
Abstract
Background:
The term “nodular goiter” has long been used to refer to a nodular thyroid gland, based on the assumption that nodule growth may be associated with hyperplasia of the surrounding non-nodular tissue. The aim of this prospective, multicenter, observational study was to determine whether nodule growth is accompanied by growth in the non-nodular tissue.
Methods:
Eight Italian thyroid-disease referral centers enrolled 992 consecutive patients with one to four benign nodules. Nodular and non-nodular thyroid tissue volumes were assessed for five years with annual ultrasound examinations.
Results:
In participants whose nodules remained stable (n = 839), thyroid volumes did not change (baseline 15.0 mL [confidence interval (CI) 14.5–15.6]; five-year evaluation 15.1 mL [CI 14.5–15.7]). In participants with significant growth of one or more nodule (n = 153), thyroid volumes increased and by year 5 were significantly greater than those of the former group (17.4 mL [CI 16–18.7]). In 76 individuals with unilateral nodules that grew, the mean nodular lobe volume significantly exceeded that of the contralateral lobe (8.6 mL [CI 7.4–9.8] vs. 6.7 mL [CI 6–7.4]). The unaffected lobe volumes remained stable over time, while nodular lobes grew steadily and were significantly greater at the end of follow-up (10.1 mL [CI 8.9–11.3]). Excluding the volume of the largest growing nodule in these cases, the remaining volume of the affected lobe remained virtually unchanged with respect to its baseline value. Furthermore, there was no significant difference in the non-nodular tissue volume between the unaffected lobe and the affected lobe (with the largest growing nodule volume subtracted), both at baseline and at the end of follow-up.
Conclusions:
The growth of thyroid nodules is a local process, not associated with growth of the surrounding non-nodular tissue. Therefore, a normal-sized thyroid containing nodules should be referred to as a “uni- or multinodular thyroid gland” and considered a distinct entity from “uni- or multinodular goiter.”
Introduction
T
A final issue centers on the question of pathogenesis. Non-autoimmune goiters have historically been considered to be predominantly a manifestation of iodine deficiency (12), and that continues to be the case. However, efforts to eliminate iodine deficiency have been largely successful over the last decades (13), at least in developed countries, where the prevalence of iodine-deficiency goiter has decreased, even if systematic evaluation of outcomes is needed (14). In addition, other pathogenetic pathways can lead to the formation of thyroid nodules. The most widely acknowledged causes (iodine-deficiency disorders, Graves' disease, Hashimoto's thyroiditis) all involve thyroid hyperplasia that can be related to excess thyrotropin receptor (TSH-R) activity (owing to stimulation of the receptor by TSH itself or by activating autoantibodies (15) or to activating mutations of the TSH-R gene (16,17). In the classic pathogenetic description of nodular goiter developed originally by Marine (18) and later by Taylor (19), this initial phase of diffuse thyroid hyperplasia is followed by nodular transformation caused by the alternation of stimulation phases with resting states of the thyroid tissue. A more recent view ascribes the nodular transformation to increased mutagenesis within the hyperplastic tissue secondary to the elevated cell division rates and the increased production of free radicals (9). In both cases, the natural history of the nodular goiter implicitly includes progressive increases in the size of both the gland as a whole and in the dimensions (and possibly the number) of individual nodules (8,9).
How well does this model fit the cases of thyroid nodular disease being seen in today's clinics? The diagnosis of these lesions has increased remarkably over the past 30 years, largely as a result of the incidental discovery of small, asymptomatic lesions during imaging studies performed for other reasons (20). A prospective multicenter study was recently initiated of the natural history of benign thyroid nodules, and in 2015, data were analyzed from the first five years of follow-up for 992 cases (21). On the basis of this experience, it was concluded that very few benign nodules (approximately 15%) exhibited significant growth during the first five years after their first evaluation. In the present study, a secondary analysis was performed of sonographic follow-up data for the same 992 cases, comparing the behaviors of the non-nodular thyroid parenchyma (surrounding and contralateral) in patients whose nodules grew and those whose nodules remained stable in size over the five-year observation period. The aim was to determine whether thyroid nodule growth is paralleled by growth in the non-nodular tissue.
Materials and Methods
Original cohort enrollment and data collection
Data analyzed in the present study were collected in eight hospital-based thyroid disease referral centers in Italy, four of which were academic sites. The protocol for the original study (21) was approved by the Institutional Review Boards of each participating center, and written informed consent was obtained from all participants. Between January 1, 2006, and January 31, 2008, all centers consecutively enrolled patients presenting with one to four asymptomatic thyroid nodules that were presumed to be benign on the basis of a benign cytology report or the absence of suspicious sonographic features. The protocol-specified enrollment criteria have been described in detailed elsewhere (21) and are summarized in Table 1.
The decision to exclude patients with more than four nodules was made to facilitate the sonographic follow-up over time.
Benign cytology (Bethesda class II) for any lesion with (i) sonographic features suggestive of malignancy (i.e., at least one of the following: hypoechogenicity, irregular margins, taller-than-wide shape [i.e., anteroposterior diameter greater than transverse diameter], intranodular vascular spots, microcalcifications); (ii) largest diameter of ≥10 mm (in patients with multiple nonsuspicious nodules of this size, only the largest lesion was aspirated); or (iii) both. Nonsuspicious lesions measuring <10 mm were classified as presumably benign, without cytological confirmation.
Nonsurgical interventions include radioactive iodine ablation and ultrasound-guided, minimally invasive procedures such as ethanol injection and radiofrequency, laser, or ultrasound ablation.
These criteria were designed to exclude patients with chronic or acute thyroiditis because: (i) the associated inflammatory changes hamper sonographic differentiation of true nodules and pseudonodules, and (ii) positive thyroid antibody titers are a potential confounding factor in a study of the natural history of thyroid nodules.
Hypoechoic and heterogeneous thyroid parenchyma.
Clinical (painful thyroid swelling) and sonographic evidence (hypoechoic and heterogeneous thyroid parenchyma) of subacute thyroiditis.
Enrolled patients were followed with yearly visits through January, 31, 2013. As previously described (21), each visit included a color Doppler ultrasound examination of the thyroid and neck performed with multi-frequency (7.5–12 MHz) linear transducers. Examiners were endocrinologists with specific training and at least 10 years' experience in thyroid and neck ultrasonography. All study-related examinations at a given center were done by the same operator. At each visit, the examiner measured the transverse, anteroposterior, and longitudinal diameters of each nodule and of each thyroid lobe without consulting data from the previous visit. Nodule and lobe volumes were calculated with the ellipsoid formula (the product of the three largest perpendicular diameters multiplied by 0.525) (22). Lobe volumes were summed to obtain the volume of the gland as a whole. No data about urinary iodine concentration were collected at any time during the study.
Data analysis and definitions
Goiter was defined as a thyroid gland volume >20.1 mL in men and >15 mL in women, based on data collected in a healthy Italian population (23) with a median urinary iodine excretion of 122 μg/L (M = 140.5 ± 56 μg/L; range 60–274 μg/L), indicating a iodine-sufficient area according to the World Health Organization criteria. Nodule growth or shrinkage was considered to be significant when it involved at least two nodule dimensions, amounting to at least 2 mm and representing at least 20% of the baseline diameter, corresponding to a 50% change in volume, that is reported to be the minimal reliably reproducible change in nodule size (22,24).
The present analysis focused on the magnitude and temporal trend of spontaneous changes in the volume of the thyroid gland and of each of its lobes. Subsequently, to elucidate the behavior of both nodular and non-nodular thyroid tissues during thyroid volume changes, and to explore their potential association, the subset of patients with growing, unilateral nodules, whose nodules were confined to the right or left lobe of the gland, was selected, and the two lobes were analyzed separately. This approach was chosen to identify lobes composed only of non-nodular tissue, thus avoiding potential interfering factors and calculations prone to bias.
Statistical analysis
Statistical analyses were performed with SAS software v9.4 (SAS Institute, Inc.). Data were summarized as median and interquartile range for continuous variables and frequency (percentages) for categorical variables. The continuous variables were not normally distributed, according to the Shapiro–Wilk test. Baseline characteristics of the participant subgroups were compared using the Mann–Whitney U-test for continuous variables and the Pearson v2 statistic or Fisher's exact test (as appropriate) for categorical variables. Thyroid and nodular volume changes over time were evaluated using a mixed model for repeated measurements (longitudinal models) with an autoregressive variance–covariance structure, in order to account for correlation and to obtain valid inferences based on two sources of variability (between and within variability). Results at each time point were expressed as estimated means and 95% confidence intervals (CI) and were compared with analysis of variance for repeated measures. Generalized linear mixed models were used to account for missing data on patients lost to follow-up (25). All statistical tests were two-sided, and a p-value of <0.05 was considered statistically significant.
Results
Between January 1, 2006, and January 31, 2008, 1009 patients with apparently benign thyroid nodules were enrolled. Seventeen were subsequently excluded because they developed thyroid dysfunction or thyroid autoantibody positivity. The population that completed the original study included 992 patients with 1567 nodules at baseline (Supplementary Fig. S1; Supplementary Data are available online at
Next, the temporal trends of the total thyroid gland volumes were evaluated in two subgroups defined by thyroid nodule behavior. The first subgroup comprised the 153 (15.4%) participants who experienced significant growth of one or more nodules during the five-year study period. Their baseline characteristics are shown in Table 2 (right column). The subgroup with nodule growth was not significantly different from the rest of the study population (i.e., the 839 [84.6%] participants whose nodules remained stable or decreased, as described below) in terms of sex, age, or baseline thyroid volumes (15.1 mL [CI 14.1–16.2] vs. 15.0 mL [CI 14.5–15.6 mL]). In the patients whose nodules remained stable or shrunk, the whole thyroid volume did not change (five-year evaluation 15.1 mL [CI 14.5–15.7 mL]). However, in the subgroup with significant nodule growth, the volume of the gland also increased in a gradual, linear fashion, and by year 5, it was significantly greater than that of the patients whose nodules remained stable or decreased in size (17.4 mL [CI 16–18.7] vs. 15.1 mL [CI 14.5–15.7]; Fig. 1). In the former group (n = 153), the proportion of patients whose thyroid nodules were associated with goiter rose from 30.1% (46/153) to 43.8% (67/153).
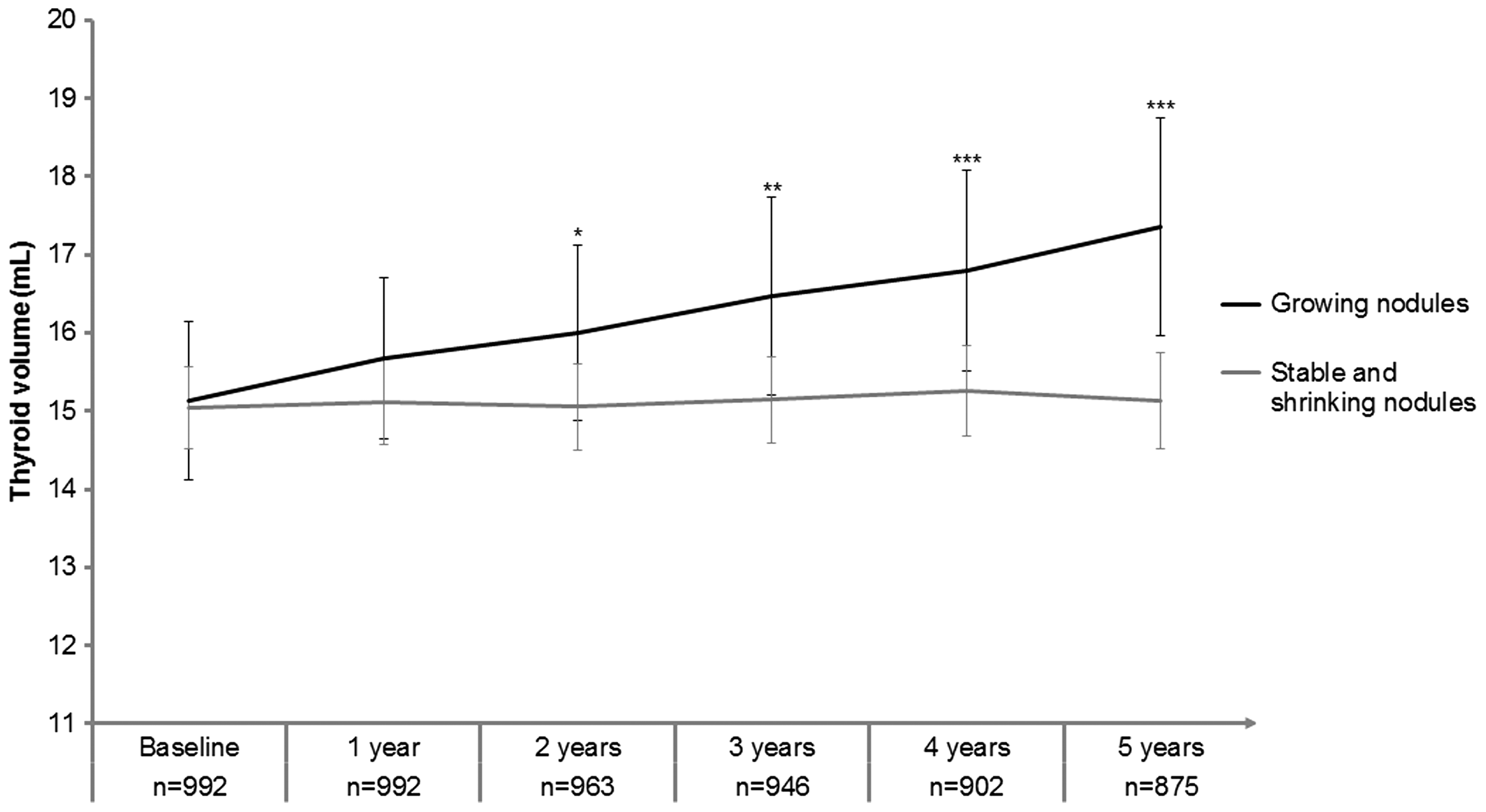
Thyroid volume in patients with at least one growing nodule (n = 153) and shrinking and/or stable nodules (n = 839). In 184 patients, one or more nodules shrank spontaneously. In the remaining patients (n = 655), the nodules were stable. Results are presented as means [confidence intervals (CI)] for each time point. Differences versus baseline: *p < 0.01; **p < 0.001; ***p < 0.0001. Shorter follow-up times were considered in 117 cases: 71 patients were lost to follow-up, four died due to non-thyroid-related causes, and 42 had thyroidectomies before the five-year assessment. The actual number of patients evaluated at each time point is reported below the horizontal axis.
For continuous values, the median and interquartile range are reported.
Difference in thyroid volume at baseline between male and females: p = 0.0002.
Difference in thyroid volume at baseline according to the age class: p < 0.0001.
Difference in thyroid volume at baseline between male and females: p = 0.0007.
Difference in thyroid volume at baseline according to the age class: p = 0.0002.
BMI, body mass index; TSH, thyrotropin.
In 93 (9.3%) patients, one (in 76 patients) or more (two in 15 patients, and three in two patients) new nodules were recorded during the follow-up. In these patients, there was no significant change in thyroid volume (baseline volume 14.8 mL [CI 13.5–16.0 mL], 5th-year volume 14.1 mL [CI 12.7–15.4 mL]).
To explore whether the whole gland expansion in patients with nodule growth was due in part to increases in the volume of the non-nodular thyroid tissue, subsequent analyses focused on the 76 individuals with unilateral nodular involvement (right lobe in 44; left lobe in 32), and at least one nodule that displayed significant growth during the follow-up. The clinical features of these cases are reported in Table 2. As shown in Figure 2A, the mean thyroid volume for this subgroup increased over time. At baseline, 21 (27.6%) of the 76 patients had sonographically determined thyroid volumes that met the predefined criteria for classification as goiter. During the five-year follow-up, 11 additional cases fit the definition of goiter. As shown in Figure 2B, the mean baseline volume of the nodular lobe was significantly greater than that of the contralateral lobe, which was nodule free (8.6 mL [CI 7.4–9.8 mL] vs. 6.7 mL [CI 6–7.4 mL]). The volume of the unaffected lobes remained completely stable during the follow-up, with a mean value in year 5 of 6.9 mL [CI 6.1–7.6 mL]. In contrast, the nodule-bearing lobes grew steadily and were significantly greater at the end of follow-up (10.1 mL [CI 8.9–11.3 mL]). A comparison of Figure 2A and B shows that the overall increase in total thyroid volume in these 76 cases was fully accounted by the volume increase in the nodular lobe. Indeed, the thyroid volume increases were caused specifically by growth of the nodular tissue in the affected lobe, as shown in Figure 2C. If the volume of the largest growing nodule is excluded in these cases, the remaining volume of the affected lobe remained virtually unchanged with respect to its baseline value. There was no significant difference in the non-nodular tissue volume between the unaffected lobe and the affected lobe (with the largest growing nodule volume subtracted), both at baseline and at end of follow-up. This behavior was observed across all cases, regardless of whether the unilateral involvement affected the right or left thyroid lobe (Supplementary Table S1).
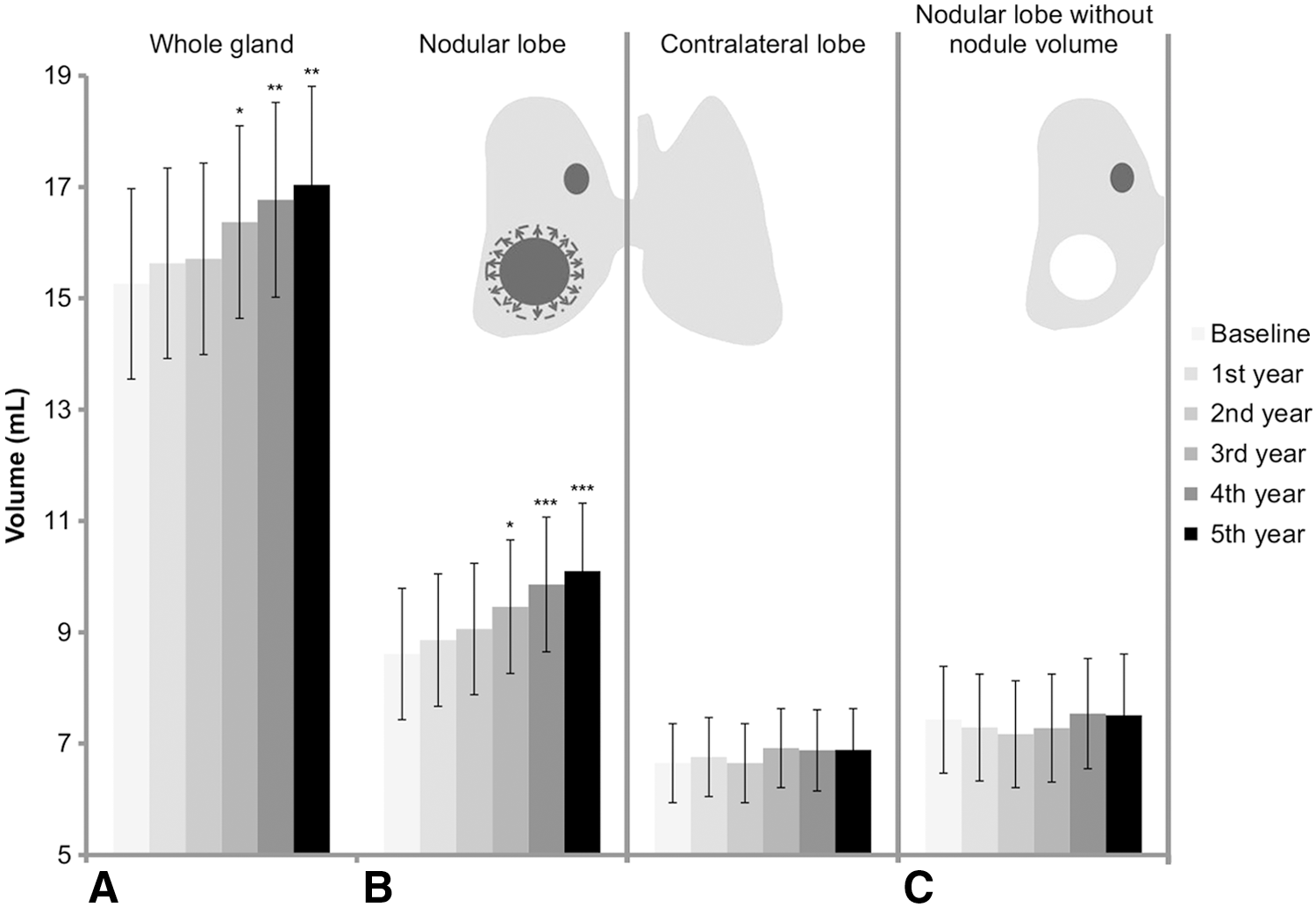
Thyroid and lobe volumes in the patients whose nodules (one or more) were confined to one lobe and included at least one nodule displaying growth (n = 76 at baseline). (
Furthermore, 104 patients with unilateral nodules had one or more shrinking nodules. In these patients, there was no significant increase or decrease in thyroid or lobe volume (Supplementary Table S2). After exclusion of seven patients who had at the same time both growing and shrinking nodules, there was no significant variation in thyroid and lobes volume (Supplementary Table S3).
A power analysis was performed for the main results, with a significance level (alpha) of 0.05. A sample size of 153 achieved 95% power to detect a mean of paired differences of 1.8 with an estimated standard deviation (SD) of differences of 6.1 (Fig. 1), while a sample size of 76 achieved 79% power to detect a mean of paired differences of 1.5 with an estimated SD of differences of 4.6 (Fig. 2).
Discussion
The population examined in this study consisted of consecutively enrolled patients with up to four apparently benign thyroid nodules and no evidence of thyroid dysfunction or autoimmune thyroid disease. It is thus highly representative of the benign nodular disease seen today by endocrinologists. In fact, in two recently published series (26,27), approximately 70% of patients presenting with thyroid nodules had no evidence of thyroid autoimmunity or hypothyroidism.
Although cases of this type continue to be referred to as “nodular goiter” in a variety of publications, the findings indicate that this usage is inappropriate. For example, at baseline, two thirds of the patients in the present cohort had thyroid volumes that failed to meet currently used definitions of “goiter” (23). In addition, increases over time in the total thyroid volume were seen only in participants with growing nodules: in subjects whose nodules remained stable or diminished in size, the volume of the gland itself remained unchanged. Studies of the patients whose nodes were confined to the right or left lobe of the gland revealed that the nodule-bearing lobe was significantly larger at baseline than the unaffected control lobe. Increases over time in lobar volumes occurred exclusively in the affected lobes. More specifically, they occurred only in affected lobes that contained one or more nodules displaying significant growth, and the volume increase at the lobar level was appreciable only when the volume of the growing nodule was included in the calculation.
Collectively, the present findings would suggest that in patient populations resembling the one that was analyzed, increases observed in the thyroid volume are primarily the result of focal alterations or processes within the glandular parenchyma (e.g., genetic variations (28), impaired thyroid-specific gene expression (29,30), and deranged angiogenesis (31)), which give rise to the growth of space-occupying nodules. This model contrasts sharply with those described for “nodular goiters” commonly reported in a context of iodine deficiency, Graves' disease, Hashimoto's thyroiditis, excessive TSH-R stimulation, or inflammation (9,32). In these instances, nodule formation is envisioned as secondary to a pathologic process that produces variable hyperplasia of the entire gland. The thyromegaly is considered the result of growth at the level of both the nodular tissue and the surrounding thyroid parenchyma, and this view has long supported the widespread use of therapeutic TSH suppression in patients with benign thyroid nodules (1 –3,33 –35).
This study has some obvious limitations. The possibility cannot be excluded that in other series, nodular and non-nodular tissue behaviors might differ from those observed in the present population. Indeed, a different picture altogether might conceivably emerge from an analysis of a larger sample, including a larger number of true goiters and growing nodules. A longer follow-up period might also be necessary to disclose significant changes in non-nodular tissue. For this reason, the follow-up of the present cohort is ongoing, and additional data will be collected and analyzed in the future. Furthermore, the data will need to be replicated in other populations. However, given the size of the population analyzed herein and the prospective, multicenter nature of its enrollment, it is reasonable to expect that the findings will prove to be generalizable to patients with apparently benign thyroid nodules in the absence of other thyroid disease.
Indeed, this study was not designed, and is therefore not able to provide information about nodule initiation, because data before nodule formation or during the early phases of nodule formation were not collected. The data question the currently accepted natural history of goitrogenesis for a subset of nodular thyroid glands, but the development of new pathophysiologic models requires a prospective study, ideally beginning prior to the development of any thyroid nodules.
In summary, the results suggest that in patients of this type, the growth of thyroid nodules may be a local process, not associated with growth of the surrounding non-nodular tissue. In the majority of patients, the size of the thyroid gland will not meet the criteria for classification as goiter, even if one or more of the nodules are growing or stable. For that reason, it is suggested that the term “nodular goiter” is a misnomer in these cases. While use of this term continues to be utilized in textbooks (4 –7) and guidelines (10), it is felt that this condition should be distinguished from “uni- or multinodular goiter” and referred to more appropriately and more informatively as a “uni- or multinodular thyroid gland.”
Footnotes
Acknowledgments
Funding for the study was provided by Banca d'Italia, the Italian Thyroid Cancer Observatory (ITCO) Foundation, and the Fondazione Umberto di Mario. None of the funding sources had any role in the design of the study; the collection, analysis, or interpretation of data; or the approval of the final version of the manuscript. The authors thank all the members of the Italian Thyroid Cancer Observatory (ITCO) Foundation.
G.G. and L.L. contributed to this paper as recipient of the PhD program of Biotechnologies and Clinical Medicine of the University of Rome, Sapienza. D.S.C. contributed to this paper as recipient of the “Visiting Professor for research activities 2015” grant at University of Rome, Sapienza (ID number: C26V157CMC). Writing support was provided by Marian Everett Kent, BSN.
Author Disclosure Statement
The author reports no conflicts of interest in this work.