
Abstract

Graves' disease (GD), an autoimmune thyroid disorder that leads to hyperthyroidism, can result in significant morbidity for patients. Once the diagnosis of GD has been established, three modalities of therapy for initial treatment are available: antithyroid drugs (ATDs), radioactive iodine (RAI), or surgery. As no definitive pathway for treatment exists and the optimal therapeutic regimen is based on multiple disease and patient factors (such as the presence of Graves' ophthalmopathy (GO), there is great geographic variability in treatment strategies (1).
It appears that this variability in approach to therapy extends to the decision for referral for surgical management. In a study of 48 patients in New York City, Weber et al. found that the leading indication for surgical referral was failed medical management (2). In two other reports, one from Australia and the other from Hong Kong, GO accounted for almost a third of referred patients (3,4).
In light of the publication of the “2016 American Thyroid Association guidelines for diagnosis and management of hyperthyroidism and other causes of thyrotoxicosis” (5), we sought to understand better the primary reason for referral for surgery at our institution in patients with GD. This assessment was pursued to verify that these patterns were in line with guideline recommendations and other surgical series.
A total of 52 patients were referred for surgical management of GD from 2013 to 2015. A retrospective review of the documentation from the primary surgeon and the patients' endocrinologists revealed primary and secondary reasons for referral (Fig. 1). In our cohort, GO was the unequivocal leading indication for surgery (58% of patients). The frequency of this indication represents a dramatic departure from other studies. As noted above, other series report only about a third of referrals for GO. The precise explanation(s) for this difference is being further investigated in our system.
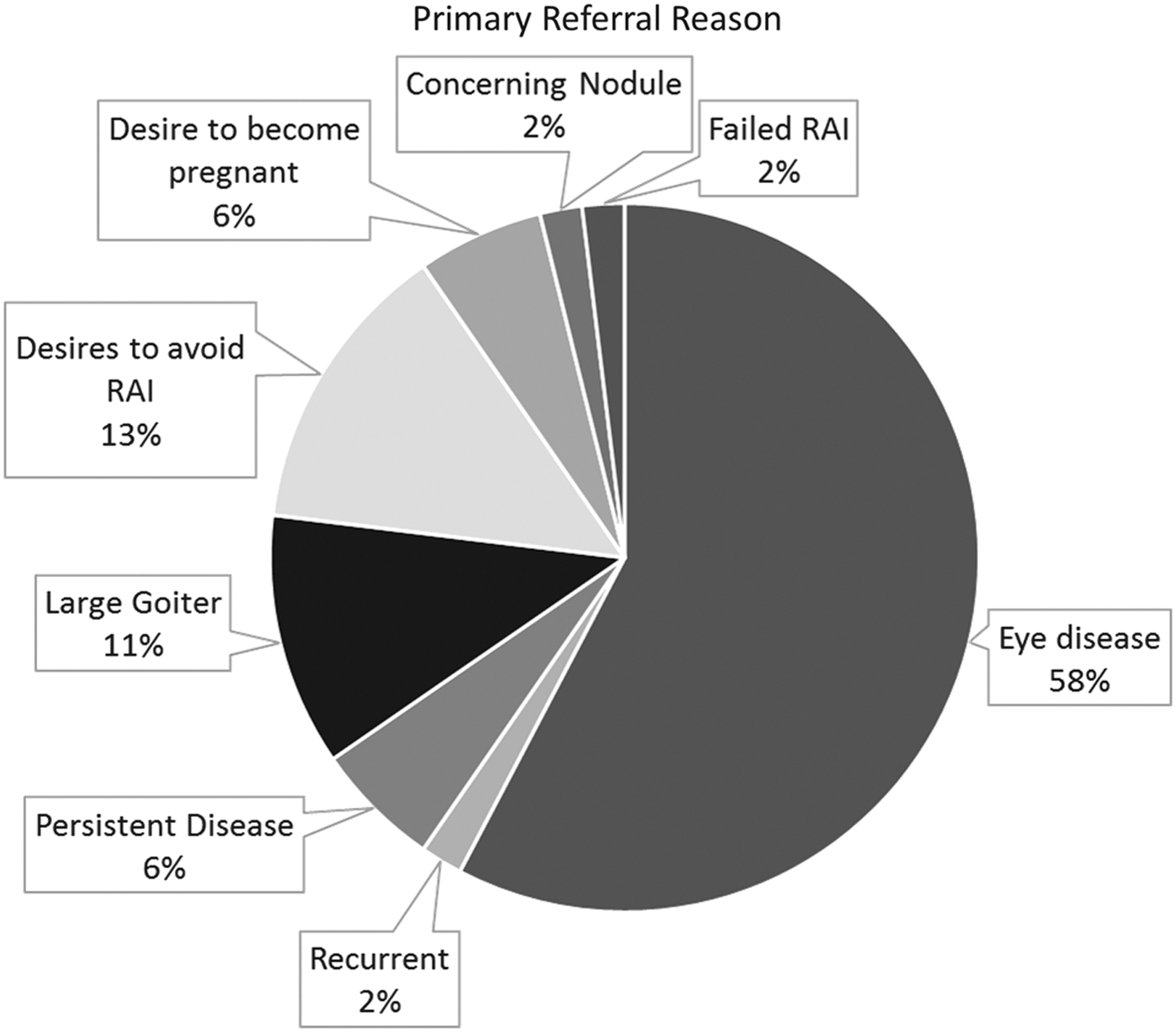
This graph represents the primary reason of referral given by the patient and endocrinologist (n = 52).
Our analysis is consistent with the reported variability that exists in the initial approach to GD. While this divergence may reflect a genuine geographic difference in GD disease patterns and patient preferences, it also likely results from the absence of clear evidence to inform practice guidelines. Further studies of GD are clearly needed to define better the optimal management approach.