
Abstract
Background:
Radiation exposure is a well-known risk factor for thyroid cancer. However, the specific effects of diagnostic radiation exposure on thyroid cancer risk are controversial. The purpose of this study was to perform a systematic review and meta-analysis to assess the effects of diagnostic radiation exposure on thyroid cancer risk.
Methods:
The PubMed and EMBASE databases were searched to identify eligible studies. Summary odds ratio (OR) estimates and confidence intervals (CIs) were used to compute the risk of thyroid cancer using fixed- and random-effects models. Subgroup and sensitivity analyses were performed to evaluate the potential heterogeneity.
Results:
Nine studies from 12 publications were included in the meta-analysis. Overall exposure to diagnostic radiation exposure was associated with a significantly increased thyroid cancer risk (OR = 1.52 [CI 1.13–2.04]). The subgroup and sensitivity analyses revealed similar results. By type of exposure, exposure to computed tomography scans (OR = 1.46 [CI 1.27–1.68]) or dental x-rays (OR = 1.69 [CI 1.17–2.44]) were associated with an increased thyroid cancer risk. Head and neck (OR = 1.31 [CI 1.02–1.69]) and chest (OR = 1.71 [CI 1.09–2.69]) exposure to diagnostic radiation was associated with an increased thyroid cancer risk.
Conclusions:
The results of this meta-analysis indicate that diagnostic radiation exposure is associated with an increased thyroid cancer risk. Therefore, to the extent that it will not compromise the information being sought, radiation exposure to the thyroid should be minimized during diagnostic examinations.
Introduction
T
With the development of diagnostic examinations, early detection and more accurate diagnoses may contribute to reduced morbidity, additional treatment options, and increased life expectancy (8). As the use of radiologic technology has increased, the general population is more likely to be exposed to radiation during various diagnostic procedures (e.g., chest x-rays, dental x-rays, computed tomography [CT] scans, myocardial perfusion scans, positron emission tomography scans) (9,10). Almost every diagnostic examination exposes the recipient to relatively low radiation doses, but there are concerns that increasing exposure to low-dose radiation from repeated diagnostic testing could increase thyroid cancer risk.
Several observational studies have found an association between diagnostic radiation exposure and thyroid cancer risk, but the results of these studies were not consistent. A population-based case-control study revealed that exposure to diagnostic x-rays is associated with an increased risk of thyroid cancer, with the highest risk increase occurring with CT scans (11). The results of a case-control study suggested that exposure to dental x-rays, particularly multiple exposures, may also be associated with an increased risk of thyroid cancer (12).
The precise nature of the effects of exposure to diagnostic radiation on the risk of thyroid cancer is not well documented. Because of the widespread use of radiologic diagnostic examinations, it is important to investigate the extent to which people could be affected by exposure to radiation. A systematic review and meta-analysis were performed to evaluate associations between exposure to diagnostic radiation and thyroid cancer risk.
Materials and Methods
Search strategy
A systematic literature search of the PubMed and EMBASE databases was performed on December 9, 2016, with no time restrictions on publications. The objective was to find studies on exposure to diagnostic radiation and the effects on thyroid cancer risk. The search terms were (screening OR diagnosis OR screen OR examination OR diagnostic) AND (radiation OR radiography OR x-rays OR ionization OR ionizing) AND (“thyroid cancer” OR “thyroid carcinoma”). The reference lists of the selected studies were reviewed, and a manual search was performed to find additional relevant studies.
Inclusion and exclusion criteria
Two authors (M.A.H. and J.H.K.) independently reviewed each study, and any discrepancy was resolved by discussion. A study was included if it met all of the following inclusion criteria: (i) human study; (ii) exposure to diagnostic radiation was defined as an independent variable; (iii) thyroid cancer risk was assessed as an outcome variable; (iv) the entire published text of the study was available; (v) use of the odds ratio (OR), relative risk (RR), hazard ratio (HR), standardized incidence ratio (SIR), and standardized mortality ratio (SMR), with a corresponding confidence interval (CI), or associated risk estimate calculations; and (vi) written in English. Studies were excluded if they were based on cell-level, animal, or modeling studies. Letters, comments, correspondence, conference reports, and laboratory studies were also excluded. When multiple publications were available for the same study subjects, only the most recent publication was included. When more detailed data (such as type of diagnostic procedure or exposure site or other subgroups) were published in an overlapping publication, the information from the overlapping publication in the subgroup analyses was used, but each study was included only once in each analysis.
Data extraction
Two authors (M.A.H. and J.H.K.) independently collected the following information: first author's name, year of publication, study location, study design, number of participants (cases/controls), age range, sex, histological type of thyroid cancer, type of radiologic examination, exposure assessment method (medical records versus self-report), time between first exposure and diagnosis, risk estimates, CIs, and variables adjusted for the analysis. Disagreements were resolved using discussion.
Statistical analyses
Summary estimates were calculated using fixed- and random-effects models. Heterogeneity was evaluated using the Cochrane Q test and I 2 statistics. When individual study estimates are combined, they vary by chance; when excessive variation between studies occurs, it is called statistical heterogeneity. When statistically significant heterogeneity was present (p < 0.05, I 2 > 50%), a random-effects model was used. First, the risk for thyroid cancer from overall exposure to diagnostic radiation was calculated. When examination-specific risk estimates by each radiologic examination were the only results reported (vs. the risk estimate from overall diagnostic radiation exposure) in a single study, the risk estimate based on the most common exposure (e.g., chest x-rays) was used as the representative risk estimate for calculating summary estimates between overall diagnostic radiation exposure and thyroid cancer risk. The thyroid cancer risk by radiologic examination method was then calculated. A sensitivity analysis was performed to evaluate robustness by excluding one study, and the results were assessed to evaluate whether they were substantially influenced by a specific study. Subgroups were investigated to find variability in the pooled risk estimates. Subgroup analyses by body site of exposure, study design, method of exposure assessment, handling of radiation therapy status, and latency period were performed to evaluate heterogeneity. Publication bias was not evaluated because a small number of studies were included in the meta-analysis (13). When risk estimates and CIs were not reported, they were calcu lated from the data included in the article. All data were entered and analyzed using Review Manager v5.3 (The Nordic Cochrane Centre, The Cochrane Collaboration, Copenhagen).
Results
Study selection and general characteristics of included studies
The database and hand searches revealed a total of 8748 studies (PubMed: 3420; EMBASE: 5325; manual search: 3). After duplicate studies (n = 1277) were removed, 7471 remaining studies were screened; of these, 7393 were excluded based on title and/or abstract information. The remaining 78 full-text articles were then assessed for eligibility based on the inclusion criteria. Sixty-six studies were excluded (47 had irrelevant exposures or outcomes or both, six were abstracts only, four were review studies, three were not written in English, two were letters or comments, two did not report risk estimates, one was a pooled analysis, and one was a case report). From the remaining 12 publications (11,12,14 –23), nine were eligible for inclusion in the meta-analysis (Fig. 1).
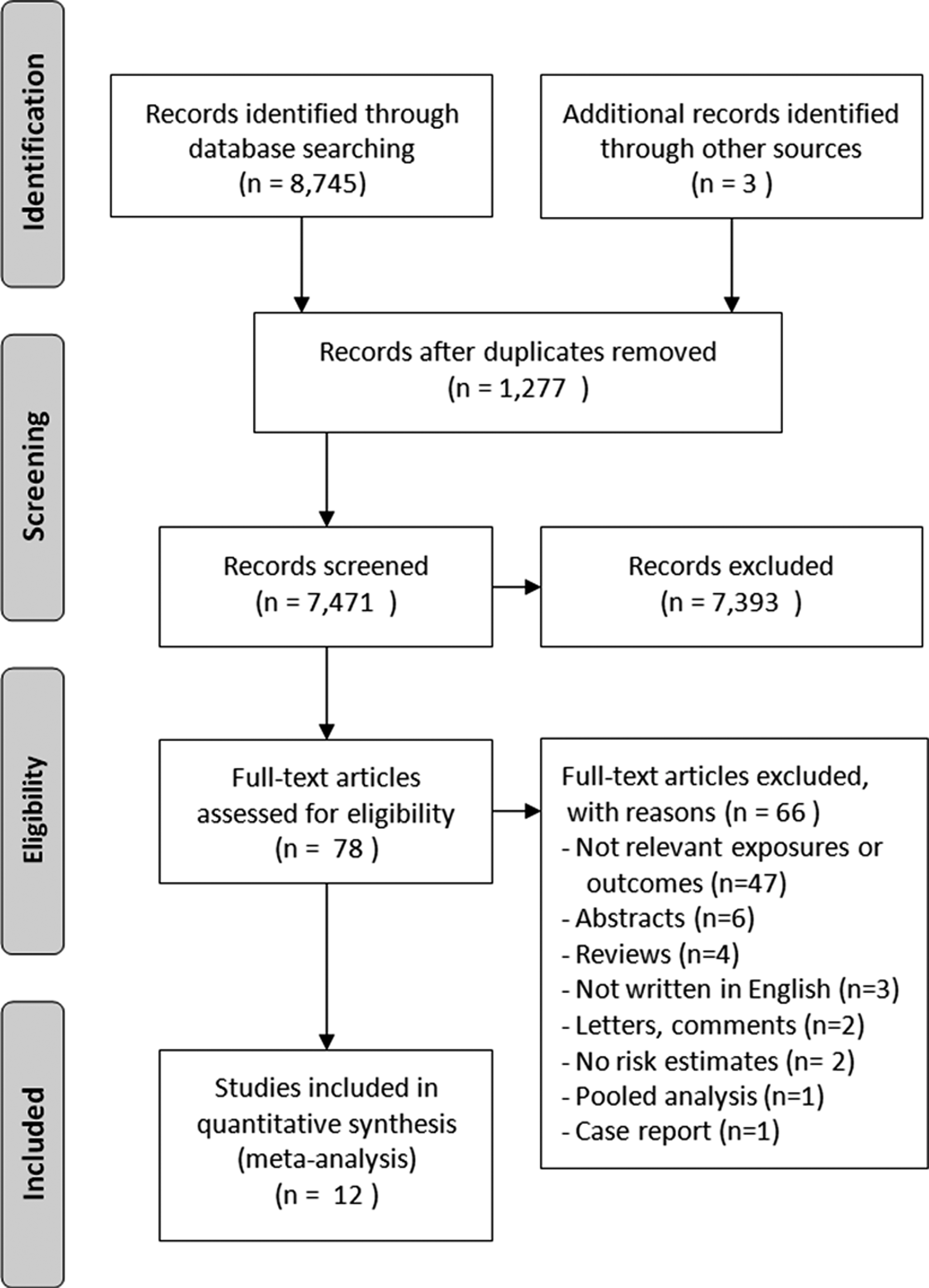
Flow diagram of study selection process.
Two duplicate publications (18,19) were included only in subgroup analyses that included type of exposure and body site of exposure variables because the main article (17) only provided results for overall diagnostic radiation exposure based on the medical record. One publication (21) was included only in the subgroup analysis of dental x-ray exposure because the results of the main publication (20) were used for the main and other subgroup analyses.
Three cohort studies (14 –16) and six case-control studies (11,12,17,20,22,23) were identified. Four studies were performed in the United States (11,15,16,23), one in Australia (14), one in Kuwait (12), and three in Sweden (17,20,22). Two studies included data from females only; nine studies included data from males and females. Two studies used medical records to obtain radiation exposure data (14,16), five studies used self-report (11,12,15,22,23), and two studies used medical records and self-report (17,20). One study excluded subjects who had received radiotherapy (12), two studies reported estimates after adjusting for prior radiotherapy (11,23), and six studies neither excluded nor adjusted for therapeutic radiation exposure history (14 –17,20,22) (Table 1).
ATC, anaplastic thyroid cancer; CI, confidence interval; CT, computed tomography; F, female; FTC, follicular thyroid cancer; GI, gastrointestinal; M, male; MTC, medullary thyroid cancer; NR, not reported; OR, odds ratio; PCCS, population based case-control study; PCS, prospective cohort study; PTC, papillary thyroid cancer; RCS, retrospective cohort study.
Exposure to diagnostic x-ray exposure and thyroid cancer risk
The overall diagnostic x-ray exposure was associated with an increased thyroid cancer risk (OR = 1.52 [CI 1.13–2.04]) with significant heterogeneity (p < 0.001, I 2 = 79.0%; Fig. 2). The results of sensitivity analyses indicated that any single study did not significantly affect the summary estimate, which ranged from 1.43 [CI 1.06–1.93] to 1.61 ([CI 1.08–2.43]; Fig. 3).
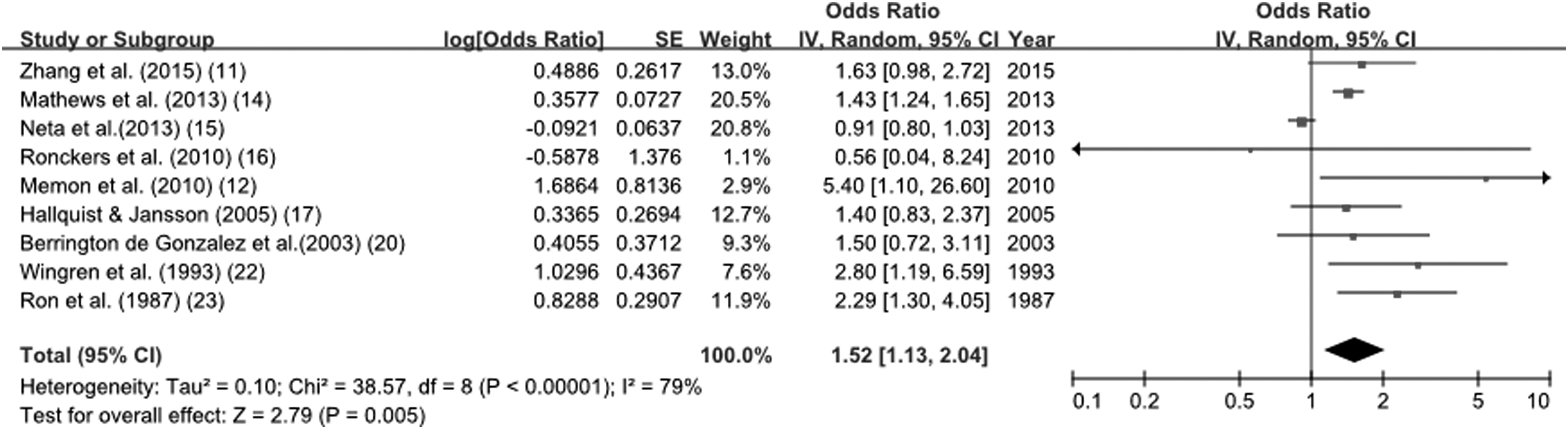
Forest plot of diagnostic radiation exposure and thyroid cancer risk.
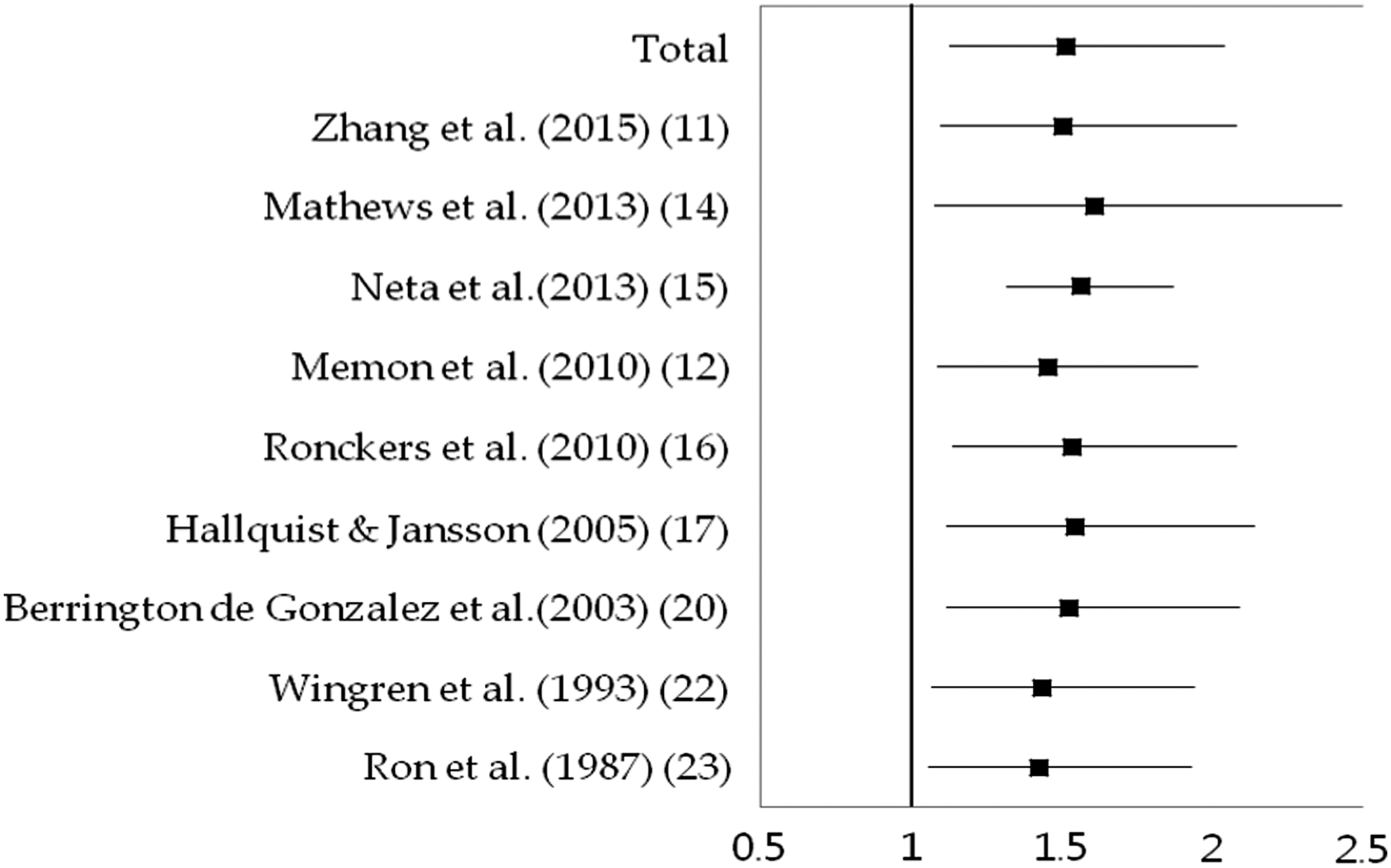
Sensitivity analysis of diagnostic radiation exposure and thyroid cancer risk.
Subgroup analyses were performed using type of radiologic examination, body site of exposure, study design, methods of exposure assessment, handling of radiation therapy status, and latency period subgroups. CT (OR = 1.46 [CI 1.27–1.68]) and dental x-ray (OR = 1.69 [CI 1.17–2.44]) exposures were associated with increased odds of thyroid cancer. The results for chest x-ray and mammography exposures indicated that they were not associated with thyroid cancer risk. Head and neck (OR = 1.31 [CI 1.02–1.69]) and chest (OR = 1.71 [CI 1.09–2.69]) exposure to diagnostic radiation were associated with thyroid cancer outcome, but other body site exposures were not. Analysis of that method of exposure assessment revealed that use of medical records (OR = 1.43 [CI 1.25–1.63]) and self-reporting (OR = 1.65 [CI 1.08–2.54]) were associated with thyroid cancer outcome (Table 2).
Discussion
The individual risk of cancer from a single diagnostic radiation examination is extremely small. However, total exposure to diagnostic radiation has substantially increased over the past decades (9,10). The use of diagnostic radiation may contribute to a precise diagnosis and early treatment, and will likely continue to increase because of physicians' reliance on imaging tests for an accurate diagnosis (10,24). Therefore, assessment of the cancer risk from diagnostic radiation exposure is an important objective. This meta-analysis was used to analyze data from nine studies to evaluate the effects of diagnostic radiation exposure on thyroid cancer risk. The findings reveal that there were significant associations between exposure to diagnostic x-ray exposure (OR = 1.52 [CI 1.13–2.04]) and increased risk of thyroid cancer.
Dental x-ray exposure was associated with an increased thyroid cancer risk (OR = 1.69 [CI 1.17–2.44]). This result was consistent with the results of previous studies that found that dental x-ray exposure is associated with head and neck region cancer (25,26). A meta-analysis that assessed the association between dental x-rays and meningioma risk found that the association was different by dental x-ray type (e.g., bitewing x-ray, panorex x-ray) and that radiation dose varied by type of dental x-ray (27). Most of the articles included in our meta-analysis did not report the type of dental x-ray, so the results of our analysis did not include associations according to x-ray type.
The meta-analysis revealed that radiation exposure of the thyroid associated with a CT exam contributed to thyroid cancer risk (OR = 1.46 [CI 1.27–1.68]). Use of CT exams has markedly increased since 1990 (28), with the head and neck as the most commonly scanned body parts (29,30). A CT scan is a relatively high-dose procedure. The radiation dose absorbed by the thyroid is greater when multiphase CT examination (31) or a CT scan using a contrast medium (32) is performed. A previous study was used to estimate thyroid dose and the associated risk for thyroid cancer from a head and neck CT exam. An absorbed radiation dose range of 15.2–52.0 mGy during a neck CT can increase the risk for thyroid cancer up to 390 cases per million patients (33). Another study was used to estimate thyroid cancer risk from CT scans of pediatric patients. The lifetime attributable risk estimates for thyroid cancer were: head CT, 1.1 cases per 100,000 for boys and 8.7 cases per 100,000 for girls; chest CT scans, 2.1 cases per 100,000 for boys and 14.1 cases per 100,000 for girls (34).
Head and neck (OR = 1.31 [CI 1.02–1.69]) and chest (OR = 1.71 [CI 1.09–2.69]) exposure to diagnostic radiation were associated with an increased risk of thyroid cancer; there were no associations with exposure of other body sites. These body sites are closely associated with the thyroid. Irradiation of these body regions for therapeutic purpose is a well-known risk factor for thyroid cancer (2,35). The present results suggested that exposure of the head/neck and chest areas to diagnostic radiation also increased the risk for thyroid cancer.
The minimum latency period is longer for solid tumors than for hematologic cancers; it ranges from 10 years to many years after the initial radiation exposure (9). Studies have found latency periods of much less than four years for thyroid cancer cases. The incidence of thyroid cancer dramatically increased within four years after the Chernobyl nuclear facility accident (36). According to the U.S. Centers for Disease Control and Prevention, the minimum latency time for thyroid cancer is 2.5 years (37). Not all studies report the time interval between the first exposure and the thyroid cancer diagnosis. However, most studies report more than a five-year latency period. One study did not exclude cases diagnosed with thyroid cancer within five years after exposure, but sensitivity analyses excluding the first five years of follow-up did not materially change the results of the point estimates (15). Recalculation after exclusion of three studies that did not report on latency period produced a similar result (OR = 1.38 [CI 1.02–1.87]).
Exposure to diagnostic radiation was assessed using medical records or self-reporting. Of the studies used for the meta-analysis, two (14,16), five (11,12,15,22,23), and two (17,20) studies assessed radiation exposure using medical records, self-report, or both, respectively. The summary OR for use of medical records (1.43 [CI 1.25–1.63]) was similar to the summary OR for use of self-report (1.65 [CI 1.08–2.54]). Previous studies found disagreement between medical x-ray histories obtained using interview compared to a review of medical records (17,20). The overall discrepancy is low, but the exam-specific discrepancy for the diagnostic radiation exposure is quite large (20). In this meta-analysis, when a study assessed radiation exposure using both medical records and self-report, the study estimates using medical records were usually selected. When assessing diagnostic x-ray as a risk factor for thyroid cancer, it is important to reduce information bias using a prospective design or medical records.
Diagnostic radiation exposure can be a risk factor for cancer; it cannot be assumed that there is a dose threshold at which cancer risk is minimal or non-existent (38). Although the linear non-threshold (LNT) model is still controversial, it is regarded as the most robust and safest model for making decisions about the effects of medical radiation exposure on cancer risk (39). It is recommended that the LNT model be used as the basis of radiation protection (39,40).
Reverse causation might explain the association between diagnostic radiation exposure and cancer risk observed in this study. The early symptoms of undetected cancer, or the medical conditions that predispose an individual to cancer, indicate that diagnostic radiation exams, rather than the radiation dose per se, is the main cause of cancer (41). However, dental x-rays, which are widely used for dental disease screening in the general population, were associated with the risk of thyroid cancer in the current meta-analysis. Further studies investigating the association between these diagnostic exams and radiation dose will help elucidating any causal relationship.
There are some limitations of this meta-analysis. First, the effects of therapeutic radiation exposure were not completely excluded. Two studies excluded study subjects who received radiotherapy or reported risk estimates after adjusting for therapeutic radiation exposure history. However, seven studies did not exclude or adjust or report the therapeutic radiation exposure status. Although subgroup analyses that “excluded subjects who had received RT or adjustment of RT status” showed similar results, this information should be considered during assessments of the effects of diagnostic radiation exposure on thyroid cancer risk. Second, radiation exposure at a younger age has a higher carcinogenic effect than at an older age. Most case-control studies did not report the age at exposure to diagnostic radiation. In addition, general radiation protection equipment (e.g., lead shields) can decrease the radiation burden on the body. Further studies are needed to investigate differences in thyroid cancer risk by age at exposure to diagnostic radiation and the use of protective equipment. Third, several risk estimates based on specific types of radiologic examinations were obtained from this meta-analysis. However, it was difficult to exclude the effects of other types. Among the included studies, only one study (15) calculated study-specific estimates after adjusting for all other diagnostic procedures. Multiple radiologic examinations of the same subject have become increasingly common (29,30). Finally, because a limited number of articles were available for the meta-analysis, the effects of publication bias on the results were not assessed.
To the authors' knowledge, this is the first meta-analysis to investigate the risk of thyroid cancer from diagnostic radiation exposure. This exposure has increased in the last decades. Overall, the results of the meta-analysis revealed that diagnostic radiation exposure was associated with increased thyroid cancer risk. This result was robust to the sensitivity analysis and was not substantially changed by excluding a specific study. Healthcare professionals have a critical role in the appropriate use of diagnostic radiation imaging. While the disadvantages of diagnostic x-rays must be considered, the benefits of diagnostic radiation (e.g., early detection and increases in life expectancy) are not insignificant. During diagnostic procedures, it is imperative to protect the thyroid and reduce radiation doses. Strategies include preferred use of imaging examinations without ionizing radiation, avoiding or reducing thyroid exposure during diagnostic examination, and not using a contrast medium to reduce the absorption of radiation.
Footnotes
Author Disclosure Statement
No competing financial interests exist.