
Abstract
Background:
The application of radioactive iodine in differentiated thyroid carcinomas has become more selective in an attempt to decrease morbidity. While ablative success has been documented, it is less clear how changes in radioactive iodine treatment strategies will influence long-term recurrence rates for patients with larger tumors and adverse pathological features, including extrathyroidal extension and nodal metastases.
Methods:
Patients diagnosed between 1995 and 2008 with differentiated thyroid carcinoma treated with thyroidectomy followed by radioactive iodine treatment were eligible. All patients were followed for a minimum of five years using a standardized follow-up protocol requiring both biochemical and imaging assessments for recurrent disease (n = 219). Patients were stratified by initial radioactive iodine activity, and disease-free survival was calculated using the Kaplan–Meier method, with significant differences defined by the log-rank test.
Results:
In this cohort, 46% of patients had clinical metastases and 74% had primary tumors >1.5 cm. Patients who had recurrences were more likely to present with extrathyroidal extension (p = 0.002) and lymph node metastases at diagnosis (p < 0.001). Patients presenting with both extrathyroidal extension and lymph node metastases had a significantly worse time to progression if treated with <1850 MBq radioactive iodine compared to those patients treated with >1850 MBq (25 months vs. 121 months; p = 0.004). The use of lower-activity radioactive iodine ablative therapy was associated with more early recurrences (p = 0.003). Being aged younger or older than 45 years did not impact the time to recurrence nor did the use of level 6 dissection. On multivariate analysis, lymph node metastases at diagnosis and multiple applications of radioactive iodine were linked to increased risk of recurrence. Patients with neither, or only one, adverse pathologic feature had excellent outcomes, regardless of initial ablative activity, with <10% of patients recurring over a 10-year time span.
Conclusions:
Recurrent disease in differentiated thyroid carcinoma is more common in patients treated with low-activity radioactive iodine in patients with lymph node metastases and extrathyroidal extension. These recurrences typically occur within four years of initial treatment. Patients lacking both of these risk factors treated with low radioactive iodine activity (<1850 MBq) have excellent outcomes, even after 10 years.
Introduction
P
An important feature that predicts poor outcomes and disease recurrence for patients with well-differentiated variants of thyroid cancer is resistance to radioactive iodine (15 –18). Not limited only to high-risk groups, patients with low and intermediate risk of recurrent disease may exhibit resistance to therapy. These patients more often exhibit nodal metastases, extrathyroidal extension, or aggressive histology (17,19 –22). Nodal disease and extrathyroidal extension are pathologic features previously reported to be associated with more aggressive disease, but because disease burden definitions vary, the literature is complex and varied (23 –28). There is also limited evidence supporting the application of either high- or low-activity radioactive iodine therapy under circumstances where one or both of these features are present and when followed for disease recurrence beyond five years (28 –30). Currently, patients with both extrathyroidal extension and nodal metastases may be considered in the same low-risk group as other patients subsequently offered low-activity radioactive iodine (12). It is unclear if the use of the low-activity radioiodine protocol is appropriate for all low- or intermediate-risk patients.
Further work is required to understand better how the varied application of radioactive iodine influences the risk of recurrence over time frames extending beyond three years. The rate of biochemical progression and rates of structural recurrence were compared in patients with well-differentiated papillary or follicular thyroid carcinomas treated using initial activities above or below 1850 MBq. This cohort, typically exhibiting tumors >1.5 cm and/or adverse pathologic features, were treated before the implementation of the 2009 ATA guidelines. Patients were followed using a standardized protocol for a minimum of five years, with a median follow-up duration of 112 months. These patients, assessed for extrathyroidal extension and nodal metastases, encompass low- and intermediate-risk disease at the time of diagnosis.
Methods
Patient population
The inclusion criteria were: consecutive, newly diagnosed differentiated thyroid cancer referred to the Cross Cancer Institute; treated with a total or near total thyroidectomy; confirmed pathologic findings of a differentiated thyroid cancer, either papillary or follicular carcinoma; absence of distant metastases at the time of diagnosis; staging including a minimum of a neck ultrasound and measurements of thyrotropin (TSH) and thyroglobulin (Tg) at baseline; and followed for a minimum of five years after treatment was completed. Patients with oncocytic or Hürthle cell carcinoma were included. Patients were followed at the Cross Cancer Institute, at a minimum, with yearly bloodwork including TSH, Tg, and antithyroglobulin antibody levels. Ultrasound was completed within one year of surgery with a diagnostic 131I whole-body scan followed by assessments every two years, at a minimum. Stimulated Tg testing was typically accomplished with thyrotropin alpha. If thyrotropin alpha was not available, patients withdrew their levothyroxine prior to the diagnostic scan. In this cohort, recurrence was defined through serial clinical examinations, neck ultrasound scanning, and measurement of stimulated and unstimulated Tg levels whether by hormone withdrawal or Thyrogen stimulation. Patients had whole-body post-therapy scans, and a small fraction of patients were also evaluated with [18F]2-fluoro-2-deoxy-d-glucose positron emission tomography (PET)/computed tomography (CT) to localize the site of disease recurrence. In the event that an elevated Tg was identified or there was clinical evidence of recurrence in the thyroid bed or neck (on ultrasound or 131I whole-body scan), patients were referred for further surgical consideration. The extent of surgery was determined by the treating physician and ranged from an excisional biopsy to a lymph node dissection. From 1995 to 2008, there were 1067 new patient diagnoses of thyroid carcinoma that were screened for the analysis. Within this group, 219 patients were identified with thyroid carcinoma who underwent a total or near total thyroidectomy followed for at least five years (median 112.5 months; range 60–286 months) with intervals not exceeding one year. Of this group, 145 patients had nodal sampling in the form of level 6 lymph node dissections or selective neck dissections. Of the other 848 patients screened from the analysis, 26% presented with tumor volumes <1.5 cm who were not followed, and 53% did not have follow-up for the entire period or lacked one or more of the more required assessments of Tg level or neck imaging. The remaining 21% had significant residual thyroid remnants requiring multiple ablative attempts or persistent structural disease (identified by whole-body iodine scans, ultrasound, or CT scans), presented with distant disease, had a strong family history of thyroid cancer, or moved away and could not be contacted. Five percent of patients received adjuvant external-beam radiotherapy.
Treatment
The decision to treat with radioactive iodine was determined by a multidisciplinary team consisting of surgeons, endocrinologists, and radiation oncologists and administered with the patient's consent. Preparation for radioactive iodine treatment with TSH stimulation was completed either with thyroid hormone withdrawal or with recombinant human TSH (thyrotropin alpha). Cross Cancer Institute guidelines recommended 1110–1850 MBq for patients considered to have low-risk disease and 1850–5550 MBq for patients with intermediate-risk thyroid cancer, but individual doses were all prescribed at the discretion of the individual physicians (n = 7). Patients treated using thyrotropin alpha (n = 36) were given a reconstituted injection of 0.9 mg/mL intramuscularly followed by a second injection 24 hours later. Those who were treated using thyroid hormone withdrawal (n = 183) typically discontinued their levothyroxine treatment for a minimum of 28 days with 14 days of cytomel before its cessation. A low-iodine diet was followed for one week prior to treatment. 131I was administered when serum TSH was ≥30 mIU/L. TSH, Tg, and antithyroglobulin antibody levels were measured prior to radioactive iodine administration. Within one week after radioactive iodine treatment, patients had a 131I whole-body scan. Utilization of external-beam radiotherapy was generally used for macroscopic disease extension. However, the final decision on radiotherapy was at the discretion of the treating physician. Subsequent radioactive iodine was recommended to patients with pathologic confirmation of a recurrence in the neck or thyroid bed; biochemical recurrence ± structural evidence of recurrence; or iodine uptake at a distant site as determined by expert radiologists.
Outcomes
The main endpoint of this analysis was to determine time to recurrence defined clinically as increased Tg level (minimum >0.4 μg/L for unstimulated serum test or >2.0 μg/L for stimulated test) and/or appearance of novel structural disease. Following total thyroidectomy, patients with persistent structural disease following initial radioactive iodine ablation, or with biochemical incomplete responses, were not included in the analysis. Locoregional recurrence was defined as recurrence within the tumor bed or neck, as defined by new sites of disease identified by whole-body iodine scans, ultrasound, or CT scans. Distant metastases referred to recurrences outside of the neck region. Time to recurrence was determined from the date of diagnosis to the date of recurrence, either by pathologic confirmation or biochemical recurrence. Patients lacking evidence of nodal metastases radiographically or pathologically were deemed N0. Overall survival and progression-free survival were calculated from date of diagnosis to date of death or date of recurrence, respectively. Patients were stratified by initial radioactive iodine activity, cumulative radioactive iodine activity, and by the ATA guidelines criteria.
Statistical analysis
Descriptive statistics were presented for the study variables. Means and standard deviations were reported for continuous variables; frequencies and proportions were reported for categorical variables. Independent t-tests were used to compare the mean values for total radioactive iodine activity applied; chi square tests were used to compare two categorical variables. Analysis of variance was used to compare the continuous variables with more than two groups. Recurrence-free survival was calculated from the day of treatment to the day of documented disease progression or recurrence. The logistic regression model was completed using 131I quantity as the dependent variable adjusting for extrathyroidal extension, tumor stage, and nodal disease. Any patient who did not have an event was censored for the survival analyses. Kaplan–Meier estimates were obtained and presented along with their confidence intervals (CI). Log-rank tests were used to compare the survival curves. Binary logistic regression was used to determine the factors associated with recurrence (yes vs. no) and location of recurrence (local vs. neck) as the response variable. SPSS Statistics for Windows v15 (SPSS, Inc., Chicago, IL) was used to conduct all statistical tests. A p-value of <0.05 was used for statistical significance.
Results
Patient characteristics
This cohort of thyroid cancer patients was followed from diagnosis for a median of 112.5 months (range 60–286 months). As expected, the cohort was predominantly female, and there were no variations with respect to patient age, tumor size, focality, or the presence of lymphatic invasion between the two patient groups. The median age at diagnosis was approximately 44 years. The initial analysis and basic demographics as a function of recurrent disease are provided in Table 1. Median tumor size was approximately 2.6 cm (range 1.0–10.5 cm), and 46% of patients had lymph node metastases pathologically demonstrated (Table 1). Forty-two percent of the cohort underwent radioactive iodine treatment using activities <1850 MBq, with the lowest at 751 MBq. Both extrathyroidal extension and nodal metastases were associated, on univariate analysis, with increased risk of recurrence (Table 1). Patient location in a rural center did not appear to influence disease recurrence, consistent with the defined follow-up protocol. Recurrences in 89 patients included the thyroid bed (n = 16), lymphatic disease (n = 74), and distant metastases (n = 7). Following initial radioactive iodine therapy, 54% had a complete response, with undetectable Tg levels, 32% had biochemical disease, with a Tg <2 ng/mL; and 14% had Tg levels whose nadir exceeded 2 ng/mL. Patients with recurrent disease identified by Tg increase, whole-body scan, ultrasound, or PET scans were treated with radioactive iodine in 95% of cases, with 40% receiving more than one treatment. Following the initial ablation, 3.1% of patients exhibited thyroid remnants, 13% had nodal uptake, and one patient exhibited potentially distant disease. Surgery was the sole treatment in 6% of cases, and overall 25% of recurrences had focused or formal neck dissections. Table 2 outlines radioactive iodine treatment and recurrences based on TNM staging. T3/4 tumors, compared to T1/2 disease with or without nodal metastases, were more likely to exhibit remnant disease (p = 0.022). However, this was not linked to disease recurrence overall (p = 0.29). There was a broad range of total average radioactive iodine activities, even within similar histopathological groups, reflecting the significantly increased number of ablations for larger tumors (p = 0.034). The differences are also linked to varying physician preferences spanning 14 years and a previous aggressive approach to achieve athyroglobulinemia for patients treated prior to 2002 (Table 2). For biochemical disease in patients lacking nodal metastases at diagnosis, approximately 24% of patients did recur, while 6/10 patients with nodal disease exhibited a recurrence (p < 0.0001). For structural recurrences, patients with disease in the lateral neck compartments were much more likely to have a recurrence than patients with disease in the thyroid or central compartment (p < 0.0001). In addition, structural recurrences in the cohort were significantly more common with extrathyroidal extension (p = 0.014). It was found that the initial treatment 131I activity was not linked with tumor size or nodal status, but the overall cumulative application of 131I was increased for nodal disease (p < 0.001). Extrathyroidal extension was linked to primary tumor size >4 cm (p = 0.0005), as well as to structural recurrence (p < 0.0001), but not to nodal status (p = 0.40). PET scans were used to document disease in a small number of patients (11%) following progression after radioactive iodine, with the majority of positive scans (75%) associated with non-iodine avid disease.
Disease-free survival
Patients with recurrent disease were much more likely to exhibit extrathyroidal extension or nodal metastases at diagnosis (Table 1). Overall, nearly two-thirds of all biochemical and/or structural disease recurrence occurred within 40 months of initial diagnosis. In light of the fact that the application of radioactive iodine is often driven by the presence or absence of metastases, an analysis was completed of disease recurrence as a function of nodal status, as identified in Figure 1. As expected, the recurrence rate for disease lacking nodal metastases, even for larger tumors, is <20% at five years. Patients with nodal metastases were much more likely to have biochemical or structural recurrences, with nearly 50% recurring five years following initial diagnosis. In the cohort, disease-free survival was dependent on the presence of extrathyroidal extension (p = 0.0007) or nodal metastases (p < 0.0001), as documented in Figures 2 and 3, respectively. The presence of lymph node metastases, with a median recurrence-free survival time of 66 months, appeared to generate a slightly worse prognosis than those patients with extrathyroidal extension (median recurrence-free survival time 77 months). If patients had both extrathyroidal extension and nodal metastases, the median recurrence-free survival time decreased further to 61 months. Lastly, for patients lacking any adverse pathologic features, the median time to recur was ≥144 months. It was noted that the presence or absence of extrathyroidal extension or nodal metastases did not predict the site of recurrence (thyroid bed vs. cervical lymph nodes). However, females were more likely to have a recurrence in the tumor bed as opposed to the cervical lymph nodes (88% vs. 65%; p = 0.046). Multifocal tumors were also more likely to recur within the tumor bed rather than the neck (75% vs. 48%; p = 0.030). On multivariate analysis, female patients were four times more likely to have a recurrence in the thyroid bed (hazard ratio [HR] = 4.08 [CI 1.04–16.05]), and patients who received 1850 MBq for their initial ablative activity were six times more likely to have a recurrence in the thyroid bed (HR = 6.30 [CI 1.30–30.55]).
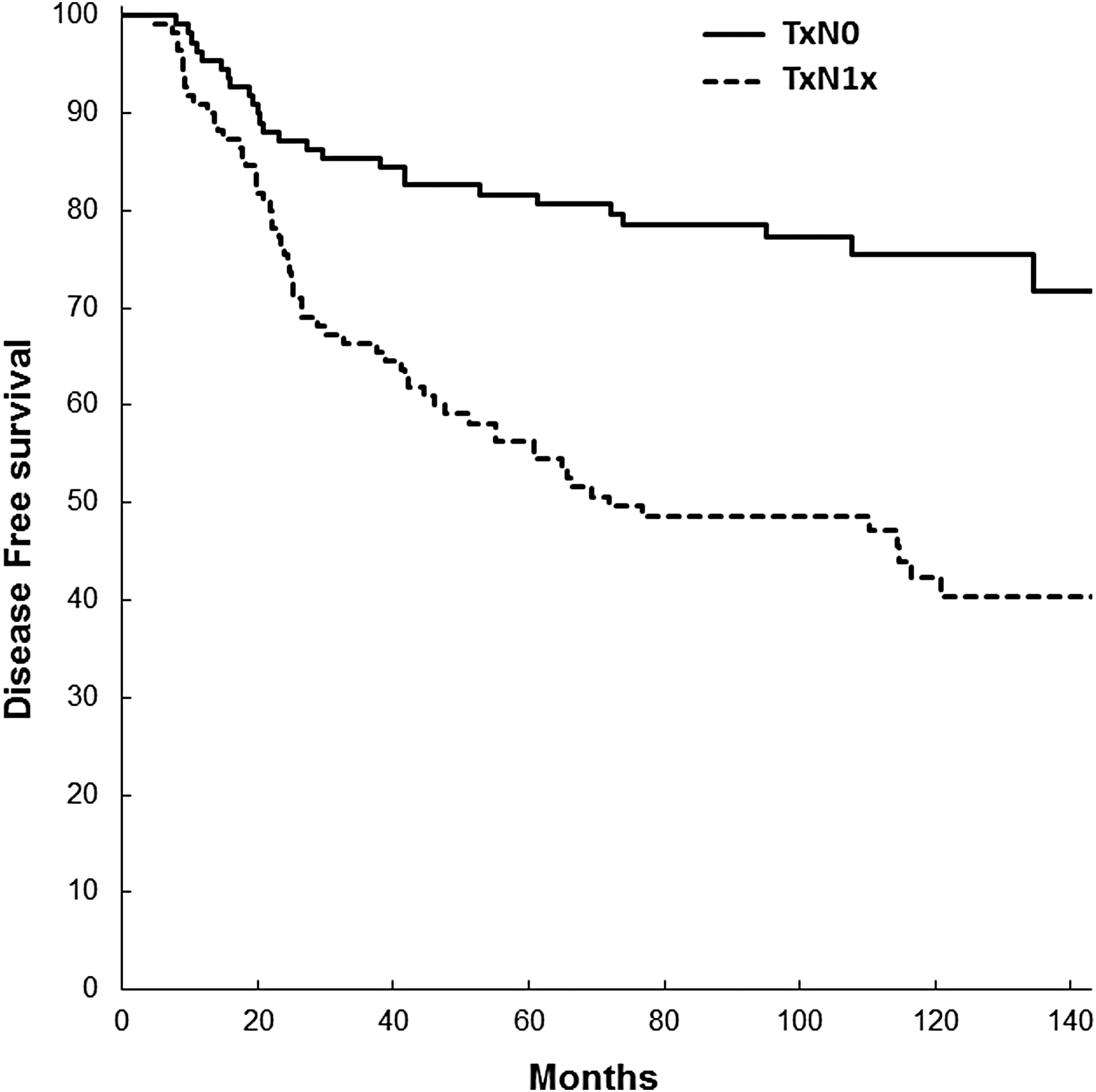
Disease-free survival based on nodal status on presentation.
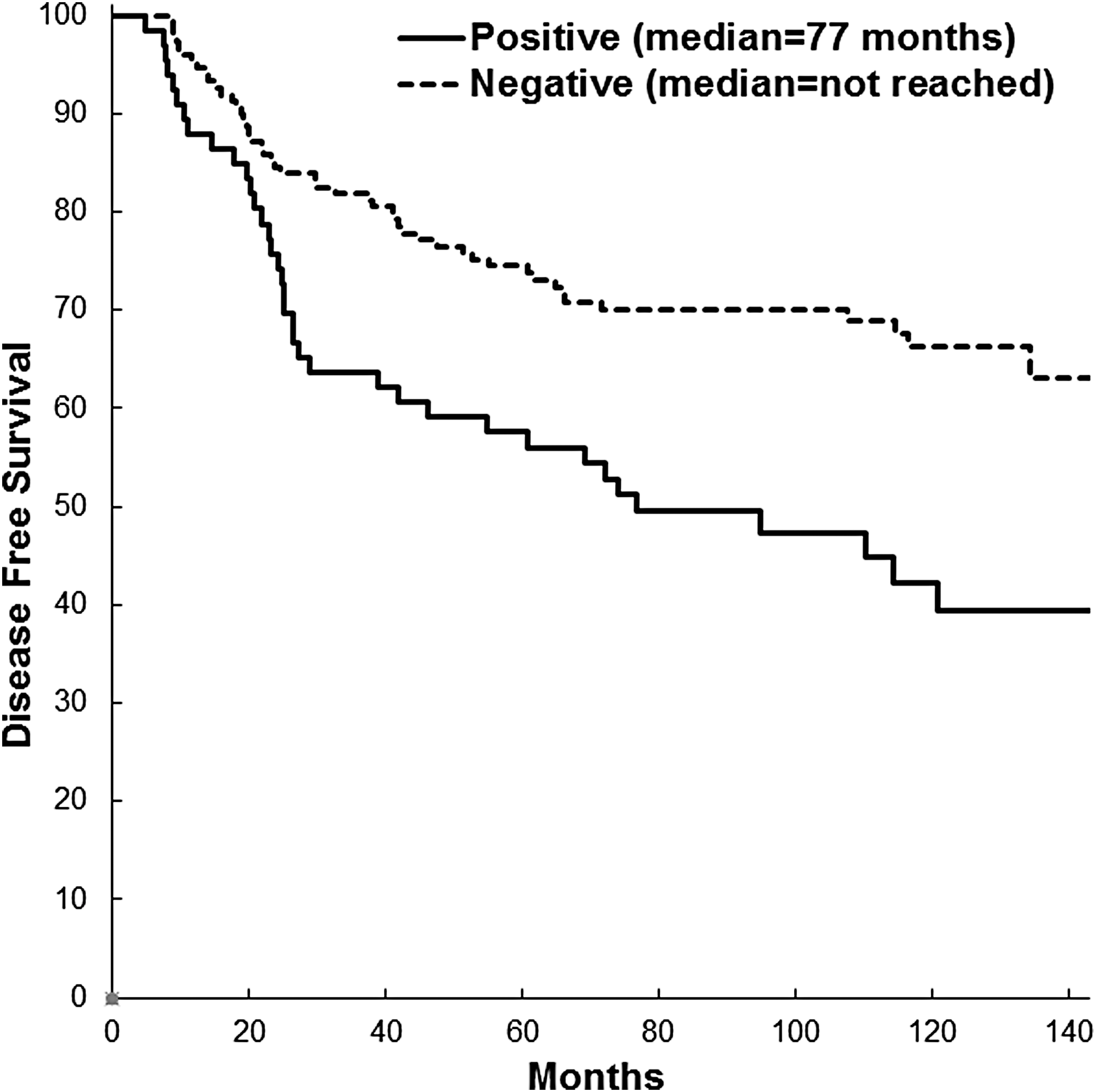
Impact of extrathyroidal extension on disease-free survival. Extrathyroidal extension negatively impacted disease-free survival (p = 0.0007).
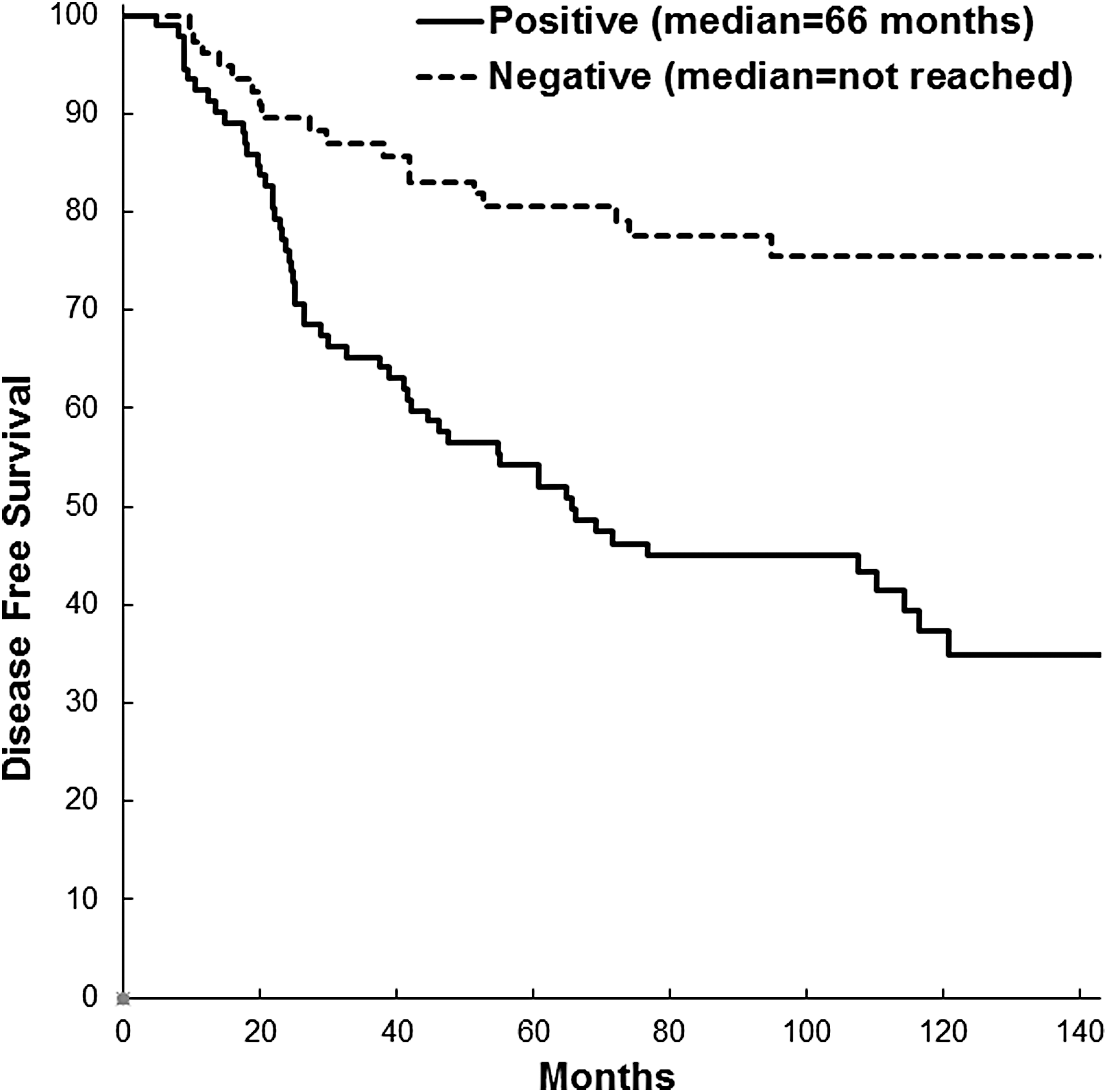
Impact of nodal metastases on disease-free survival. Presence of lymph node metastases negatively impacted disease-free survival (p < 0.0001).
Impact of initial radioactive iodine treatment activity on disease recurrence
While none of the patients in this cohort exhibited high-risk disease based on the exclusion criteria, there were a number of patients with extrathyroidal extension or lymph node metastases who were treated at the physician's discretion with activities above and below 1850 MBq, with the lowest at 1110 MBq. The impact of the initial radioactive iodine treatment activity on disease recurrence was examined in these patient groups. In patients with neither extrathyroidal extension nor nodal metastases at diagnosis, there was no difference in the recurrence-free survival, with variations in the initial ablative activity (Fig. 4; p = 0.57). Patients exhibiting nodal metastases at diagnosis demonstrated minimal difference in disease-free survival, with varying activities of radioactive iodine (Fig. 5). The application of lower-activity 131I in patients exhibiting extrathyroidal extension did lead to more recurrences over an earlier time frame than patients receiving higher 131I activities, but the trend was not significant (Fig. 6). However, in patients with both extrathyroidal extension and nodal metastases, there was a dramatic difference in disease recurrence, depending on the initial ablative activity (Fig. 7). The median recurrence-free survival time for patients treated with a lower activity of radiation was approximately 25 months compared to 121 months for those patients who received a higher initial ablative activity (p = 0.0061).
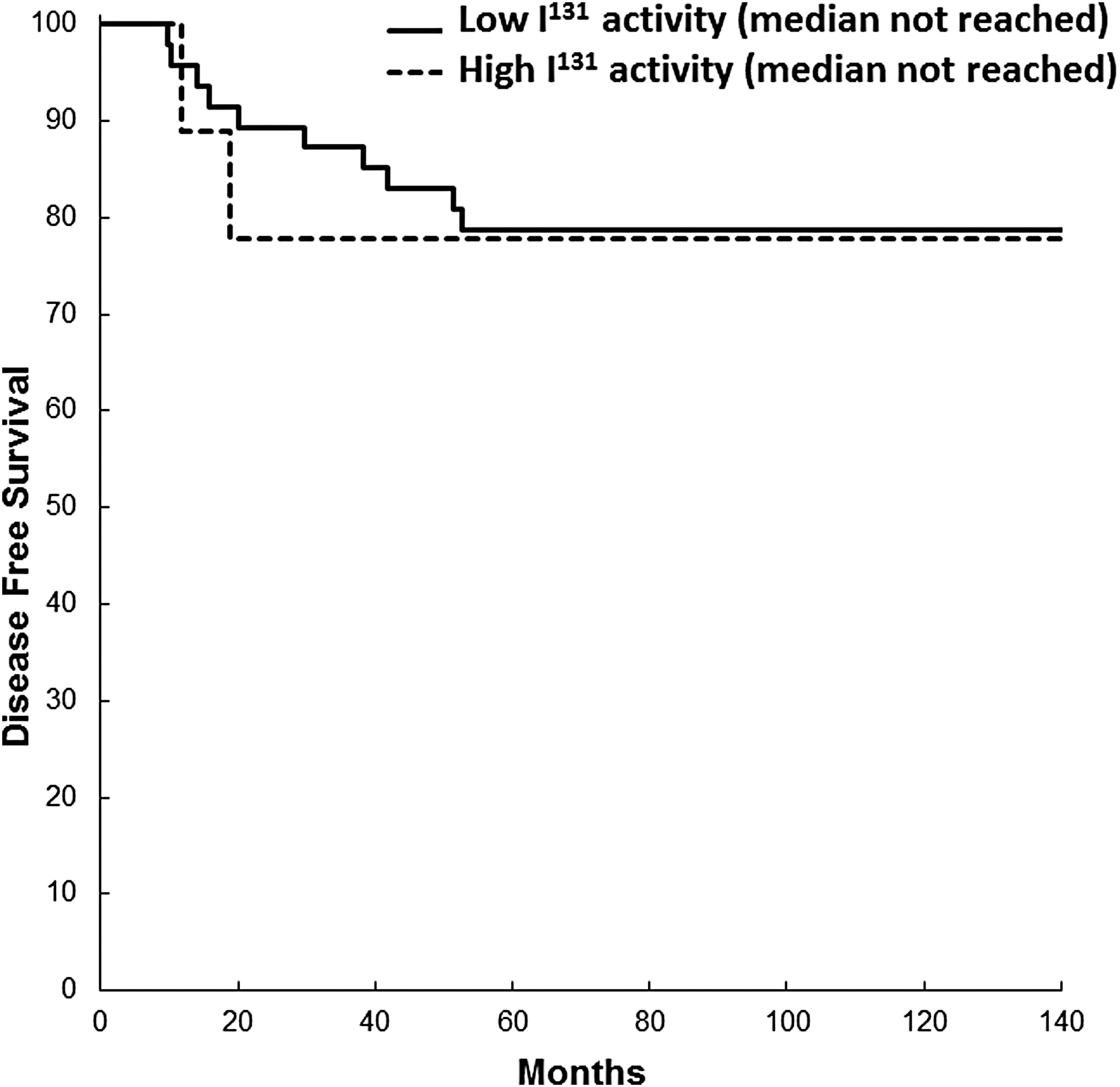
Initial 131I activity did not impact disease-free survival when neither extrathyroidal extension nor lymph node metastases was present (p = 0.57).
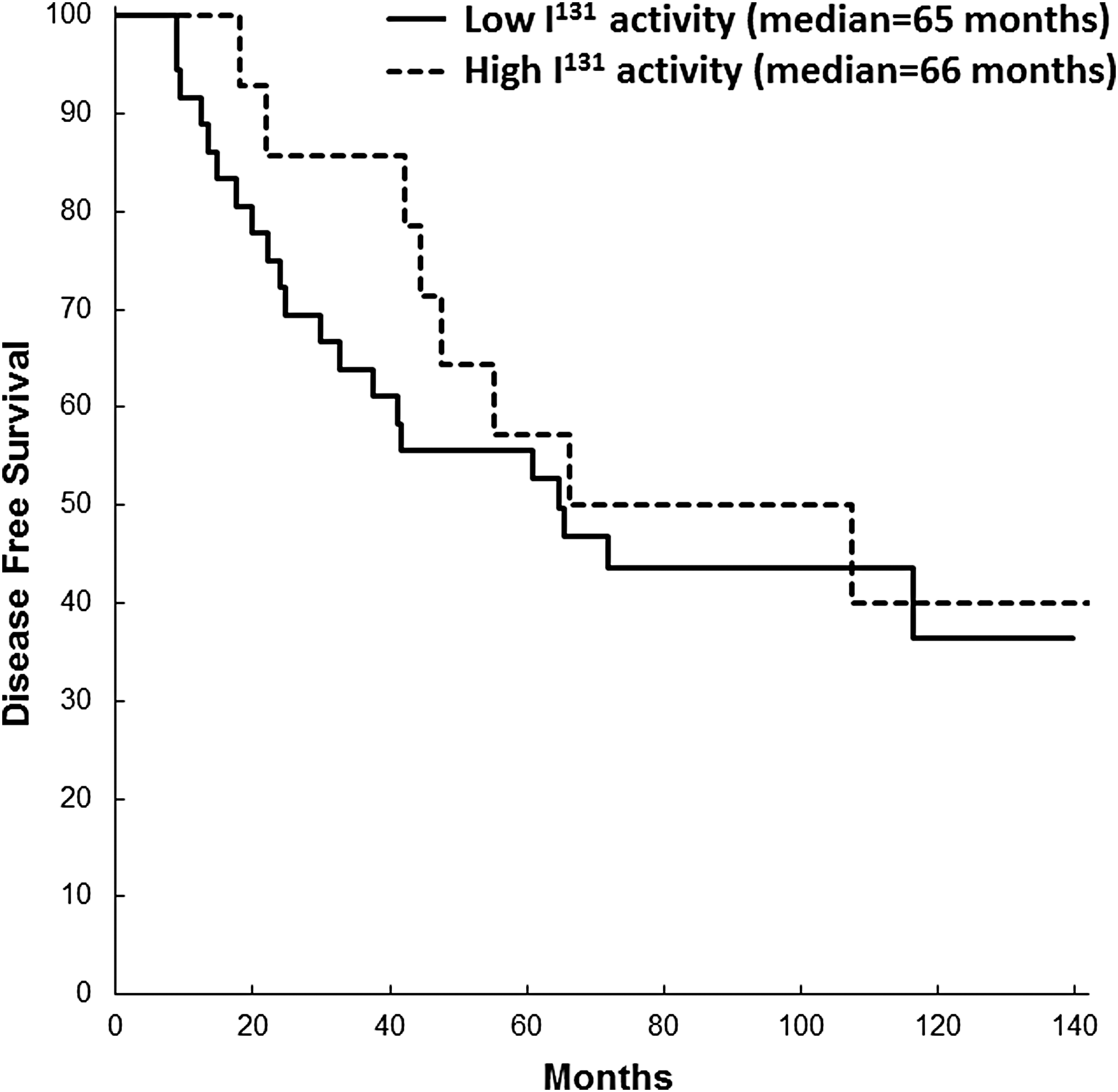
Disease-free survival was not affected by initial 131I activity in patients whose only risk factor was lymph node metastases (p = 0.53).
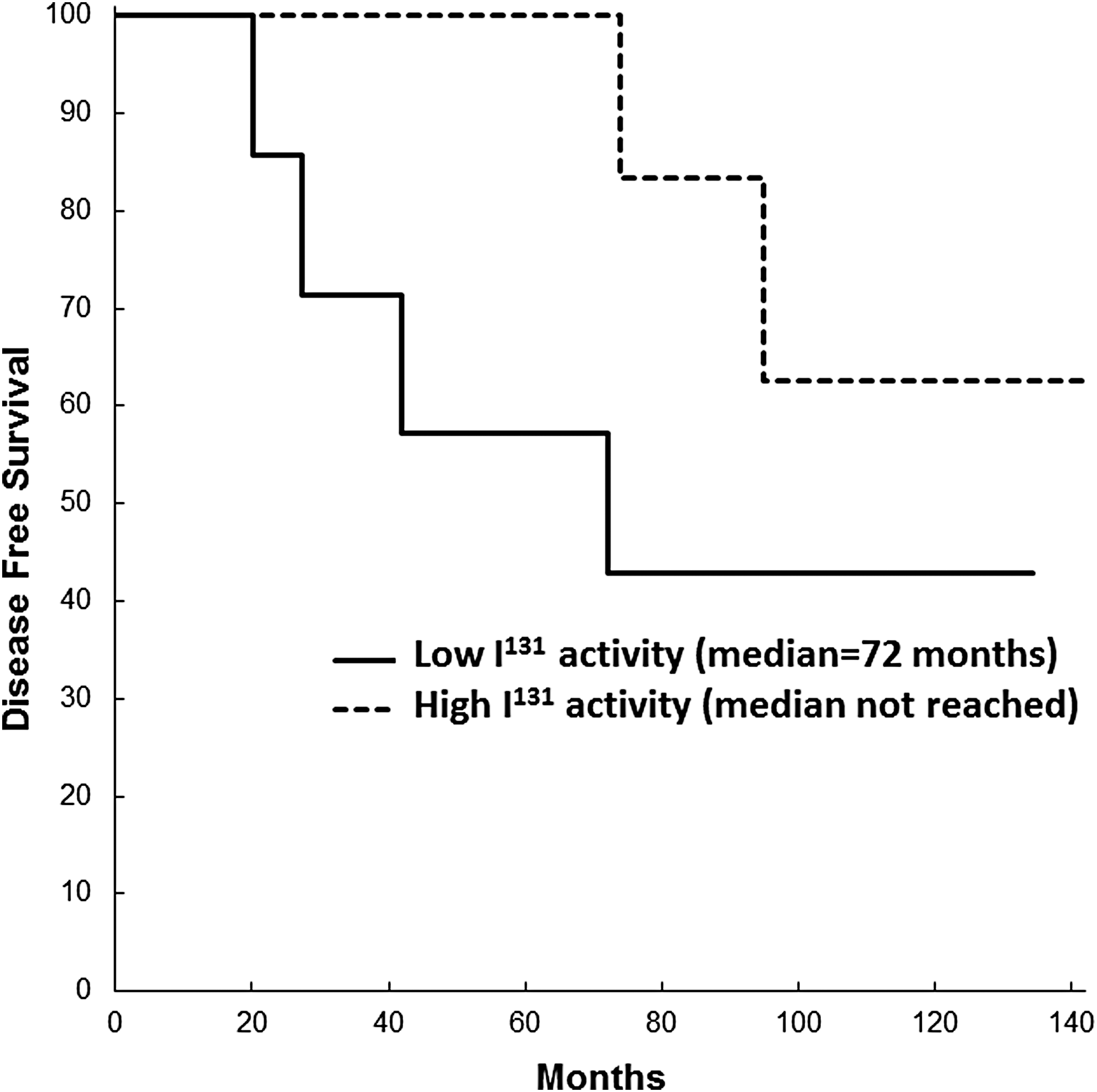
Disease-free survival was not significantly altered with varied initial 131I activity in patients whose only risk factor was extrathyroidal extension (p = 0.20).
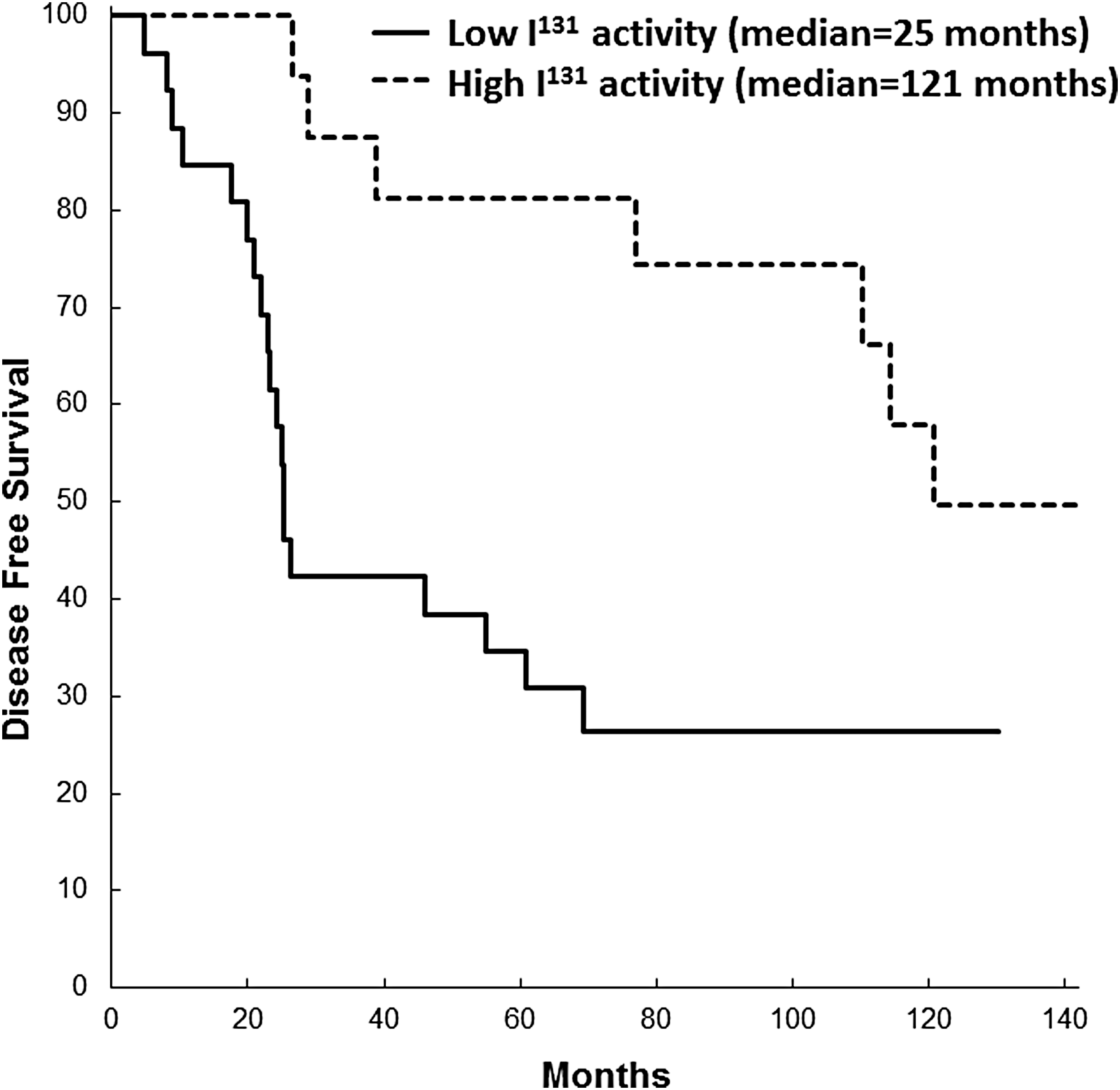
Disease-free survival depends strongly on the initial applied 131I activity when patients exhibit both extrathyroidal extension and lymph node metastases (p = 0.0061).
Discussion
In a patient cohort defined by regular follow-up of no less than five years and up to 20 years, the use of initial radioactive iodine treatments of more or less than 1850 MBq on patient outcomes were compared with respect to pathologic risk factors, including extrathyroidal extension and nodal metastases. In contrast to previous studies, the focus was on recurrence and disease-free survival as an endpoint rather than on ablation success. When patients with both of these risk factors were subjected to varying activities of ablative radiation, a striking difference in recurrence rates was observed. Patients treated with at least 1850 MBq radioactive iodine exhibited much longer disease-free survival compared to patients with both extrathyroidal extension and nodal metastases who received lower activities. The use of low-activity radioactive iodine therapy in patients having both extrathyroidal extension and nodal metastases thus created a marked disparity in recurrence rates, with more than half of the recurrences in the group receiving low-activity radioactive iodine therapy occurring within 24 months of their initial diagnosis. Interestingly, an initial activity of 1110 MBq was also a negative prognostic factor for recurrence locally in the tumor bed (HR = 6.30 [CI 1.30–30.55]). It is important to note that the use of low-activity radioactive iodine therapy did not impact recurrence rates for patients lacking either of these adverse pathological features, even over a follow-up period >10 years. This work supports the use of lower activities of radioactive iodine in the initial postoperative therapy for patients lacking adverse pathologic features. However, a higher activity of radioactive iodine may benefit patients who exhibit both extrathyroidal extension and nodal metastases.
It is well documented that recurrences from thyroid cancer can span decades. While there have been a number of studies examining the utility of high- versus low-activity treatment, there are few studies that examine how this impacts disease recurrence over time frames exceeding five years (31). Kukulska et al. did not observe a significant difference in recurrence rates for low-risk differentiated thyroid cancer over a median follow-up time of approximately six years, examining ablation rates between 30 and 100 mCi (28). However, the analysis was confounded by the fact that patients with a lower initial activity of radioactive iodine were more likely to require a second treatment to complete the ablation (28). Kruijff et al. examined patients ablated with higher- or lower-activity radioactive iodine treatments and did not observe a significant variation in disease-free survival, but in this series, pathologic features were not separately assessed (32). The mixed evidence for decreased recurrence and variations in the application of radioactive iodine for low- and intermediate-risk patients is due to the fact that most studies did not stratify based on pathologic risk features. In the present analysis, initially differences in disease recurrence were not observed when variables such as lymph node dissection or tumor size were considered, similar to previous studies. However, stratifying patients based on the presence or absence of extrathyroidal extension and/or nodal metastases did demonstrate the divergent natural history of recurrence when comparing low- and high-activity radioactive iodine ablation. This may account, in part, for variations in the previous studies examining disease recurrence and variations in the application of radioactive iodine treatment (9,33).
This work indicates that the presence of both extrathyroidal extension and nodal metastases are associated with disease recurrence when only low levels of radioactive iodine are initially employed. Nodal metastases and extrathyroidal extension are both well-established pathologic markers of aggressive disease that are linked to recurrent disease (19 –21). For both of these pathologic features, the spectrum of disease is difficult to define, given the varying definitions of minimal or extensive disease burden. Moreover, very few studies have examined how variations in the application of radioactive iodine influence disease recurrence when examining patients with one or both of these adverse pathologic features. Minimal extrathyroidal extension was included in order to be inclusive in the analysis, as well as to acknowledge the fact that its presence is linked with other adverse features, namely nodal metastases. Individually, these pathologic features did not appear to drive significant differences in disease recurrence, generally consistent with the previous literature (34). However, the presence of both adverse features predicts early recurrence, and quantification of extrathyroidal extension and nodal metastases may be useful in the selective application of radioactive iodine for patients deemed as otherwise having a low or intermediate risk of recurrence. This work also potentially supports a strategy of dosimetry-based high-activity 131I therapy to address tumors with a high risk of recurrence (35,36). Further studies examining variations in the application of radioactive iodine for biochemical or structural recurrences are also needed to avoid over-treating patients who would otherwise not have been materially impacted by the disease, despite elevated biochemical levels of Tg.
This cohort represents one of the largest of all previous studies examining disease-free survival as a function of radioactive iodine ablative activity in well-differentiated thyroid cancer patients followed beyond five years. The limitations of the current study include the fact that it is a retrospective analysis and that the first decision for the radioactive iodine treatment was at the discretion of the treating physician. The application of radioactive iodine was highly variable, in some cases reflecting the fact that many physicians were pursuing athyroglobulinemia and used much higher activities than currently accepted. It is also recognized that there is a treatment and selection bias in this retrospective sampling. The patients had larger tumors, more nodal metastases, and adverse pathological features in excess of many cohorts examining disease recurrence (37,38). However, all thyroid cancer patients referred to this site for risk stratification use a standardized regime for stimulated testing and assessments for biochemical and structural recurrence. Equally important, the varied application of radiation within this group, even for patients with similar pathologic features, is what allowed the varying natural history of disease recurrence to be identified in the face of adverse pathological features, including extrathyroidal extension and nodal metastases. This was strengthened by increased stringent in the application of the criteria with defined follow-up such that the natural history of disease was similarly mapped for all patients within the study. The initial application of radioactive iodine was completed within 90 days after surgery, again avoiding variations in the timing of radioactive iodine, which can influence disease recurrence and survival (39).
The study supports a risk-stratification protocol where a higher activity of radioactive iodine treatment is favored when both extrathyroidal extension and nodal metastases are present in patients with low- and intermediate-risk differentiated thyroid carcinomas. The lack of these features allows the use of low-activity ablative strategies with excellent outcomes that likely reduce the risk of complications secondary to radioactive iodine treatment.
Footnotes
Acknowledgments
This study was supported by The University of Alberta Department of Surgery.
Author Disclosure Statement
T.McM. has received unrestricted research funds from Genzyme and an educational grant from Novartis. No competing financial interests exist for the remaining authors.