
Abstract
Background:
Well-differentiated thyroid carcinoma (WDTC) has a high predilection for regional metastatic spread. Rates for WDTC lateral neck recurrence are reported to be as high as 24% in patients after initial thyroidectomy, lateral neck surgery, and adjuvant radioactive (RAI) iodine treatment. The objective of the study was to evaluate the efficacy, safety, and long-term outcome of comprehensive lateral neck dissection (LND) of levels II–V for recurrent or persistent WDTC in a tertiary referral center.
Methods:
This study retrospectively analyzed the standardized approach of LND for recurrent WDTC in the lateral neck compartment. Survival was analyzed by Cox regression analysis.
Results:
Three hundred and seven patients underwent 429 LND for cytopathology-confirmed lateral neck recurrent WDTC at the University of Texas MD Anderson Cancer Center between 1994 and 2012. The vast majority (90%) of patients were originally treated elsewhere. Multilevel lateral neck dissection had been originally performed in 80% of patients, with 17% having undergone at least two previous operations. Two hundred and sixty-seven (87%) patients had previous RAI. The most common levels of recurrence were levels III and IV (33% and 33%, respectively). Postoperative complications were seen in 7% of patients. Median follow-up was 7.2 years. In-field lateral neck control was 96% at 10 years. Overall lateral neck regional control, overall survival (OS), and disease-specific survival (DSS) at 10 years was 88%, 78%, and 91%, respectively. When stratifying by age (<24 years, 24–50 years, and >50 years), OS and DSS was significantly better in patients <50 years (OS: p < 0.001; DSS: p < 0.001). However, there was worse overall lateral neck control in the younger group (<24 years; p = 0.04). Regional recurrence after salvage LND occurred within a median time interval of 20.0 months (2.9–121.3 months), of which 2% (8/429) developed in-field lateral neck recurrences. Of those with any lateral neck recurrence after salvage LND, 24/30 (80%) patients successfully underwent another LND, resulting in an ultimate 98% lateral neck regional control rate.
Conclusions:
Expert comprehensive LND of levels II–V is associated with few perioperative complications and results in very high in-field regional control rate and ultimate lateral neck control in recurrent/persistent WDTC.
Introduction
W
Salvage neck dissection is a challenge and increases surgically associated complications, leading some surgeons to consider super-selective neck dissection to manage only the known disease. More limited compartment-focused approaches have been shown to have increased rates of in-field recurrences in the primary management of regional metastasis in WDTC. However, the role of a comprehensive salvage LND for lateral neck regional recurrences has not been adequately studied (11).
Clayman et al. have previously shown the efficacy of a comprehensive salvage central neck dissection (12). The purpose of this study was to evaluate the role and outcomes of a comprehensive LND for salvage in WDTC, specifically to identify the efficacy, safety, and long-term outcome of LND of levels II–V as salvage therapy for WDTC in a high-volume interdisciplinary thyroid cancer clinical and research program.
Materials and Methods
Patients
A retrospective longitudinal study at a single tertiary care center was performed on patients treated with comprehensive LND of levels II–V for regionally recurrent WDTC from September 1994 to February 2012. The years of the study were chosen because of homogeneity in patient evaluation and surgery approaches, and to provide adequate long-term follow-up.
Patients were identified by a search of the Physician Referral Service database of surgical records at the University of Texas MD Anderson Cancer Center that identified all patients who underwent any type of compartment-oriented LND, including radical neck dissection, modified radical neck dissection (removal of involved structures), and compartment-oriented LND (levels II–V). Inclusion criteria included patients of any age who had a histologically confirmed WDTC in the lateral neck following definitive surgical management. This study was reviewed and approved by the University of Texas MD Anderson Cancer Center Institutional Review Board.
Surgical evaluation, approach, and postoperative care
All patients who present to MD Anderson for thyroid cancer care are evaluated by a multidisciplinary team, including the head and neck/endocrine surgeon and an endocrinologist. All patients undergo preoperative laboratory evaluation (thyroglobulin [Tg], thyroglobulin [anti-Tg] antibodies, and thyrotropin [TSH]) and imaging (computed tomography [CT] neck with contrast and/or ultrasound). Lymph nodes that are suspicious are biopsied under ultrasound guidance. Furthermore, all patients undergo a complete head and neck examination with laryngeal exam (indirect mirror or flexible laryngoscopy) to assess baseline laryngeal function. Positron emission tomography (PET)-CT imaging was not utilized in the earlier years of this study and is not routinely employed in patients enrolled more recently. All patients underwent surgery based upon recommendations of the interdisciplinary endocrine oncology planning program.
The operative report was reviewed to determine the adequacy of the comprehensive LND and to note extended resections (i.e., sternocleidomastoid muscle, internal jugular vein, spinal accessory nerve, etc.). A comprehensive LND is the standard of care at this institution, and is defined as a compartment-oriented LND of levels II–V with the intent for resection of all gross disease (at least a R1 resection). The exceptions and nuances to a safe LND are avoidance of IIb, unless there is clinical or radiographic evidence of IIa involvement. This limits the extensive mobilization of the spinal accessory nerve. Medial dissection to the jugular vein, hypoglossal plexus, and subdigastric is necessary for all patients with level II or III disease. Particular attention is paid to level IV; anteriorly the posterior carotid sheath must be dissected to address the carotid/vertebral nodal basin and inferiorly to the transverse cervical artery. This includes the anterior aspect of level VB and the subclavian vein lymph nodes at the jugular/subclavian junction. Level Va is not routinely dissected in the absence of radiographic apparent disease. If nodal disease is identified by ultrasound or CT imaging in specific levels outside II–V, then that specific level(s) is included in the LND.
Postoperative care involved drain management and monitoring of acute and delayed complications. Complications of interest were hematoma or chyle leak that required operative take-back to the operating room, stroke, injuries to the carotid artery, nerve damage (spinal accessory nerve, vagus nerve, recurrent laryngeal nerve, phrenic nerve, and/or sympathetic trunk), damage to the pharyngo-laryngeal/esophageal complex, delayed shoulder dysfunction, gastrostomy tube dependency, and/or airway compromise requiring either intubation or tracheostomy. Long-term postoperative surveillance involves serial examinations, laboratory evaluation of TSH and Tg/anti-Tg antibodies, and high-resolution ultrasound and/or CT, with ultrasound-guided fine-needle aspiration (FNA) used for any new or concerning lymph nodes.
Lateral neck recurrence
Any concern for lateral neck recurrence was based on clinical exam, imaging, and/or elevated Tg levels and confirmed with FNA. If the recurrence was surgically resectable and the patient was medically capable of undergoing surgery, then an additional salvage surgery was performed. Out-of-field recurrence was defined as a regional recurrence that occurred outside of the initial salvage LND levels (standardly levels IIa, III, IV, and Vb). In-field recurrences were defined as a regional recurrence identified either in the previously dissected neck levels (at a minimum of levels IIa, III, IV, and Vb). Overall lateral neck regional recurrence was defined as any histologically confirmed lateral neck recurrence, independent of laterality or level relative to the previous comprehensive salvage LND.
Data collection and statistics
Lateral neck regional control was based on the disease-free status (no clinical or radiographic evidence of lateral neck disease) of the lateral neck after salvage LND and is defined as the time from the initial salvage lateral neck surgery at MD Anderson until their last follow-up or a lateral neck histologically confirmed regional recurrence. Then the status of the patient was analyzed based on overall, in-field, and out-of-field lateral neck recurrence, as described above. Death or loss to follow-up was censored. OS was defined as time from initial salvage surgery at MD Anderson until death; loss to follow-up was censored. Disease-specific survival (DSS) was calculated based on the time of initial salvage surgery at MD Anderson until death from thyroid cancer; non-cancer related deaths and loss to follow-up were censored.
Descriptive statistics for scaled values and frequencies of study patients within the categories for each of the parameters of interest were enumerated with the assistance of commercial statistical software (Statistica v12; Dell Statistica, Tulsa, OK). Correlations between parameters and endpoints were assessed by Pearson's chi-square or, where there were <10 subjects in any cell of a 2 × 2 grid, by Fisher's two-tailed exact test. Curves describing overall and DSS and recurrence-free intervals were generated by the Kaplan–Meier product limit method. The statistical significance of differences between the actuarial curves was tested by the log-rank test. p-Values of <0.05 were considered statistically significant. Hazard ratios for variables found by log-rank test to be significantly correlated with endpoints were estimated by Cox regression analysis. Multivariate analysis was performed via Cox regression analysis. Follow-up time was the time from the date of the comprehensive LND for recurrent thyroid cancer at the University of Texas MD Anderson Cancer Center until the date of last contact or death for survival measurements, from date of LND to first post-salvage recurrence, death or last contact for disease-free survival measurements, and from lateral neck dissection to first post-salvage recurrence or last contact for measurements of recurrence-free intervals. These statistical tests were performed with the assistance of the Statistica v12 software application.
Results
Demographics
Three-hundred and seven patients with recurrent WDTC who underwent comprehensive LND at MD Anderson between 1994 and 2012 met the inclusion criteria for the study and are described in Table 1. There was a female preponderance (60.9%), and the vast majority (89.6%) were treated originally elsewhere. All patients had some prior treatment to the lateral neck. Lateral neck dissection was originally performed in 79.5% of patients, and 86.9% of patients had previous RAI, while none had previous external beam radiation. Pathology review at MD Anderson from the most recent surgery or biopsy prior to the salvage neck dissection confirmed were all WDTC; 99% (303/307) were PTC, with only 1% (4/307) being follicular thyroid carcinomas. Seventeen percent (n = 52) of patients had already undergone two or more operative procedures for persistent or recurrent disease in the lateral neck, and 44 (14.4%) had distant metastases at presentation. Median follow-up was 7.2 years from the salvage LND performed at MD Anderson for this study.
RAI, radioactive iodine; MDACC, MD Anderson Cancer Center.
Neck dissection and pathologic findings
Neck dissections and pathologic findings are described in Table 2. Four hundred and twenty-nine lateral necks were dissected. A compartment-oriented LND was the most common type. Sixty-five (15.2%) patients presented with aggressive regional disease requiring extended resection of adjacent neck structures (internal jugular vein, sternocleidomastoid muscle, recurrent laryngeal nerve, spinal accessory nerve [SAN] and/or phrenic nerve. Table 2 lists them as radical neck dissection, modified radical neck dissection, or extended selective neck dissections based upon these extended components requiring resection. There was pathologic transformation of three previously diagnosed WDTC to poorly differentiated carcinomas.
Level not routinely dissected; only if clinical concern for disease.
ECS, extracapsular spread.
Locations of lateral neck regional recurrences are shown in Table 2. All LND specimens had at least one positive node, with nearly 70% having extracapsular spread (ECS). The most common levels of recurrence were levels III and IV (32.5% and 32.5%, respectively). While levels I and V had regional documented disease in 14% and 20% of cases, respectively, this does not represent a true potential for untreated metastatic spread to these levels, since most patients had undergone prior LND, and level I was only dissected if clinical and/or radiographic findings were concerning for disease.
Complications
Postoperative complications were seen in 21 (7.1%) patients. The most common complications were chyle leak (2.3%) and hematoma (2.3%). Despite 91% of patients undergoing a level II dissection, no patients with intent to spare the SAN described permanent SAN paralysis, with only one (0.2%) having a significant transient weakness. There were no perioperative deaths or strokes.
Follow-up and adjuvant therapy
Preoperatively, 163 patients had serologic evidence of disease and no evidence of distant metastases. The remainder either had Tg antibodies or presented with distant metastasis. Postoperatively, 66% of these previously Tg-positive patients (no Tg antibodies) and no evidence of distant disease were biochemically without evidence of disease. Similarly, 81.3% of patients who underwent postoperative diagnostic RAI uptake scan had negative studies. Therapeutic RAI was given to 59 (19%) patients of patients, and adjuvant external beam radiation was given to 33 (10.9%) patients, with 65.5% of these via intensity-modulated radiation therapy. Only 2% underwent concurrent chemoradiation.
Outcomes: regional neck control
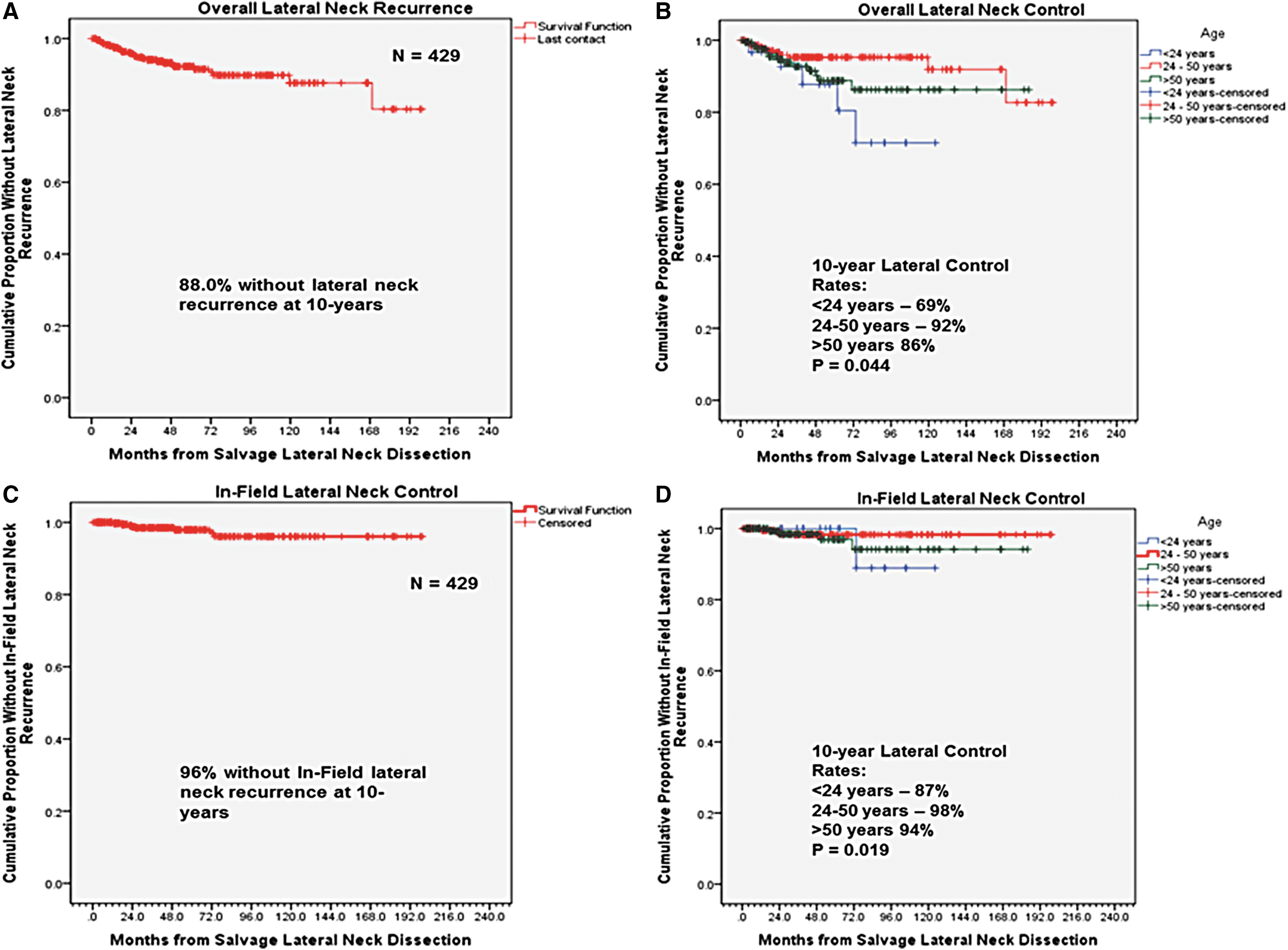
Overall lateral neck regional control was 91% at five years and 88% at 10 years (Fig. 1A). When evaluated by age and sex, only age, stratified by tertiles (<24 years, 24–50 years, and >50 years; Fig. 1B) was significantly correlated with differences in lateral neck regional control rates (69%, 92%, and 86%, respectively). Younger age (<24 years) was significantly associated with worse regional control (p = 0.005). Presentation with more than two prior surgical interventions also predicted significantly worse regional control compared to those who presented with fewer recurrences (70.0% vs. 89.3%, respectively; p = 0.021). Evaluating pathologic predictors of recurrence identified no differences in regional control based on type of neck dissection (p = 0.862), number of lymph nodes removed (p = 0.527), extracapsular spread (p = 0.455), resection of adjacent structures (p = 0.645), soft-tissue invasion (p = 0.181), invasion of adjacent structures (p = 0.778), or perineural invasion (p = 0.808). More than two positive lymph nodes trended toward worse regional control (81% vs. 90%; p = 0.0521), and the presence of lymphovascular invasion was associated with higher rates of regional recurrence (100% vs. 0%; p < 0.001). The significance of lymphovascular invasion may be biased, as this variable was only reported in 6% (26/429) of cases, with 92% (24/26) of those being in the regional recurrence group. Its significance needs to be further investigated. Adjuvant therapy was given based on risk of recurrence, and there was no difference in regional recurrence based on adjuvant RAI, radiation, or chemotherapy (p = 0.361, p = 0.554, and p = 0.886, respectively). Only elevated postoperative Tg significantly predicted regional recurrence (p = 0.016). On multivariate analysis, only age <24 years and detectable postoperative Tg levels were significantly associated with lateral neck regional failure after salvage neck dissection (Table 3).
Kaplan–Meier survival curves. (
HR, hazard ratio.
Regional recurrence after salvage LND occurred within a median time interval of 20.0 months (2.9–121.3 months), of which 1.9% (8/429) recurred in-field and an additional 5.1% (22/429) developed a recurrence outside of dissected levels II–V, thus giving a 96% in-field regional control rate at 10 years (Fig. 1C). When stratified by age (tertiles; Fig. 1D), there was a significant difference in in-field lateral neck control rates (p = 0.02; 87%, 98%, and 94%, respectively). The location of regional recurrences is described in Table 4. Of those with a lateral neck regional recurrence, level II was the most common level of recurrence overall, and all were out of field (contralateral neck). In-field recurrences most often occurred in level IV. Of the 30 patients who developed a lateral neck regional recurrence, 24 were followed long-term at MD Anderson, and 17/24 (71%) patients underwent a subsequent salvage LND, resulting in an overall 98% lateral neck regional control rate at 10 years. Of the three patients who had transformation to poorly differentiated carcinoma, none recurred in the lateral neck.
Some patients had more than one level with a recurrence, and 24/30 recurrences had nodal levels available.
All out of field recurrences in levels II–IV occurred in the contralateral neck.
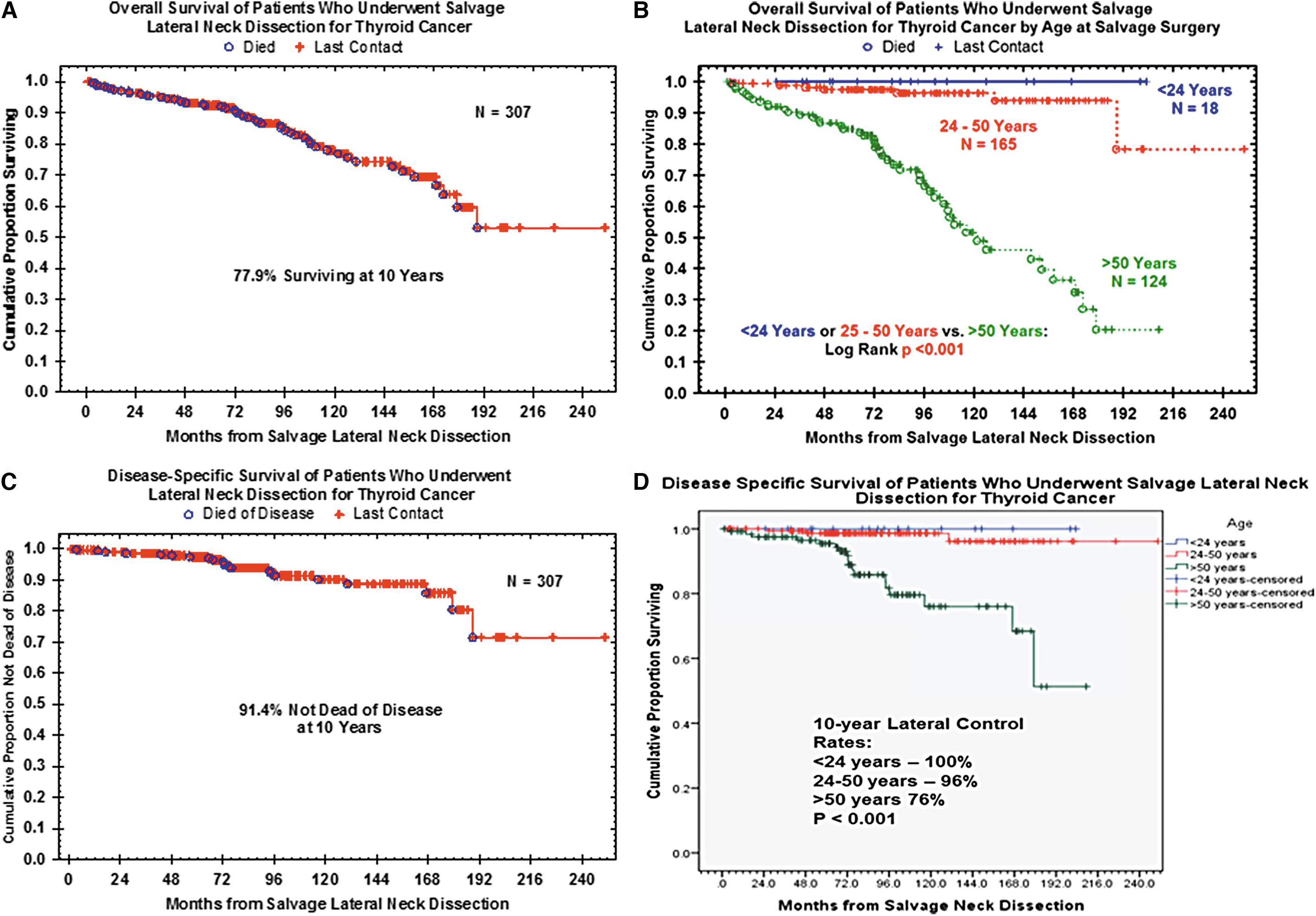
OS at 10 years was 77.9% (Fig. 2A). Table 5 demonstrates univariable analysis; age >50 years (Fig. 2B) and male sex were significantly associated with worse OS (p < 0.001 and p = 0.033, respectively). Presentation with more than two previous resections and the presence of distant metastasis (previous or found during surveillance) was associated with worse OS (p = 0.004, p < 0.001, and p < 0.001, respectively). Postoperative pathologic analyses identified ECS as a risk factor for death (p = 0.025), as well as presentation with or development of distant metastasis (p < 0.001 and p = 0.016, respectively). There was no difference in OS with regards to number of presence of prior operations of the lateral neck or number of positive nodes. However, positive nodes >1 cm were associated with worse OS (p = 0.031). Soft-tissue invasion was also associated with worse OS (p = 0.017). Adjuvant RAI had no effect on OS, whereas patients who underwent adjuvant radiation and/or chemotherapy had worse OS (p < 0.001 and p < 0.001, respectively). On multivariate analysis (Table 3), only age >50 years and any detectable postoperative Tg levels were significantly associated with death after salvage LND.
Kaplan–Meier survival curves. (
NC, not calculated; Tg, thyroglobulin; XRT, radiation; DM, distant metastasis; LND, lateral neck dissection.
Overall DSS in the cohort was 91.4% at 10 years (Fig. 2C). When stratified by age (tertiles; Fig. 2D), only the older age group (>50 years) was associated with worse DSS (p < 0.001). Male sex was not associated with worse DSS (p = 0.887). Similar to OS and regional control, more than two previous operations was associated with worse DSS (p = 0.006). As expected, the presence of distant metastasis (previous or found during surveillance) was associated with worse DSS (p < 0.001 and p = 0.025, respectively). Pathologically, ECS, number of positive nodes, size of positive nodes, and soft-tissue invasion were not associated with worse DSS. The presence of ECS trended toward significantly worse DSS (87% vs. 99%; p = 0.08). Adjuvant RAI did not affect DSS. Adjuvant radiation and/or chemotherapy carried a worse DSS (55% vs. 94%, p < 0.001; 0% vs. 92%, p < 0.001, respectively). On multivariate analysis (Table 3), only age >50 years and postoperative Tg levels were significantly associated with disease-specific death following LND.
Discussion
More than two decades ago, the senior author of this work began to emphasize the management of recurrent or persistent thyroid cancer within the multidisciplinary program at a tertiary referral center. As a result of this emphasis, a large number of patients with recurrent disease were referred for surgical management of local and regional recurrent thyroid cancer. The long-term outcomes of central compartment surgery for recurrent/persistent differentiated thyroid cancer have been previously reported to help to establish the extent of surgery required and the expected achievable outcomes (12). Until this point in time, no long-term analysis of the outcomes of comprehensive compartment-oriented LND for recurrent or persistent differentiated thyroid cancer have been published. This was the purpose of this investigation.
This study demonstrates that in highly experienced hands, comprehensive salvage LND is a safe and highly effective treatment, with an overall 98% in-field control rate, despite extensive prior surgery, scarring, and reported historical adverse pathologic findings. Essentially, surgery is an incredibly effective management of even the most extensive regional recurrent or persistent differentiated thyroid cancer among highly experienced thyroid cancer surgeons.
Recently, McNamara et al. reviewed their experience with LND for metastatic PTC (11). In the primary setting, they compared a super-selective (III–IV) neck dissection (SSND) with LND (II–V). There was no difference in overall regional recurrence (LND 94.4% vs. SSND 89.4%; p = 0.0158), but regional control in the dissected neck was significantly improved in the LND group (LND 97.7% vs. level II and IV only 89.4%; p < 0.001). The in-field regional control rate (96%), despite a salvage setting, is nearly identical, and the ability to salvage out-of-field recurrences led to an overall 98% regional control rate, which is comparable to their rate in the primary setting. The rationale for comprehensively dissecting levels II–V is further supported by findings by Ahmadi et al. who identified a higher prevalence of regional metastasis in level II, III, and IV (45%, 57%, and 60%, respectively) in both the primary and recurrent setting (13). The present study found that of the 30 regional recurrences, only 5% (22/429) were out of field. The data confirm the need to perform a compartment-oriented LND, addressing levels II–V, and only dissecting additional regions if there is clinically or radiographic evidence of disease in both the primary or salvage settings.
Recently, Chereau et al. described their experience and found after super-selective neck dissection (levels III and IV), they had a 71% regional recurrence/persistence in level II (10). They then performed a single-level dissection for salvage. They also demonstrated a worse disease-specific mortality in the re-operative group compared to the non-re-operative group (9.4% vs. 1.5%; p < 0.01). Unfortunately, they did not describe their regional control after salvage. While the present study demonstrates no significant difference in survival relative to the literature, the regional control in the lateral neck is excellent. With nearly one third of patients in this study undergoing at least two or more prior surgical procedures, it suggested in fact that a population of thyroid cancer patients at high risk for both complications due to scaring as well as recurrence had been selected. Nevertheless, the excellent control of lateral neck disease and low complication rates compare favorably to regional control outcomes for primary LND for WDTC (11).
In the authors' practice, all patients with lateral neck disease for WDTC undergo a comprehensive level II–V dissection. The neck dissection for thyroid cancer is not the neck dissection for non-thyroid malignancies (i.e., mucosal disease), and this is an important component of any discussion of management of lymph node disease in thyroid cancer. The following areas must be comprehensively addressed in the neck dissection for thyroid cancer: (i) Level IV including the subclavian lymph nodes and transverse cervical lymph nodes; (ii) Level Vb posterior to the sternocleidomastoid muscle; (iii) Level III and IV posterior to the carotid removing the carotid/vertebral lymph nodes; (iv) Level II in the subdigastric area anterior to the internal jugular vein comprehensively dissecting the hypoglossal nerve and lymphatics extending inferiorly through to the superior thyroid artery takeoff and lymphatics (junction of level VI superiorly); (v) Level IIa, comprehensively identifying but not mobilizing the spinal accessory nerve unless level IIa is involved grossly or in case of ultrasonographic evidence of disease.
Outstanding regional control in the salvage setting, despite multiple surgeons included in the study, confirms that the approach to the lateral neck is feasible and reproducible among experienced thyroid cancer surgeons.
Patients undergoing comprehensive LND for differentiated thyroid cancer can certainly develop recurrences in the lateral neck outside of the routinely dissected levels II–V. In fact, the data confirm that this occurs much more frequently than “in-field” recurrences (1.9% vs. 5%). However, given the low rate of out-of-field recurrence and the fact that these out-of-field recurrences are often unpredictable, an approach of active surveillance and then appropriate compartmental dissection of recurrent disease is proposed. Similarly, excellent lateral neck control rates are demonstrated after revision-salvage surgery. This has been our programmatic approach and affords an excellent long-term outcome for control of cervical disease.
Patients who presented with three or more previous operations had significantly worse OS, DSS, and regional control compared to those with fewer recurrences. This suggests that in the salvage setting, presentation with up to two prior operations, survival outcomes are comparable to those with fewer or no previous recurrences. Although salvage LND can successfully manage regional recurrences, if the patient has had three or more previous operations, survival is negatively impacted. This is likely related to the increasing challenge with identifying and eradicating nodal disease in repeatedly operated necks. This further supports the comprehensive LND as either the initial treatment in patients with lymph node involvement, or for the initial salvage surgery by highly experienced thyroid cancer surgeons.
The significant factors that were associated with regional failure were age <24 years, more than two previous operations, postoperative RAI, and the presence of distant metastasis prior to LND. The latter two variables may be explained by a more aggressive tumor biology. One of the major findings was that young patients (<24 years) had worse regional control but this had no effect on survival. At times, a less aggressive surgical approach in young patients with extensive soft tissue invasion may lead to increased regional failure but has no effect on survival. There may be instances, particularly in prepubescent and adolescent thyroid cancer patients, where less aggressive surgery, even allowing for persistent disease, may be considered among highly experience thyroid cancer surgeons, since RAI may be beneficial in a subset of these patients. Such decisions must only be made by the most experienced thyroid cancer teams. A decision for a surgeon to leave grossly detectable thyroid cancer in the neck is very rarely indicated. This decision is most commonly seen when surgical soft-tissue extension is encountered by inexperienced surgeons ill-prepared for such findings. This is a nuanced understanding of the disease process that performing an R1 resection in young patients has limited effect on survival and aggressive surgery may negatively affect quality of life. However, in older patients, persistent disease increases the risk of recurrence and survival. Despite worse regional control, young patients (<24 years) did not have any worse DSS or OS compared to older patients. In older patients, regional recurrence increased the risk of distant metastasis, which has a negative effect on survival.
Some of the variables that were expected to affect regional control were not significant. The number of lymph nodes removed was not significant, as this is often used as a marker of the quality of the neck dissection (14). In the salvage setting, the nodal basins have frequently already been partially addressed. This inherently reduces the number of lymph nodes available for dissection, and the number of removed lymph nodes may not be a good marker in the salvage setting. Similarly, ECS and soft-tissue extension had no effect on regional failure but was associated with worse OS and DSS. Therefore, a comprehensive LND, addressing all invasive disease, is effective in controlling reportedly pathologically adverse WDTC. Cases of super-selective neck dissection are not available to compare to a more comprehensive LND, as this is against the authors' practice principles, but the high rates of regional control and limited complications strongly suggest that this is a safe and efficacious practice.
From a complication standpoint, chyle leak was the most common complication, and this was observed in 3% of cases. A higher chyle leak rate is expected as part of the LND due to extensive dissection in level IV in the carotid/vertebral artery basin. Carotid-vertebral lymph nodes must be considered a primary echelon of lateral neck metastasis in thyroid cancer, and therefore this area must be addressed. Meticulous intraoperative dissection of the thoracic duct and other chylous vessels are required in LND for thyroid malignancies. Hematoma was the next most common complication and consistent with reported outcomes (15). No long-term SAN nerve dysfunction or any damage to the phrenic nerve or cranial nerves X or XII was observed. Polistena et al. looked at their complication rate after LND for thyroid cancer and reported similar complication rates (15).
While OS and DSS were not the main focus of the study, age >50 years, male sex, more than two previous recurrences, ECS, adjuvant external beam radiation and/or chemotherapy, and presence of distant metastasis were all associated with diminished survival. As expected, the presence of distant metastasis at time of presentation or during surveillance was significantly associated with poor OS and DSS. More pertinent to this study is the finding that lateral neck regional failure also predicted distant metastasis in patients >50 years of age, again confirming the importance of appropriate surgical management for disease control.
In conclusion, salvage LND of levels II–V is safe and effective surgical therapy for persistent or recurrent differentiated thyroid cancer in the lateral neck among experienced thyroid cancer surgeons. It is further suggested that recurrent/persistent thyroid cancer surgery should be performed by the most experienced thyroid cancer surgeons to afford patients the greatest opportunity for long-term control and reduced morbidity.
Footnotes
Author Disclosure Statement
None of the authors have any conflicts or disclosures.