
Abstract
Background:
Thyrotropin (TSH) suppression has improved the clinical outcomes of patients with differentiated thyroid cancer (DTC). However, the efficacy of TSH suppressive therapy (TST) is unclear in patients with low-risk DTC. This study aimed to evaluate the efficacy of TST and optimal TSH levels of patients with low-risk DTC.
Methods:
This retrospective propensity score–matched cohort study included DTC patients (n = 446) who underwent lobectomy from 2002 to 2008 with or without TST (TST group and No-TST group). Disease-free survival (DFS) and dynamic risk stratification were compared between both groups using serum TSH levels.
Results:
Approximately 74% of TST patients and 11% of No-TST patients had suppressed serum TSH levels (<2 mIU/L). The median follow-up period was 8.6 years. During follow-up, the disease recurred in 10 (2.7%) patients, with no significant difference in DFS between the groups (p = 0.63). The proportion of patients with excellent treatment response was similar between the TST (65.2%) and No-TST (64.4%) groups. Incomplete biochemical response was noted in 17.2% of the TST group patients and 9.4% of the No-TST group patients. No significant difference was observed in the DFS between both groups by comparing serum TSH level (p = 0.57).
Conclusions:
TST did not improve clinical outcomes, and serum TSH levels were not associated with recurrence in patients with low-risk small DTC. No clinical benefits were shown for TSH suppression in low-risk patients who underwent lobectomy. Thus, levothyroxine is not necessary for patients without evidence of hypothyroidism.
Introduction
E
The rationale for using TST with levothyroxine (LT4) is based on several clinical and experimental studies (5,6). Cancer cells originating from DTC express the TSH receptor (7,8), and TSH stimulates the proliferation of cancer cells in vitro (9,10). In TST, supra-physiological doses of thyroid hormone may inhibit tumor growth (5,6). TST has been commonly used for patients with DTC to reduce the risk of recurrence of the disease (11,12). More aggressive TST may improve cancer-specific mortality and disease recurrence in high-risk patients (11,13). However, the target level of TSH suppression for patients with low-risk DTC is unclear (4).
Several studies have reported potential adverse effects of long-term TST for subclinical hyperthyroidism associated with the use of supra-physiological doses of thyroid hormone, including an increased risk for thyrotoxicosis, osteoporosis, and cardiovascular disease (14). Therefore, physicians should be cautious when using TST due to the potential risk of adverse effects. The use of aggressive TSH suppression in patients with DTC is controversial, especially for patients with low-risk disease (14). Thus, it is crucial to determine whether TST is beneficial for patients with low-risk DTC, despite the risk of adverse effects.
This study aimed to evaluate the need for TST and the optimal level of TSH suppression in patients with low-risk DTC who underwent lobectomy. The clinical outcomes of patients with or without TST were compared in a propensity score–matched cohort.
Materials and Methods
Patients
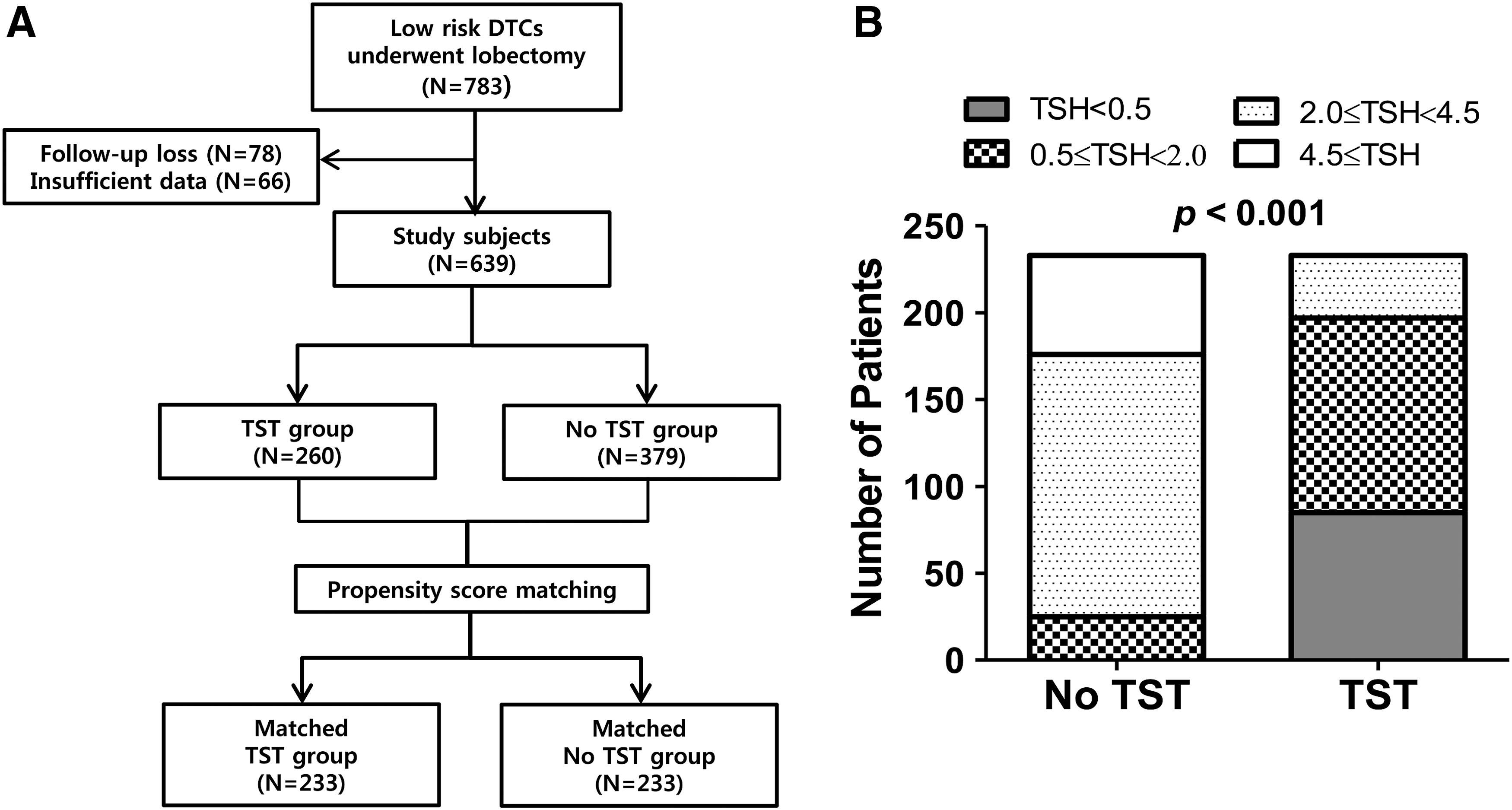
This retrospective, propensity score–matched cohort study screened 1442 consecutive patients with DTC who underwent lobectomy from 2002 to 2008 at the Asan Medical Center (Seoul, Korea). Patients who had an aggressive variant of papillary thyroid cancer or poorly differentiated thyroid cancer were not included. A total of 783 patients with low-risk DTC, as defined by the ATA guidelines (4), were included in this study. Low-risk DTC was defined according to the following criteria: intrathyroidal DTC, tumors <4 cm in size, no extrathyroidal extension, no vascular invasion, no clinical lymph node (LN) metastases, or five or fewer pathological N1 micrometastases (<0.2 cm in their largest dimension). Patients with less than two years of follow-up (n = 78) and patients who had insufficient data to determine dynamic risk stratification (DRS; n = 66) were excluded, leaving 639 eligible patients. Of these, 466 patients were ultimately eligible for propensity score matching in this study (Fig. 1A). This study protocol was approved by the Institutional Review Board of the Asan Medical Center.
(
Initial treatment and follow-up
The Asan Center has an established protocol to ensure that patients with DTC receive consistent treatment and follow-up, as previously described (15 –17). Preoperative neck ultrasonography (US) was performed in all patients to examine the contralateral lobe and cervical LN. If the US indicated the presence of suspicious thyroid nodules in the contralateral lobe or cervical LN metastasis in the lateral neck, US-guided fine-needle aspiration cytology (FNAC) was obtained to examine the lesions prior to thyroid surgery. Prophylactic unilateral central neck dissection (CND) was routinely performed for patients who underwent lobectomy. After the initial surgery, a physical examination and measurement of thyroid function tests were regularly performed every 6–12 months. Some patients underwent TST with LT4; other patients did not receive LT4 during the follow-up period (17). Measurement of stimulated thyroglobulin (Tg) and Tg antibody (TgAb) levels was conducted every six months or yearly, depending on clinical evaluation. Neck US was conducted annually or biannually. A simple chest radiography was performed regularly. The decision for TST after lobectomy was determined by clinical risk factors such as age, sex, tumor size, multifocality, cervical LN metastasis, and preference of the endocrinologist and patients.
The follow-up protocol for patients with low-risk DTC after lobectomy has been reported previously (17,18). Briefly, patients were routinely followed up every 6–12 months for a physical examination and serum free thyroxine (fT4), TSH, Tg, and TgAb measurements. The details of these assays are reported elsewhere (19). Neck US was performed every six months during the first year and repeated every one to two years thereafter.
Definition of serum TSH levels during follow-up
Serum TSH levels were measured multiple times during follow-up. All patients had data for at least three serum TSH measurements; the average number of measurements per patient was 4.62. Because serum TSH levels may occasionally fluctuate, the patients were categorized into four groups using a range of serum TSH: low serum TSH (<0.5 mIU/L), low-normal serum TSH (0.5–1.9 mIU/L), high-normal serum TSH (2.0–4.4 mIU/L), and high serum TSH (≥4.5 mIU/L). Patients were assigned to each group according to the serum TSH level obtained for >75% of their measurements during the follow-up period after thyroid surgery.
Clinical outcomes after DTC treatment
The initial tumor-node-metastasis (TNM) staging was evaluated using the seventh edition of the American Joint Committee on Cancer/Union for International Cancer Control staging system (20). The primary outcome in this study was recurrent disease, which was defined as pathologically or cytologically proven lesions in suspicious LNs or operative thyroid-bed nodules or contralateral lobe nodules on neck US. Disease-free survival (DFS) was defined as the time interval from the date of initial surgery to the date of detection of recurrence. The secondary outcome was the DRS category of DTC for the first two years after the initial surgery, according to previous studies (12,18,21). The DRS system for DTC patients who underwent lobectomy was applied according to previous studies (18,21). Briefly, (i) a non-stimulated Tg <30 ng/mL, undetectable TgAb, and negative imaging were categorized as the excellent response group; (ii) a non-stimulated Tg >30 ng/mL or increasing Tg levels over time with similar TSH levels or increasing TgAb levels, and negative imaging were categorized as a biochemical incomplete response; (iii) nonspecific image findings or stable or declining TgAb were categorized as an indeterminate response; and (iv) identified structural disease was categorized as a structural incomplete response.
Statistical analysis
Data were analyzed using R v3.0 and R libraries (survival, car, Hmisc, and Cairo; R Foundation for Statistical Computing,
Results
Baseline patient characteristics
The baseline clinical and pathological characteristics of 639 patients with low-risk DTC are presented in Table 1. The mean tumor size was 0.77 ± 0.56 cm; 73.2% (341/466) of patients had a tumor <1 cm. The median follow-up period was 8.6 years (IQR 6.9–10.5 years). After the initial surgery, 260 (40.7%) patients underwent TST (the TST group), and 379 (59.3%) patients were followed without any LT4 replacement (No-TST group). Patients in the TST group received LT4 for TSH suppression for more than four years; the median duration of TST was 8.0 years (IQR 6.3–10.7 years). There were no significant differences in age or sex between the TST and No-TST groups. The primary tumors of patients in the TST group were significantly larger in size than those of patients in the No-TST group (p < 0.001). There were more patients with follicular thyroid carcinoma in the TST group than in the No-TST group (p < 0.001). Multifocal tumors and cervical LN metastases occurred more frequently in the TST group than in the No-TST group (p = 0.03 and 0.01, respectively). Significant differences in TNM staging were noted between the two groups (p < 0.001). After propensity score matching, no significant differences were found in age, sex, tumor size, cervical LN metastases, and TNM staging between the two groups (Table 1).
Categorical variables were described by numbers with percentages and continuous variables were described by mean and standard deviation.
TNM stage was determined by the 7th American Joint Cancer Committee TNM stage system.
TSH, thyrotropin; TST, TSH suppressive therapy; SMD, standard mean difference; TNM, tumor, node, metastasis.
Serum TSH levels in the No-TST group and TST group
The four categories of serum TSH levels in the No-TST and TST groups are shown in Figure 1B. In the No-TST group, most patients had normal serum TSH levels between 0.5 and 4.5 mIU/L (10.7% in the low-normal group and 64.8% in the high-normal group). Approximately 24% of patients had high serum TSH levels (>4.5 mIU/L). None of the patients in the No-TST group had a suppressed serum TSH level (<0.5 mIU/L). However, 36.5% of patients in the TST group had suppressed serum TSH levels (<0.5 mIU/L). In the TST group, only 15.5% of patients had a high-normal level of serum TSH (2.0–4.5 mIU/L), and no patients had high serum TSH levels (≥4.5 mIU/L). There was a significant difference in serum TSH levels between the two groups (p < 0.001).
Dynamic risk stratification between the No-TST group and TST group
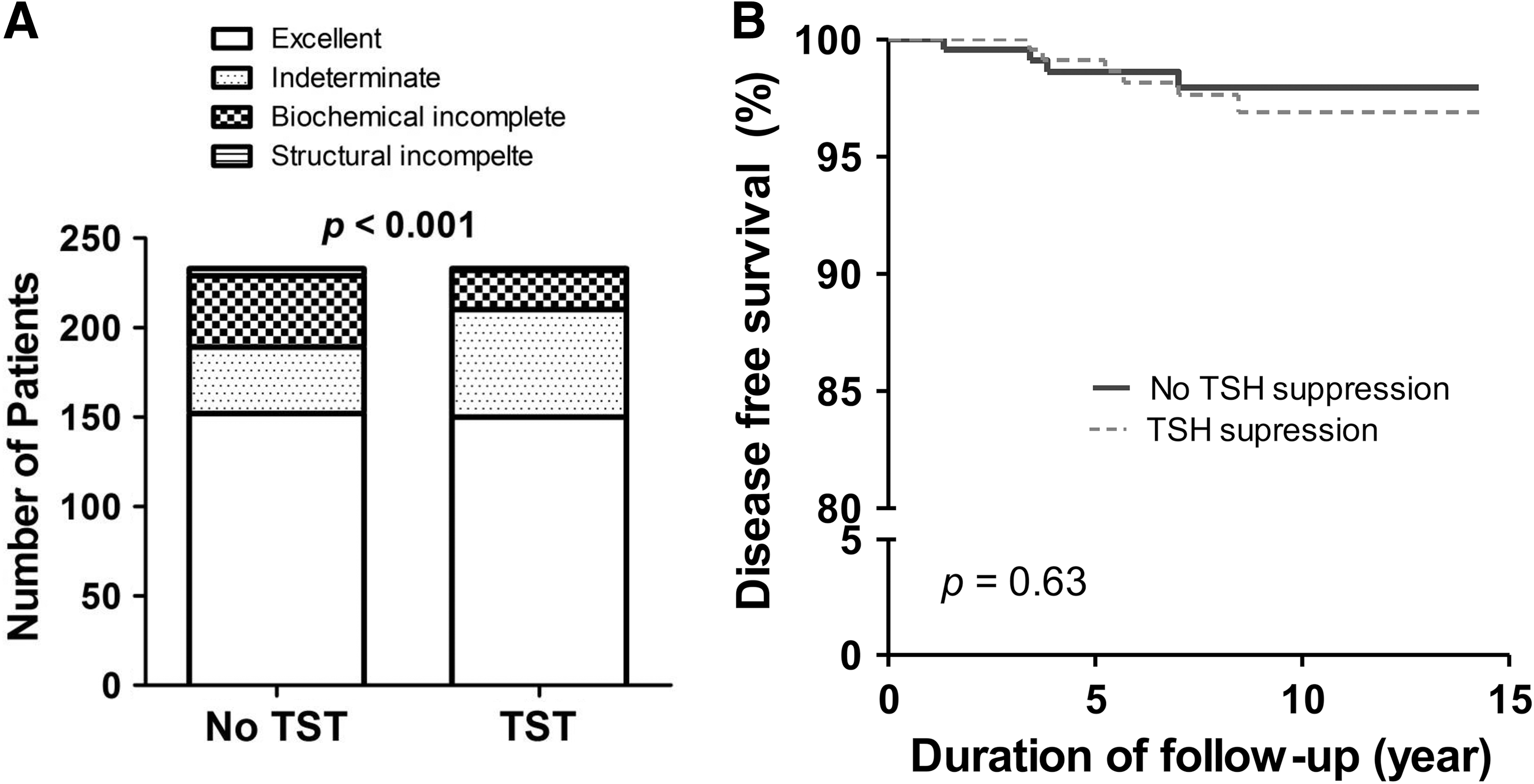
DRS was determined for the first two years after the initial surgery. The number of patients in each DRS category is shown in Figure 2A. In all, 152 (65.2%) patients in the No-TST group and 150 (64.4%) patients in the TST group were classified in the excellent treatment response category. There was no significant difference between the two groups in the excellent response category. However, there were significant differences between the two groups in the indeterminate response and biochemical incomplete response categories (p < 0.001). A total of 37 (15.9%) patients in the No-TST group and 60 (25.8%) patients in the TST group were in the indeterminate response category. Forty (17.2%) patients in the No-TST group and 22 (9.4%) patients in the TST group were in the biochemical incomplete response category. Four (1.7%) patients in the No-TST group and one (0.4%) patient in the TST group were classified in the structural incomplete response category.
Clinical outcome of patients with DTC with and without TSH suppression. (
DFS in the No-TST group and TST group
During the median follow-up period of 8.6 years, recurrence of the disease was observed in 10 (2.7%) patients. No significant differences in DFS between the No-TST and TST groups (p = 0.63; Fig. 2B) were observed. All recurrences in the TST group were located in the contralateral lobe of the thyroid, whereas three of four (75%) patients in the No-TST group had recurrences in lateral cervical LNs. In patients with tumor size more than 1 cm, there was no significant difference in DFS between TST group (n = 61) and No-TST group (n = 64; Supplementary Fig. S1; Supplementary Data are available online at
DFS by serum TSH levels
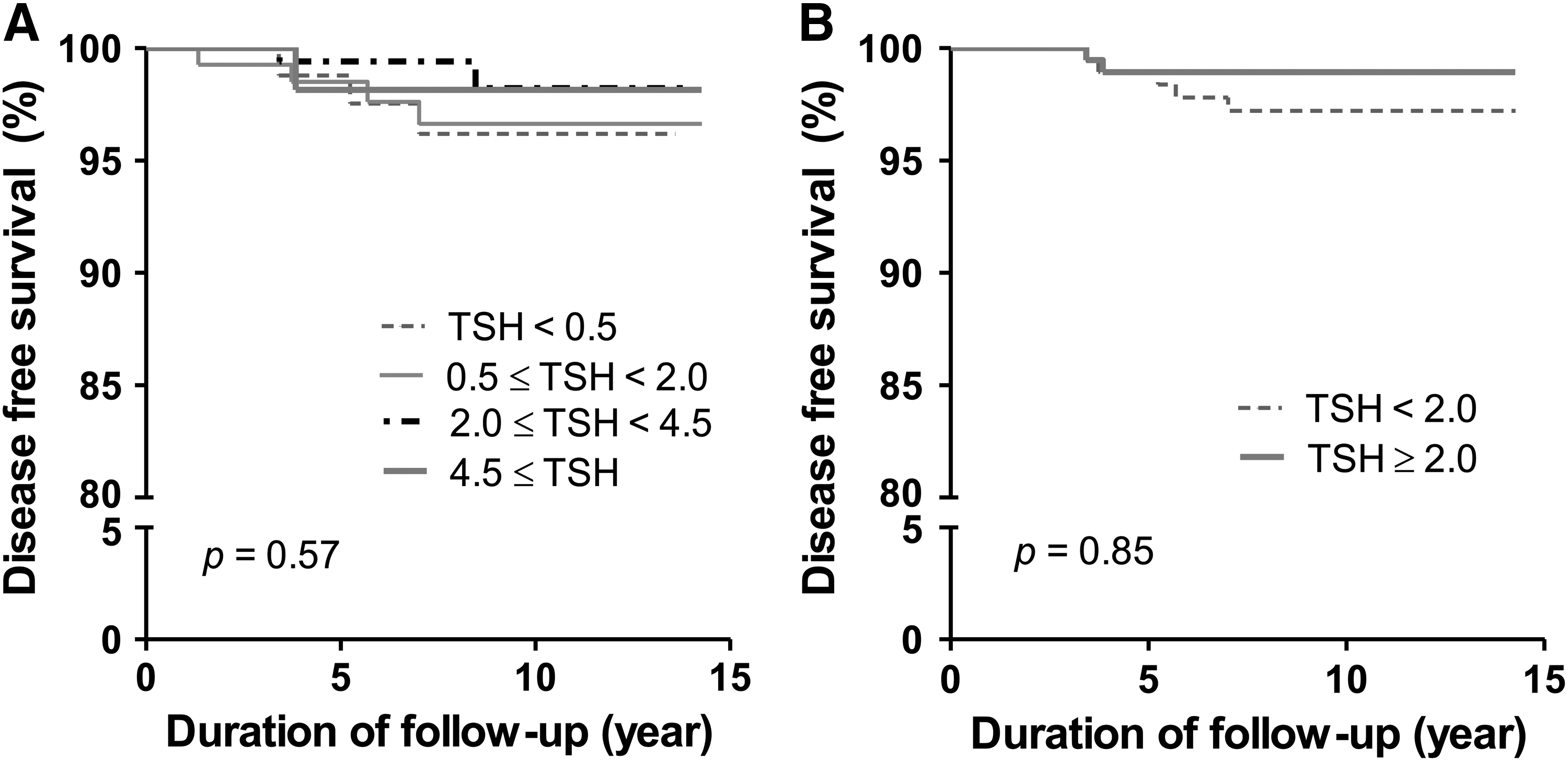
When the patients were stratified into four groups according to serum TSH levels, regardless of TST, no significant differences in DFS were found between the groups (p = 0.57; Fig. 3A). When two subgroups of these patients were found between the groups (ed in the contralate mIU/L) from the TST group, and 208 patients with non-suppressed serum TSH levels (≥2.0 mIU/L) from the No-TST group—were compared, still no significant differences were found in DFS between the subgroups (p = 0.85; Fig. 3B). The optimal TSH target for low-risk DTC patients who underwent lobectomy could not be identified.
DFS curves of the patients according to the level of serum TSH (
Discussion
This study evaluated the effects of TST in patients with low-risk small DTC within a propensity score–matched cohort. No significant differences were found in DFS between the TST group and the No-TST group. DFS did not differ, according to the serum TSH level, in low-risk patients. The proportion of patients with excellent treatment response was also similar between the two groups. More patients in the TST group had an indeterminate response, whereas more patients in the No-TST group had a biochemical incomplete response. These findings suggest that the effect of TST is limited in patients with low-risk small DTC.
Previous studies have reported that the suppression of serum TSH levels to <0.1 mIU/L could reduce cancer-specific mortality and disease recurrence in high-risk patients (11,13,24). However, these studies did not consistently demonstrate whether a similar degree of TST is also needed for low-risk patients to prevent recurrence. Jonklaas et al. reported that aggressive TSH suppression resulted in superior clinical outcomes for high-risk patients, whereas modest TSH suppression improved clinical outcomes in patients with stage II disease (12). However, TSH suppression was not shown to be effective for patients with stage I disease. Furthermore, the intensity of initial therapy (including the extent of surgery and RAI ablation therapy) varied in these previous studies. Therefore, it is difficult to determine the impact of TST alone. The present study included only patients with low-risk DTC who were treated with lobectomy in order to evaluate the clinical impacts of TST after minimizing the effects of other treatments. Before propensity score matching, patients in the TST group showed a tendency for larger-sized tumors, a greater number of cervical LN metastases, and multifocality compared to the No-TST group. Therefore, an attempt was made to minimize selection bias by using propensity score matching, after which no significant differences in clinical outcomes according to TST use could be demonstrated.
A prospective Japanese study reported no significant differences in five-year DFS according to TSH suppression for patients with high- and low-risk papillary thyroid cancer by age, metastasis, extent, and tumor size (AMES). The authors compared five-year DFS between patients with suppressed serum TSH levels (0.01–0.3 mIU/L) and patients within the normal range of serum TSH (0.4–5.0 mIU/L) (25). Patients who received total thyroidectomy or less-than-total thyroidectomy were included, regardless of the initial risk group. In addition, the extent of thyroid surgery differed in each risk group in that study. The present study only included patients with low-risk DTC who underwent lobectomy. Furthermore, this study did not supplement LT4 in any patient in the No-TST group. This approach minimizes the extent of surgery and illustrates that LT4 suppression does not impact outcomes in patients without evidence of hypothyroidism. This study also categorized the patients into four groups according to serum TSH levels and analyzed the DFS for these four groups. Another prospective study suggested that moderate TST improved the overall survival and DFS, regardless of stage of DTC (26). It is important to demonstrate potential differences in clinical outcomes between patients with suppressed serum TSH and patients with a TSH within the reference range, as reported in a previous study (25,26). A moderate degree of TSH suppression is generally acceptable for patients with low-risk DTC (14). However, evidence on the target levels for serum TSH in low-risk patients is lacking. This study analyzed clinical outcomes for a more detailed range of serum TSH levels, and it was found that serum TSH levels were not associated with DFS. The findings suggest that there is no need for LT4 supplementation in patients who undergo a lobectomy for DTC, except when hypothyroidism develops.
To evaluate the extent of residual disease, the differences in DRS between the two groups were estimated. Approximately 65% of patients showed an excellent response in both the TST and No-TST groups. However, the TST group had more patients with an indeterminate response. The TST group also had fewer patients with a biochemical incomplete response. Tg is synthesized by stimulation of the TSH receptor in normal thyroid tissue, as well as in DTC tissue (27). The suppressed TSH levels in the TST group may contribute to reducing serum Tg levels and thus in a lower rate of biochemical incomplete response compared to the No-TST group. Serum Tg levels also reflect the amount of benign or malignant thyroid tissue and the degree of TSH receptor stimulation (28). However, nonspecific US findings were observed more frequently in patients within the TST group, despite their relatively low levels of serum Tg, which led to a higher frequency of indeterminate responses in the TST group. There was a discrepancy between the growth of tissues or nodules in the contralateral lobe and the level of serum Tg in this study. This suggests that serum Tg levels may not exactly reflect the extent of residual disease in patients who undergo lobectomy.
The prognosis for patients with low-risk DTC is usually excellent. In several studies with median follow-up periods ranging from 5 to 10 years, disease recurrence was observed in <1–2% of low-risk patients (29 –31). In the current cohort, 10 (2.1%) patients experienced recurrences during the follow-up period, which is consistent with previous studies. All patients with recurrences in the TST group and the three of four patients with a recurrence in the No-TST group had contralateral lobe recurrences. The other patient in the No-TST group had cervical LN metastasis. The patients with a contralateral lobe recurrence underwent a completion thyroidectomy and prophylactic central LN dissection. The patient with cervical LN metastasis underwent a completion thyroidectomy and modified radical neck dissection. Seven of these patients underwent additional RAI remnant ablation therapy while the others did not. All patients who were treated for recurrences did not have any evidence of disease during the follow-up after undergoing additional treatments. All patients in the cohort underwent preoperative neck US; FNAC was performed on all suspicious nodules in the contralateral lobe when indicated. However, most cases of disease recurrence were identified on neck US in the contralateral lobe. The importance of neck US as a surveillance tool must be emphasized for low-risk patients who undergo lobectomy.
This study has some limitations, since it is based on retrospective data. Although propensity score matching was applied to minimize selection bias, the analysis could not eliminate the possibility of remaining biases. Second, the adverse effects of TST on bone metabolism and cardiovascular disease were not assessed during the follow-up period. Third, the number of patients with follicular thyroid carcinoma (FTC) was small in this study and may not be representative for low-risk FTC patients in general. Moreover, since the study sampled and enrolled low-risk patients from a single center, the number of patients with recurrent disease was small. Further multicenter or larger cohort–based studies are required to overcome this limitation.
However, this study also has several strengths. The efficacy of TST was evaluated in patients with low-risk DTC using a cohort that was treated with a defined protocol for initial and follow-up treatment. Furthermore, this study enrolled patients who had a sufficient follow-up duration. A long-term follow-up period is important to identify the clinical outcomes in patients with low-risk DTC. Disease recurrences in these patients are mostly identified within the first three to five years after initial treatment, but late recurrences have been found up to 10 years after the initial treatment (32).
In conclusion, this study shows no clinical benefits for TST in patients with low-risk DTC who underwent lobectomy. Serum TSH levels were not associated with disease recurrence in these patients. Therefore, TSH suppression and its related risks to bone metabolism and cardiovascular disease can be avoided for patients with low-risk DTC. LT4 replacement is therefore only needed for patients with evidence of hypothyroidism. Further studies are needed to elucidate the effects of TST in patients with intermediate-risk DTC in order to justify TSH suppression. A more individualized approach to TST that balances its benefits and risks is needed.
Footnotes
Acknowledgments
This study was supported by a grant from the Korean Health Technology R&D project, Ministry of Health and Welfare, Republic of Korea (HC15C3372). The authors retain the right to provide an electronic copy of the final peer-reviewed manuscript to Korea PubMed Central (PMC) upon acceptance for publication and to make it publicly available as soon as possible but no later than 12 months after publication.
Author Disclosure Statement
The authors have nothing to disclose.