
Abstract
Background:
This study validated the dynamic risk stratification (DRS) system with regard to its association with structural recurrence and risk factors associated with non-excellent responses in patients <45 years with stage I classical papillary thyroid cancer (PTC).
Methods:
This historical cohort study included 598 patients with stage I classical PTC <45 years of age treated with total thyroidectomy followed by radioactive iodine remnant ablation (n = 440), total thyroidectomy without radioactive iodine remnant ablation (n = 23), and thyroid lobectomy alone (n = 135).
Results:
The median follow-up period was 123 months. Structural recurrence occurred in 4.2% (n = 18/432) of the patients with an excellent response, 17.1% (18/105) of patients with an indeterminate response, 44.7% (17/38) of patients with a biochemically incomplete response, and 82.6% (19/23) of patients with a structurally incomplete response (p < 0.001) during the follow-up. The disease-free survival curves of each response showed significant differences (p < 0.001). Extensive extrathyroidal extension and extranodal extension were the independent risk factors associated with non-excellent response (p < 0.05).
Conclusions:
DRS may reduce unnecessary additional treatments by reclassifying initial risk estimates of structural recurrence. Furthermore, applying the risk factors associated with non-excellent response to initial therapy may be a more useful and viable surrogate of the risk for structural recurrence in stage I PTC patients <45 years of age.
Introduction
I
Various initial risk stratification systems, including the revised American Thyroid Association (ATA), National Comprehensive Cancer Network (NCCN), and the British Thyroid Association (BTA) guidelines, have been applied to guide the postoperative management and follow-up strategies during the early follow-up period after initial treatment (3,5,7,8). However, these initial risk stratifications are just a static representation of risks based on clinicopathologic features available at the time of initial therapy. They do not include adequate variables to consider the impact of initial therapy on long-term outcomes (6,9). Therefore, an indiscriminate application of these initial risk stratifications to patient cohorts with divergent clinical situations may result in unnecessary additional treatments or too many follow-up studies. To complement the shortcomings of initial risk stratification systems, a dynamic risk stratification (DRS) system based on the response to initial therapy was proposed to reclassify the initial risks and guide long-term treatment strategies (10 –13).
This study aimed to validate the DRS system based on the response to initial therapy with respect to its association with structural recurrence and to assess the clinicopathologic risk factors associated with a non-excellent response to initial therapy in stage I classical PTC patients <45 years of age.
Patients and Methods
Study population
This study retrospectively reviewed 598 patients with stage I classical PTC who underwent initial thyroid surgery with cervical lymph node (LN) dissection at the Asan Medical Center (Seoul, Korea) from 2000 to 2005. Patients aged ≥45 years and those with distant metastases at initial presentation or detected within 12 months after the initial operation were excluded. Patients presenting with PTC variants that could influence the outcomes and those with incomplete medical records were also excluded. Follicular variant of PTC was excluded from the present study to make the study population more homogeneous, although during the study period, the diagnosis of follicular variant of PTC was not common at the Asan Medical Center. In this analysis, the extent of extrathyroidal extension (ETE) was divided into three categories: none for intrathyroidal lesion without ETE; minimal for T3, including microscopic extension; and extensive for T4 lesions, according to the seventh edition of the AJCC TNM staging system. The study protocol was approved by the Institutional Review Board, and the requirement for informed consent from each patient was waived because of the non-interventional nature of the study.
For these enrolled patients, first the clinicopathologic characteristics and DRS were evaluated based on the response to initial therapy according to the treatment modalities applied, such as total thyroidectomy (TT) with/without radioactive iodine (RAI) remnant ablation or thyroid lobectomy alone. Association of each DRS category with the rate of structural recurrence and structural disease-free survival (DFS) during the follow-up period was then investigated. In addition, the risk factors for both structural recurrence and non-excellent response to initial therapy were analyzed and compared.
DRS
All of the enrolled patients were divided into four categories—excellent, indeterminate, biochemically incomplete, and structurally incomplete—based on the response to initial therapy, which was determined by the data obtained within two years after their initial treatment. The detailed definitions of each category in the DRS system were adopted from the current definitions of DRS proposed by Tuttle et al., and these are described in Table 1 (11,14,15). For the purpose of this study, patients not showing an excellent response were defined as having a non-excellent response.
TT, total thyroidectomy; RAI, radioactive iodine; Tg, thyroglobulin; TgAb, thyroglobulin antibody; TSH, thyrotropin.
Surgical strategy
During this study period, earlier ATA management guidelines for differentiated thyroid cancer (DTC) were adopted (6). Patients who refused TT were recommended to receive sufficient information about the potential risks and benefits of thyroid lobectomy versus TT as well as follow-up examinations.
At the Asan Medical Center, routine ipsilateral central compartment node dissection (CCND) is preferred, even in patients without clinically apparent LN metastases (LNM) on preoperative staging. Bilateral CCND was performed if suspicious LN enlargement in the contralateral central compartment was observed in preoperative staging or during operation and for bilateral cancer. Compartment-based CCND usually involved level VI and/or level VII LNs. The extent of CCND typically follows a well-established pattern. Prophylactic lateral neck dissection for PTC patients is not preferred, but therapeutic lateral neck dissection was performed in patients with lateral LNM confirmed by fine-needle aspiration cytology (FNAC) and measurement of thyroglobulin (Tg) levels in the washout fluid of the needles used for FNAC. Modified radical neck dissection (MRND) is preferred for levels IIa, III, IV, and V. If there were suspicious LNs in level IIa, LN dissection of level IIb was added.
RAI remnant ablation protocol
RAI remnant ablation following TT was performed at four to six weeks after the initial operation, according to the authors' own protocol. Briefly, an ablative dose of 30 mCi was administered to patients with a multifocal tumor and/or a tumor >1.0 cm without ETE. An ablative dose of 80 mCi was administered to patients with any tumor measuring <4.0 cm with ETE, and an ablative dose of 150 mCi was administered to patients with a tumor measuring ≥4.0 cm with or without positive surgical resection margins.
At the time of remnant ablation following thyroid hormone withdrawal or recombinant human thyrotropin (rhTSH) administration, the serum-stimulated Tg (sTg) level (reference range 1.0–23.3 ng/mL) was measured, together with anti-Tg antibody (TgAb) levels (reference range <60 IU/mL) when the TSH level (reference range 0.4–5.0 mIU/L) was >30 mIU/L. A post-ablation whole-body scan (WBS) was performed five to seven days after administering 131I.
Postoperative follow-up protocol
All of the study patients received follow-up examinations at the institution's outpatient clinic. Patients who underwent thyroid lobectomy alone or TT without RAI remnant ablation were checked at 1, 7, and 12 months postoperatively, and every 12 months thereafter, while receiving thyroid hormone treatment in order to decrease their serum TSH to subnormal levels without thyrotoxicosis. Thyroid function tests, including serum TSH, Tg, and anti-TgAb levels, were routinely checked at every visit, and neck ultrasonography (US) and/or computed tomography (CT) scans were routinely performed once a year.
In patients who underwent TT with RAI remnant ablation, diagnostic WBS following thyroid hormone withdrawal or rhTSH administration was performed 6–12 months after remnant ablation with the simultaneous measurement of serum sTg. Serum Tg and TgAb measurement and neck US were performed during the follow-up period. When the sTg was ≥2–10 ng/mL but a neck US showed no evidence of disease, 18F-deoxyglucose positron emission tomography (FDG-PET) or chest CT were considered in order to localize persistent/remnant disease. Any patients suspected of locoregional recurrence underwent US-guided FNAC. Distant metastasis was diagnosed using WBS, chest CT, or 18F-FDG PET/CT and confirmed by serial imaging and/or cytology performed by FNAC.
Recurrence was defined as the appearance of cytologically or histopathologically proven malignant tissue, or the appearance of highly suspicious structural lesions on cross-sectional or functional imaging studies after a disease-free status for at least one year after initial operation. However, even highly suspicious locoregional structural disease was not considered as a recurrence unless the lesion was confirmed by FNAC or surgical biopsy. Persistent disease was defined when there was no change within one year after initial operation presenting the appearance of structural lesions on cross-sectional or functional imaging studies. Elevated serum Tg or TgAb levels without clinical evidence of structural disease were not considered as a true recurrent/persistent disease.
Statistics
Continuous variables are presented as the mean ± standard deviation (SD) or as medians and ranges, while categorical variables are presented as percentages and absolute numbers. Univariate and multivariate Cox proportional hazards modeling analyses or logistic regression analyses were used to identify the risk factors for structural recurrence or non-excellent response to initial therapy, respectively. Hazards ratios (HR) and odds ratios (OR) with confidence intervals (CI) were calculated. All clinicopathologic variables were entered into the univariate and multivariate analyses. For clinical applicability, the area under the curve (AUC) was calculated using receiver-operating characteristic (ROC) curve analysis in order to evaluate the cutoff value for continuous variables with significance. Survival outcomes were analyzed using the Kaplan–Meier method and log-rank tests. Here, p < 0.05 was considered significant. These statistical analyses were performed using SPSS v21 and R v3.1.1 software, with packages “lattice,” “survival,” and “survival ROC” (R Project, Vienna, Austria).
Results
Demographic characteristics
The clinicopathologic characteristics of the patients enrolled in this study are summarized in Table 2. The median follow-up duration was 123 months (range 33–188 months). Most of the patients underwent TT with RAI remnant ablation (440/598; 73.6%); the rest received total thyroidectomy without RAI remnant ablation (23/598; 3.8%) or thyroid lobectomy alone (135/598; 22.6%). The overall rate of structural recurrence was 12.0% (72/598). All patients had locoregional recurrence, including central LN recurrence in nine (12.5%) cases and lateral LN recurrence in 63 (87.5%) cases. Based on the treatment modalities adopted, structural recurrence was observed in 13.4% (59/440) of the patients treated with TT and RAI remnant ablation and in 9.6% (13/135) of those treated with thyroid lobectomy alone. None of the patients died of PTC. Among 598 enrolled patients, an excellent response was achieved in 432 (72.2%) patients, an indeterminate response in 105 (17.6%) patients, a biochemically incomplete response in 38 (6.4%) patients, and a structurally incomplete response in 23 (3.8%) patients. According to treatment modalities applied, an excellent response was achieved in 66.4% (292/440) of the patients treated with TT and RAI remnant ablation, in 91.3% (21/23) of those receiving TT without RAI remnant ablation, and in 88.1% (119/135) of those treated with thyroid lobectomy only.
CCND, central compartment node dissection; MRND, modified radical neck dissection; LN, lymph node.
Risk factor analysis for structural recurrence
In univariate analysis, age, primary tumor size, extensive ETE, lymphovascular invasion, LN metastasis, number of metastatic LNs, metastatic LN ratio, and extranodal extension were identified as potentially significant risk factors for structural recurrence (p < 0.05; Table 3). Using the DRS system, a non-excellent response was a risk factor for structural recurrence (p < 0.001). However, in multivariate analysis, extensive ETE (HR = 4.91 [CI 1.89–12.72], p = 0.001) and biochemical incomplete and structural incomplete responses (HR = 8.49 [CI 3.39–21.30], p < 0.001, and HR = 178.41 [CI 31.62–1006.71], p < 0.001, respectively) were recognized as the independent risk factors for structural recurrence (Table 3).
NED, no evidence of disease; HR, hazard ratio; CI, confidence interval; NA, not available.
DRS based on the response to initial therapy and its correlation with structural recurrence
Based on each response to initial therapy, structural recurrence occurred in 18 (4.2%) of the patients showing an excellent response, 18 (17.1%) showing an indeterminate response, 17 (44.7%) showing a biochemically incomplete response, and 19 (82.6%) showing a structurally incomplete response during follow-up (Table 4). According to the treatment modalities applied, structural recurrence occurred in 11 (3.8%) patients with an excellent response, 18 (18.8%) patients with an indeterminate response, 17 (48.6%) patients with a biochemically incomplete response, and 13 (76.5%) patients with a structurally incomplete response among the patients treated with TT and RAI remnant ablation (Table 4). In thyroid lobectomy patients, structural recurrence occurred in seven (5.9%) patients with an excellent response and six (100%) patients with a structurally incomplete response (Table 4).
The structural DFS curves of the patients with each response showed significant differences, which suggests that the DRS correlated well with the long-term risk of structural recurrence (p < 0.001; Fig. 1).
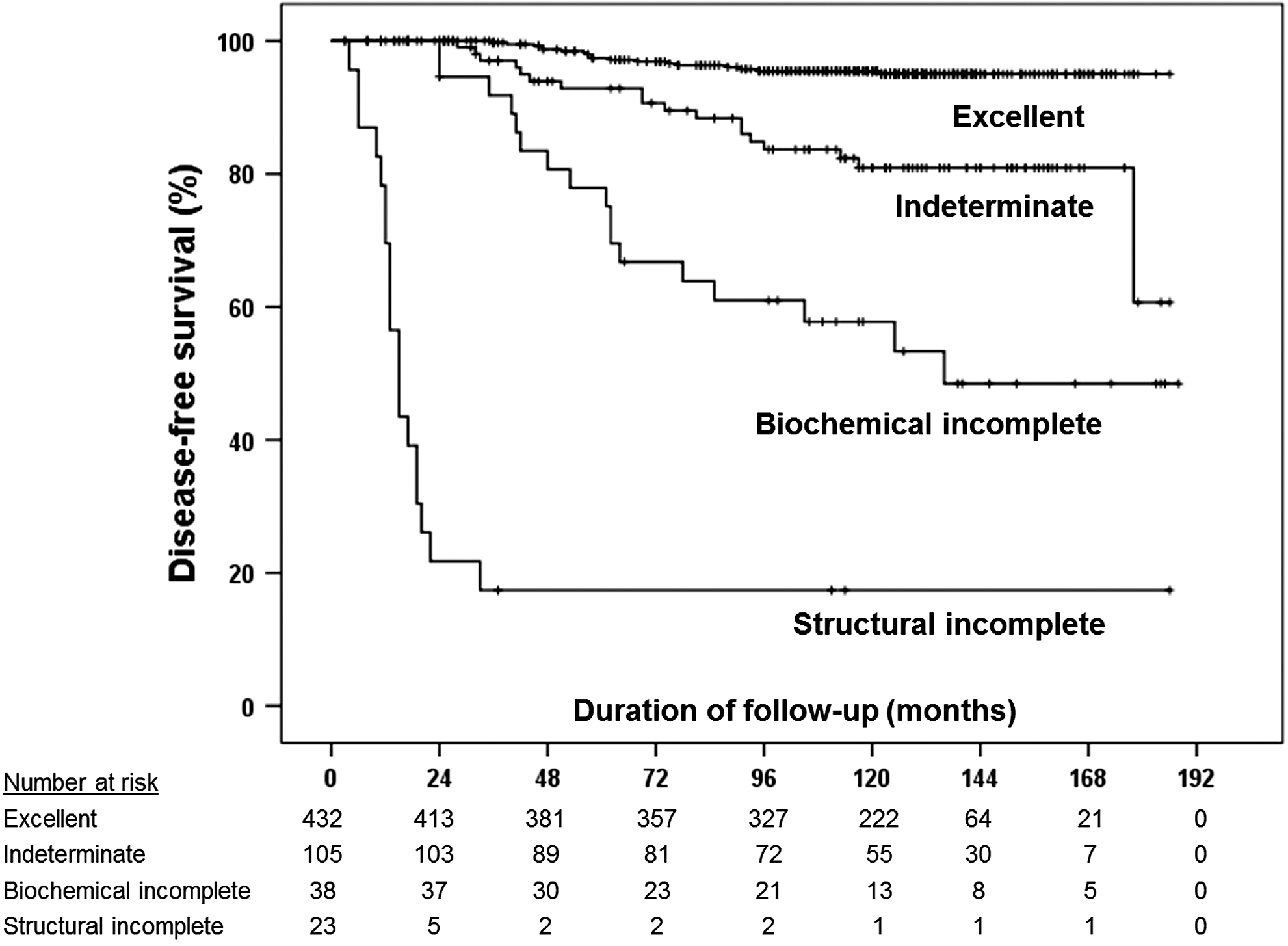
Disease-free survival curves of the dynamic risk stratification based on response to the initial therapy (p < 0.001).
Clinicopathologic risk factor analysis for a non-excellent response to initial therapy
In univariate analysis, age, TT with RAI, primary tumor size, extensive ETE, multiplicity, bilaterality, lymphovascular invasion, LN metastasis, number of retrieved LNs, number of metastatic LNs, metastatic LN ratio, metastatic LN size, and extranodal extension were identified as potentially significant risk factors for a non-excellent response (p < 0.05; Table 5). However, in multivariate analysis, extensive ETE (HR = 7.13 [CI 1.07–47.37], p = 0.042) and extranodal extension (HR = 4.78 [CI 2.22–10.30], p < 0.001) were the independent risk factors for a non-excellent response to initial therapy.
Discussion
This study used data obtained within two years after initial therapy to validate the association of DRS with structural recurrence and structural DFS in stage 1 classical PTC patients <45 years of age. This study demonstrates that biochemical and structural incomplete responses to initial therapy are significantly related to structural recurrence, and extensive ETE and extranodal extension were independent risk factors related to a non-excellent response to initial therapy. Several previously published studies have described that low-risk patients with intrathyroidal PTC and low-volume LN metastasis (≤5 and <0.2 cm in diameter) can be adequately treated with less extended surgery and do not require additional treatments such as RAI ablation or completion thyroidectomy (1,3,4,16 –20). Moreover, high-risk patients harboring extensive ETE, incomplete tumor resection, distant metastases, or high-volume LN metastasis (>3 cm in diameter) can be identified by proper imaging studies preoperatively or during surgery and should be treated with more extensive curative surgery with additional treatments such as RAI remnant ablation and TSH suppression (7,8,21,22). However, all of the histopathologic features (microscopic ETE, aggressive histologic types, incidental multifocality, or lymphovascular invasion) related to the intermediate risk category are likely to be unrecognized preoperatively or during surgery. These factors are probably identified postoperatively. On those occasions, surgeons should consider whether to perform immediate adjuvant treatments such as RAI remnant ablation and/or completion thyroidectomy, especially in those patients who underwent thyroid lobectomy alone.
Since there are no unique and absolute clinicopathologic risk factors to predict long-term structural recurrence accurately, risk factor analysis should be individualized based on each patient cohort and appropriate endpoint, and the decision for additional treatment should be made by balancing the risk of recurrence or disease-specific mortality with the potential benefits and risks of additional treatments. Recently, a DRS system was proposed to reclassify the initial risk estimates based on the response to initial therapy, and this has been shown to predict the long-term outcomes related to structural recurrence more accurately compared to the ATA initial risk (10 –12,23). Additionally, the ability to predict structural recurrence has been shown to be more accurate with the DRS system than with the ATA initial risk stratification system with regard to the proportion of variance explained (6,10 –12,23). On the basis of the results of these previous studies, the response to initial therapy was chose over structural recurrence itself as a primary endpoint of the present study. The other reason was that the response to initial therapy is determined using cross-sectional data obtained within two years after initial therapy, which can be evaluated without omission and would not be changed or missed over time. On the contrary, structural recurrence is longitudinal data that can change over time and in which late recurrence may be missed if the follow-up period is not long enough.
In this study, the DRS categories were well associated with structural recurrence, and each category showed significantly different structural DFS curves in stage I classical PTC patients <45 years of age. The association of DRS with structural recurrence could be determined, and biochemically and structurally incomplete responses to initial therapy were the independent risk factors for structural recurrence. Furthermore, extensive ETE and extranodal extension were identified as independent histopathological risk factors for a non-excellent response to initial therapy. This study is the first to evaluate comprehensively the association of DRS with structural recurrence and the risk factors for a non-excellent response to initial therapy in a cohort of stage I PTC patients <45 years of age. It is particularly noteworthy that none of the ATA intermediate risk factors, including microscopic ETE, multifocality, lymphovascular invasion, number of metastatic LNs, and maximal size of metastatic LNs, were independent risk factors for either a non-excellent response to initial therapy or structural recurrence in this study. Thus, clinicians need to be aware of the fact that there are no unique and absolute clinicopathologic risk factors, and risk factor analysis should be individualized based on specified patient cohorts.
This study has limitations inherent to retrospective studies. Unlike previous studies, the present study enrolled a relatively large number of patients treated with TT with RAI remnant ablation, as well as TT without RAI and thyroid lobectomy alone. However, the number of patients receiving the latter two treatment modalities was relatively small in order to be able to evaluate clearly the impact of DRS on predicting long-term outcomes in the entire cohort. Moreover, the parameters and the cutoff of Tg used to define the response to initial therapy in patients submitted to thyroid lobectomy alone, unlike in patients treated with total thyroidectomy, are not well established and need to be better characterized through further studies with larger numbers of patients and longer follow-up periods (14).
Consequently, even though some ATA-defined unfavorable histopathologic features are identified after initial surgical treatment, immediate adjuvant therapy, such as RAI remnant ablation with/without completion thyroidectomy, does not have to be applied uniformly to all of the patients with those features if the primary cancer was curatively removed. Additional adjuvant treatments can be delayed until the response to initial therapy is confirmed two years after initial treatment. Moreover, even if patients or physicians consider immediate adjuvant treatments, they should be limited to the patients presenting with individualized risk factors associated with a non-excellent response to initial therapy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.