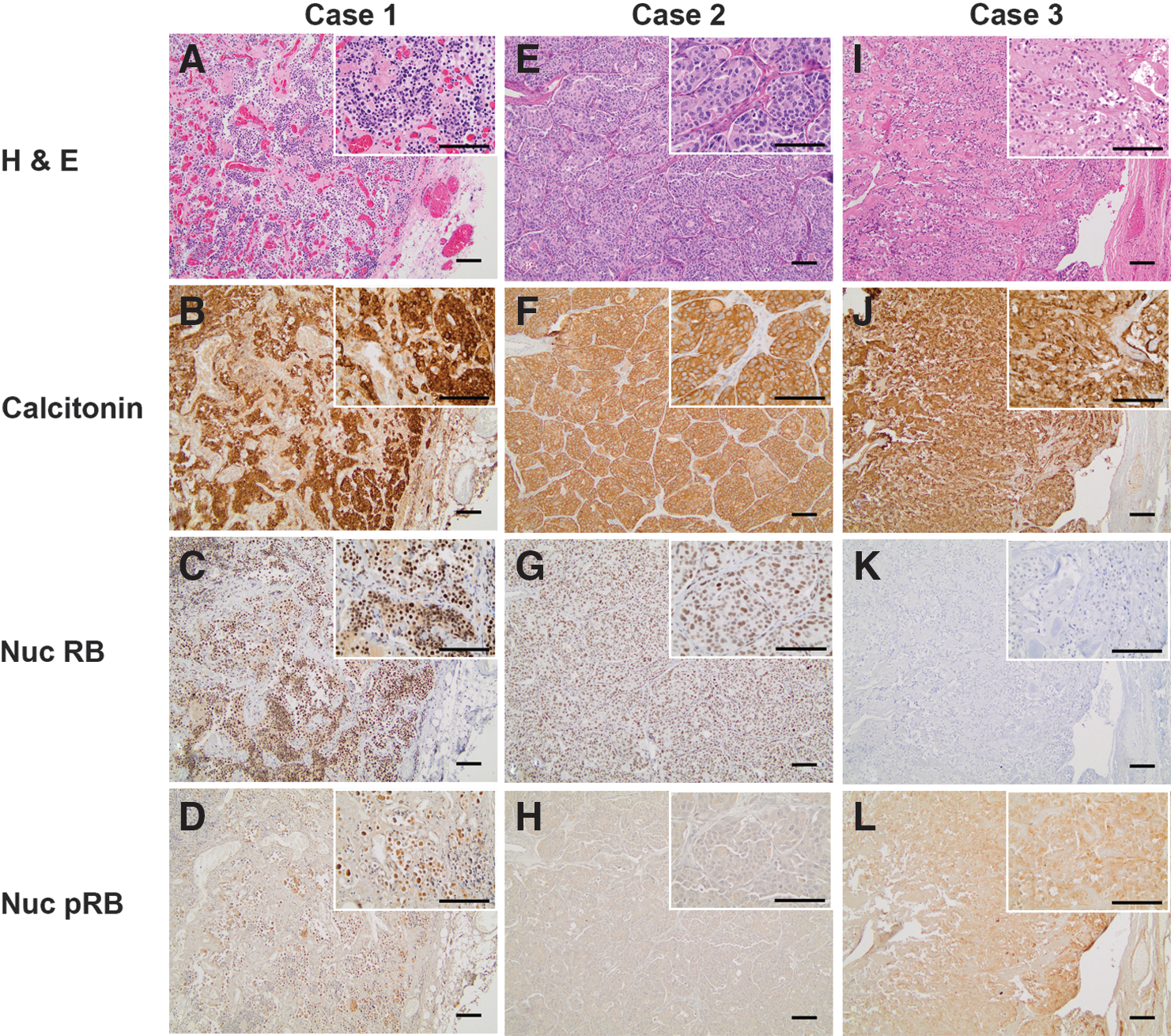
Immunostaining of medullary thyroid carcinoma (MTC) primary tumors. (
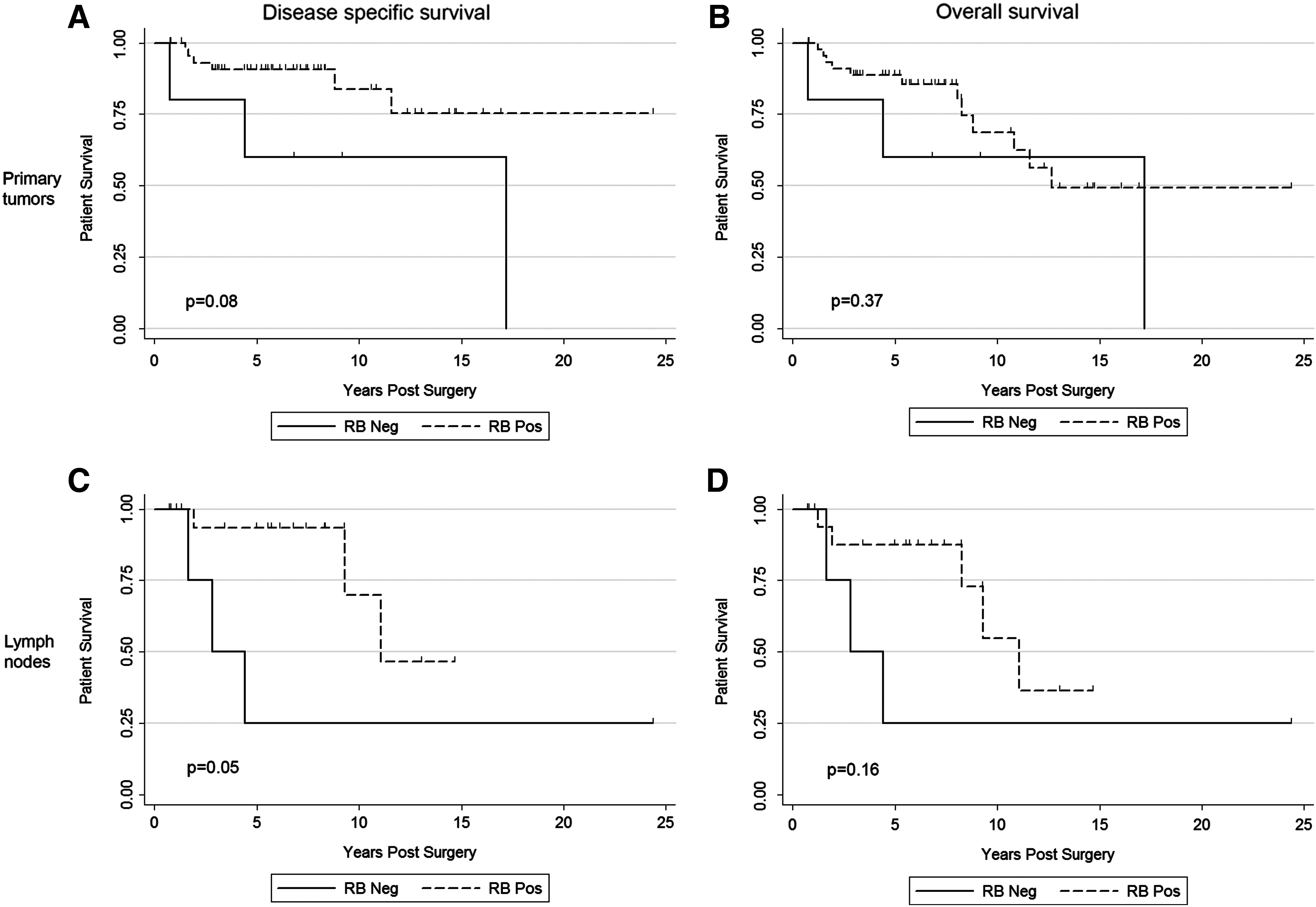
Disease-specific survival (DSS) and overall survival (OS) based on RB-positive (≥75%) or negative (<75%) protein expression for primary tumors and lymph node metastases. (
Lymph node metastasis includes 18 paired with primary thyroid tumor also tested.
RB, retinoblastoma; pRB, phosphorylated RB.
Lymph node metastases
Of the 23 lymph node specimens evaluated, 78% were RB-positive (≥75% cutoff) and 22% were pRB-positive (≥10% cutoff; Table 2). Reduced RB (negative) was associated with decreased MTC-specific patient survival (Fig. 3). The HR for DSS was 4.35 ([CI 0.87–21.83] when evaluating RB-positive vs. RB-negative status; Fig. 3C; p = 0.05), and for OS, it was 2.67 ([CI 0.63–11.29]; Fig. 3D; p = 0.16).
Concordance of RB status between the paired primary thyroid tumors and the corresponding lymph node metastases showed κ = 0.34. Similar analysis was performed for pRB status with the paired samples, showing κ = 0.56 (Supplementary Table S1; Supplementary Data are available online at
Reduced nuclear RB is independently associated with reduced patient survival
To control for potential confounders in the initial analysis, a multivariable Cox proportional hazards model was fit adjusted for age at surgery and tumor stage (Table 3). This analysis demonstrated reduced nuclear RB to be an independent factor associated with DSS (HR = 7.11 [CI 1.60–31.69]; p = 0.01) and OS (HR = 5.47 [CI 1.33–22.54]; p = 0.02]. Age at surgery and stage IV versus stages I–III were also at or near statistical significance but with lower hazard ratio point estimates than RB status (Table 3). Multivariable analysis could not be performed for lymph node cases due to a lack of variability.
RB-positive (≥75% staining).
HR, hazard ratio; CI, confidence interval.
Phosphorylated RB status is not associated with reduced DSS in MTC
Primary tumors
The presence or absence of pRB using the 10% cutoff most common in the literature was not associated with differences in OS or DSS in primary MTC tumors (Fig. 4). For primary tumors, the HR for DSS for pRB-positive versus pRB-negative cases was 1.37 ([CI 0.28–6.83]; Fig. 4A; p = 0.70). The HR for OS in this population was 1.16 ([CI 0.32–4.16]; Fig. 4B; p = 0.82).
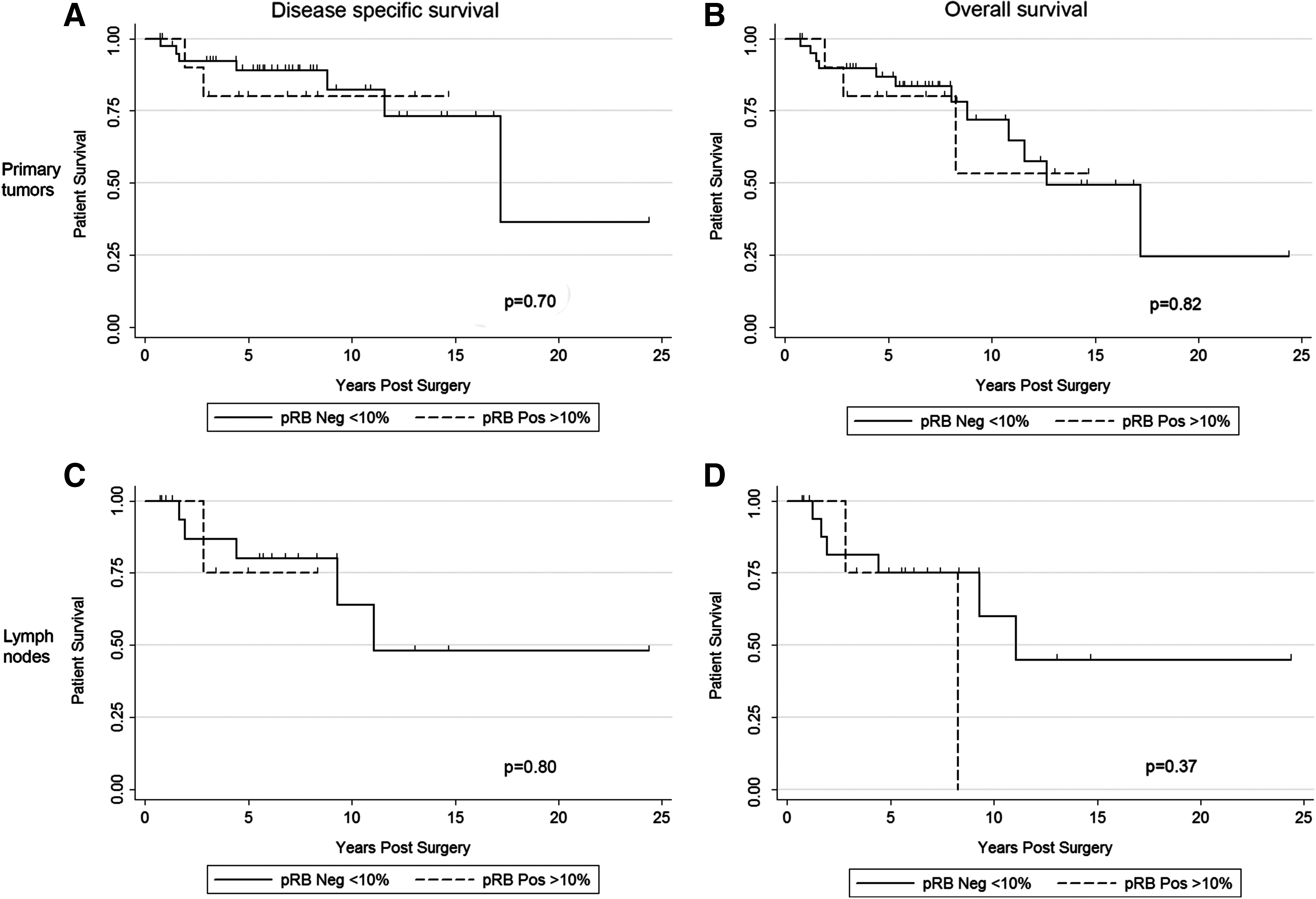
DSS and OS based on based on phosphorylated RB status (≥0%) for primary tumor samples and lymph node metastases. (
Lymph node metastases
Analysis of the lymph node samples revealed similar results. The HR analysis for pRB-positive versus pRB-negative cases in these samples was 1.33 [CI 0.14–13.00] for DSS (Fig. 4C; p = 0.80) and 2.14 [CI 0.39–11.84] for OS (Fig. 4D; p = 0.37).
Due to the discrepancy that exists in the available literature regarding the percentage of positively stained nuclei needed to classify a sample as pRB-positive, survival analysis was performed for primary tumor and lymph node cases using two additional cutoffs (20% and 50%). Supplementary Figures S1 and S2 show survival data using the additional 20% and 50% cutoffs. For both primary tumor samples and lymph node metastases, the analyses using 10% and 20% as pRB cutoffs yielded similar results, and neither of the additional cutoffs (20% or 50%) resulted in association between pRB staining status and patient survival.
Reduced nuclear RB or positive RB phosphorylation combined endpoint is not associated with reduced DSS in MTC
Both reduced nuclear RB and RB hyperphosphorylation result in loss of RB function. Therefore, patient survival was evaluated between two groups: either RB-negative or pRB-positive (at least one marker indicating loss of RB function) versus both RB-positive and pRB-negative (neither marker indicating loss of RB function).
Primary tumors
There was a non-statistically significant trend toward a relationship between a positive RB functional status and longer DSS, with a HR of 2.96 ([CI 0.79–11.17]; Supplementary Fig. S3A; p = 0.09). This potential association was not as apparent for OS, where the HR was 1.63 ([CI 0.58–4.63]; Supplementary Fig. S3B; p = 0.35).
Lymph nodes
Analysis of staining on lymph node samples with survivorship revealed no statistical significant association with either DSS or OS. The HR for the DSS data was 2.43 ([CI 0.48–12.26]; Supplementary Fig. S3C; p = 0.27) versus 2.36 [CI 0.58–9.55] for OS data (Supplementary Fig. S3D; p = 0.22). Patient survival analysis using these two staining groups and 20% or 50% positive nuclei as cutoff for pRB was performed and also revealed no differences between the groups (Supplementary Figs. S4 and S5).
RB status is not associated with clinical/pathology characteristics
As summarized in Table 4, RB expression status was not associated with the individual clinical/pathological variables analyzed, including the presence of distant metastases, or treatment with systemic therapies. Presence of somatic RETM918T mutation was not associated with RB staining category in primary tumors or nodal metastases.
Size of largest tumor was available for 47/51 primary tumor cases and for 20/23 lymph node cases.
Somatic RETM918T mutation status was available for 35/51 primary tumor cases, including hereditary and sporadic cases.
Lymphovascular invasion data were available for 45/51 primary tumor cases and present in 19 cases.
RB phosphorylation status and clinical and pathology features are summarized in Table 5. Similar to total RB levels, no significant relationships were identified. A non-statistically significant inverse trend between positive pRB status and lymphovascular invasion was noted (p = 0.06). No association was observed between somatic RETM918T mutation status and pRB in either primary tumors or nodal metastases. Higher pRB cutoffs also revealed non-significant results (Supplementary Tables S2 and S3).
Size of largest tumor was available for 47/51 primary tumor cases and for 20/23 lymph node cases.
Somatic RETM918T mutation status was available for 35/51 primary tumor cases, including hereditary and sporadic cases.
Lymphovascular invasion data were available for 45/51 primary tumor cases and present in 19 cases.
Relationships between these same features were also evaluated using a combined endpoint for both the RB and pRB category and clinical pathology features (Supplementary Tables S2, S3, and S4). No statistically significant associations were identified. Similarly, analysis of combined endpoint using higher pRB cutoffs did not yield statistically significant results (Supplementary Tables S5 and S6).
Mitotic counts and RB inactivation
RB loss was predicted to be associated with an increase in cellular proliferation and mitotic index. To assess this hypothesis, mitoses were counted for each histological sample.
Primary tumors
Mitotic counts of primary tumor slides were low overall and averaged 1.24 per 10 hpf (standard deviation [SD] = 1.69) with a median value of 1. Of 51 primary tumor samples, three (5.9%) exhibited a mitotic count of ≥4 per hpf, with two out of these samples having either negative RB or positive pRB (using 75% cutoff for RB and 10% for pRB; Supplementary Table S7). Repeating this evaluation using ≥3 mitoses per 10 hpf as an indicator of high mitotic count, the primary tumor group contained seven total high mitotic counts (13.7%), of which three (42.9%) also had either RB-positive or pRB-negative staining. The mitotic count was also examined in relation to RB and pRB staining using the 75th percentile of the mitotic counts. The upper quartile of the mitotic counts for primary tumor samples was 2. Using a cutoff of ≥2 mitoses per 10 hpf in the primary tumor sample pool, the evaluation showed 16/51 (31.4%) cases having this mitotic count, of which six (37.5%) cases had either RB-negative (<75%) or pRB-positive (≥10%) staining.
Lymph nodes
Mitotic counts averaged 2.30 per 10 hpf (SD = 2.77), with a median value of 2. Similar to the primary group, of 21 lymph node samples, three (14.3%) had mitotic count ≥4, with two of these cases having either negative RB or positive pRB (Supplementary Table S7). Two of the high mitotic count cases overlapped between the primary tumor and lymph node metastasis paired samples; both of these cases had either negative RB or positive pRB. Evaluation of the mitotic events using the quartile system revealed the upper quartile (75th percentile) of the mitotic counts to be three for the lymph node metastases. Using ≥3 mitoses per 10 hpf as an indicator of high mitotic count, it was found that there were eight cases out of 21 (38.1%) in the lymph node metastasis group that had a high mitotic count. Of these eight cases, three (37.5%) had either RB-negative of pRB-positive staining. Thus, the RB “activation status” (low RB or high pRB) did not associate with mitotic counts in either the primary tumors or the lymph node metastases samples.
Discussion
Reduced RB expression and therefore loss of RB function is critical to dysfunctional growth in cancer. C cells have a particular sensitivity to loss of RB function in mouse models, as demonstrated by the development of MTC tumors. However, the impact of RB loss in human MTC has been incompletely studied. Previously published studies demonstrate variable results regarding expression of RB in thyroid cancer, with MTC representing only a small number of evaluated samples (36 –39). In the current study, immunohistochemical analysis was performed of 74 total tissue samples obtained from 56 patients (51 primary MTCs and 23 metastatic lymph nodes), and the associations of reduced RB expression or evidence of RB hyperphosphorylation with clinical outcomes were evaluated.
RB is active in its hypophosphorylated form, which enables it to bind to the E2F family of transcription factors, leading to cell-cycle arrest (see Fig. 1) (46). The absence of RB staining or presence of hyperphosphorylated RB on IHC suggests a loss of RB function. The results indicate that lower intratumoral RB expression levels are associated with decreased MTC DSS when it is detected in either primary tumors or lymph node metastases (Fig. 3). In addition, concordance in RB and pRB status was found between paired primary tumor samples and lymph node metastases, suggesting that either it is a clonal event or it represents subclones with greater growth or metastatic advantage (Supplementary Table S1). Consistent with the concept that complete or partial RB loss may mark tumors for more aggressive behavior, multivariable analysis revealed that a reduction of RB expression within the primary tumor cells is associated with reduced DSS, independent of the presence or absence of stage IV disease or age at diagnosis (Table 3). The relationship was magnified for DSS in comparison to OS, and with the multivariable analysis versus the univariate analysis, suggestive of a specific independent effect on MTC. Interestingly, it has recently been reported in a different population of MTC cases that p18 loss on array CGH also corresponds with poor outcomes in MTC (34). These findings, in combination with those in the present study, support the notion that loss of cell-cycle regulation is important in MTC outcomes and associated with aggressive disease. It should be noted that there was a lack of association between reduced RB levels and somatic RET mutations in these sample groups (Tables 4 and 5). However, larger sample sizes are needed to clarify the relationship between RB loss and RET in the context of MTC. Rb loss has been shown to drive MTC progression in a Rb-dependent manner in mice (47). It is speculated that even haploinsufficiency of RB might also magnify the tumor-promoting and progressive effects of driver oncogenes such as RET or RAS due the effects of haploinsufficient RB on cell-cycle regulation and other features such as genomic instability and aneuploidy (48,49), although this hypothesis could not be tested directly in the present association study.
It is also of interest that in this study, pRB status in tissue samples was not associated with patient outcome (Fig. 4). When combining RB and pRB staining groups, the reduced RB- or pRB-positive group was associated with poorer patient survival, but not to a greater statistical degree than RB reduction alone (Supplementary Fig. S3). These results may suggest that loss or partial loss of RB expression is the principal regulatory mechanisms for this protein in MTC. However, there are limitations to testing phosphor-antibodies in formalin-fixed, paraffin-embedded tissues, and this lack of association could be related to the method of tissue testing.
Mitotic rates overall were relatively low for the primary tumors and lymph node metastases. Although mitotic index is used as a prognostic variable in common cancers, to date, mitotic index is not utilized in clinical care for MTC. The lack of association between RB loss/inactivation and mitotic index may reflect the reported impact of RB loss on non-cell-cycle functions such as chromosomal instability, cellular dedifferentiation, angiogenesis, and metastatic potential (50,51); may be related to a lower sensitivity of mitotic index versus RB loss in predicted MTC behavior; or as mentioned above could be related to driver mutations skewing the data to prevent determination of a statistically relevant finding. Further studies of the impact of RB pathway dysregulation in MTC biology are needed to determine mechanisms for the associations in the present study.
There are several limitations to this study. First, although it is relatively a large number for a rare disease, the sample size is still small. Second, follow-up for patients ranged from 0.64 to 24.30 years (Table 1), with many patients lost to follow-up or deceased from other causes over time. Thus, the later time points feature smaller numbers of patients. Third is the challenge associated with phosphor-antibody detection in paraffin tissue sections and the unknown thresholds at which biologic behavior is affected. To minimize this last challenge, conditions were carefully established, a range of cutoff values for pRB were analyzed, included two expert pathology evaluators, and intensity was not included as a scoring component, as intensity is semi-qualitative without clinically established thresholds. Finally, as a retrospective study, treatment effects are not fully accounted for in the survivorship analyses.
In conclusion, in the present study, a statistically significant association was observed between a reduction of RB and decreased DSS in a cohort of patients with MTC. This effect was independent of age at surgery and of the presence of distant metastases, and occurred in the presence or absence of a RETM918T mutation. These findings, if confirmed in a larger validation series, may suggest that low expression of RB in MTC could be used as a biomarker to predict an aggressive course and further support the potential importance of this cell-cycle regulatory protein in MTC biology.
Footnotes
Acknowledgments
This work is supported by NCI grant P50 CA168505 to MDR, NIH cancer center grant P30 CA016058 to Ohio State University, and by an American Cancer Society Research Scholar Grant (121138MRSGM1112901) to EGG.
Author Disclosure Statement
All authors have declared that no competing financial interests exist.