
Abstract
Background:
There are currently no reliable biomarkers to predict relapse in Graves' disease (GD). In the present study, we investigated novel diagnostic biomarkers to predict the long-term remission of or relapse in GD.
Methods:
A DNA microarray analysis was performed to examine gene expression in the peripheral leukocytes of a frequently relapsing patient with GD and a patient in long-term remission after the discontinuation of antithyroid drugs (ATDs). Based on the DNA microarray analysis, we focused on Sialic acid-binding immunoglobulin-like lectin1 (SIGLEC1) as a candidate novel biomarker to predict GD relapse. Three hundred and fifty-eight patients with GD in the thyroid clinics of four different hospitals in Japan were included in a cross-sectional study to establish whether SIGLEC1 mRNA levels distinguish GD relapse experience from long-term remission. An additional 55 patients with GD were enrolled in a prospective study to clarify whether SIGLEC1 mRNA levels at ATD discontinuation predict GD relapse.
Results:
SIGLEC1 mRNA levels were significantly higher in patients with GD relapse experience than in those in long-term remission. Based on the receiver operating characteristic analysis, we found that high SIGLEC1 mRNA levels (≥258.9 copies) significantly distinguished GD relapse experience from long-term remission (p < 0.0001; sensitivity 66.7%, specificity 70.1%). In the prospective study, when the optimal cutoff value from the receiver operating characteristic curve analysis was applied to SIGLEC1 mRNA positivity at ATD discontinuation, SIGLEC1-positive patients (≥258.9 copies) showed a significantly higher cumulative risk of relapse than SIGLEC1-negative patients (<258.9 copies) (p = 0.022, the log-rank test).
Conclusions:
SIGLEC1 mRNA levels have potential as a novel predictive biomarker for GD relapse.
Introduction
G
Predictions of the clinical outcomes of GD are important for minimizing the rate of relapse and associated adverse effects of ATD therapy and providing patients with appropriate treatment options prior to the initiation of ATD therapy. TRAb titers and thyroid blood flow measured by ultrasonographic assessments may contribute to the selection of prophylactic thyroid surgery or radioiodine ablation. However, there are currently no reliable biomarkers to predict GD relapse.
Sialic acids are a family of sugars typically found attached to the exposed terminal portion of glycan molecules on the cell surface (3). Moreover, sialic acids play a significant role in the proliferation of cells in and secretory activity of the thyroid gland (4). A previous study reported a significant increase in sialic acid expression on the luminal membranes of follicular cells in the thyroid gland of patients with autoimmune thyroiditis such as GD and Hashimoto thyroiditis (5).
SIGLEC1 (sialic acid-binding immunoglobulin-like lectin1)—also known as sialoadhesin or CD169—is a sialic acid-binding receptor, a monocyte/macrophage-restricted cell surface protein that has a number of functions in the immune system, such as cell-to-cell interactions, antigen presentation, and pathogen capture (6). SIGLEC1 expression in human monocytes is predominantly induced by type 1 interferon (IFN) and is weakly induced by type 2 IFN (IFN-γ) (7). There is increasing evidence to show that Siglecs, particularly SIGLEC1, play important roles in the initiation and progression of inflammatory and autoimmune diseases (8). SIGLEC1 was identified in a cell-specific transcriptome analysis of patients with primary Sjögren's syndrome (9) and systemic lupus erythematosus (10). GD is also an autoimmune disease, and IFNs have been associated with its onset and development (11).
In this multicenter study, which included leading hospitals with clinics specializing in thyroid disorders in Japan, we explored novel diagnostic biomarkers to predict the long-term remission of or relapse in GD and provide the first evidence to show that SIGLEC1 mRNA levels in peripheral leukocytes may predict GD relapse.
Materials and Methods
Study design and participants
Twenty milliliters of peripheral blood were drawn from a 23-year-old female GD patient who frequently relapsed and a 55-year-old female patient who was in long-term remission. Total RNA was extracted and subjected to a DNA microarray analysis conducted by World Fusion (Tokyo, Japan) using the Affimetrix Expression Console™ (Affimetrix, Santa Clara, CA). Microarray data were normalized by MAS5.
The cross-sectional study included 358 patients (79 males and 279 females) with GD who visited the thyroid clinics of the Tokyo Medical and Dental University Hospital, Gunma University Hospital, Kuma Hospital (Kobe, Japan), and Ito Hospital (Tokyo) in Japan between August 2008 and April 2015. GD relapse experience was retrospectively reviewed through medical records or by interviews with patients. Patients who relapsed were categorized into the R group, and those who had been in long-term remission for 12 months or more after ATD discontinuation were categorized into the non-R group.
The prospective study included an additional 55 patients (13 males and 42 females) who were under observation for at least 12 months since ATD discontinuation with thyroid function tests performed on a regular basis.
Patients who had a previous history of collagen diseases, type 1 diabetes mellitus (T1D), or chronic hepatitis were excluded. We also excluded patients who tested positive for the anti-nuclear antibody and rheumatoid factor. Pregnant women and patients being treated with steroids were also excluded.
According to the guidelines issued by the Japan Thyroid Association (JTA) in 2006 for the treatment of GD, ATDs (i.e., MMI and PTU) are discontinued when serum free thyroxine (fT4) and TSH concentrations have been maintained within the reference range for at least 6 months after treatment with the minimum maintenance dose (5 mg MMI or 50 mg PTU every other day) (12).
Patients were considered to have relapsed when their serum fT4 levels were greater than the reference range and TSH levels decreased to less than the reference range. Patients were considered to be in remission if they had normal serum TSH and fT4 for 12 months after ATD discontinuation (13), while patients whose thyroid function was maintained in the euthyroid state after transient thyrotoxicosis were regarded as remission cases. Thus, patients were followed up for at least 12 months after ATD discontinuation.
This study was approved by the Ethical Committees of all four facilities, and written informed consent was obtained from all patients.
Thyroid function tests
In all patients enrolled in the present study, serum fT4, free triiodothyronine (fT3), and TSH levels were measured using chemiluminescence assays (ECLusis fT4, fT3, and TSH; Roche Diagnostics Ltd., Basel, Switzerland). Their reference ranges were: TSH, 0.5–5.0 μIU/mL; fT3, 2.30–4.30 pg/mL; and fT4, 0.90–1.70 ng/dL. TRAb levels were also measured by chemiluminescence assays (ECLusis TRAb, Roche Diagnostics Ltd.), and a serum concentration greater than or equal to 2.0 IU/L was considered to be positive.
Study procedures
Peripheral blood (7 mL) was collected in Vacutainer tubes containing EDTA-2Na followed by total RNA extraction from nucleated cells (leukocytes) by SRL Inc. (Tokyo, Japan). Complementary DNA was synthesized from 0.5 μg of total RNA using real-time quantitative PCR (ReverTra Ace™ qPCR RT Master Mix Kit; TOYOBO, Osaka, Japan). Quantitative reverse transcription (qRT) PCR for SIGLEC1 mRNA levels was performed using TaqMan™ Gene Expression Assays (sialic acid-binding Ig-like lectin 1, sialoadhesin, Assay ID: Hs00988063_m1; Applied Biosystems, Carlsbad, CA). As an internal control, we measured glyceraldehyde-3-phosphate dehydrogenase (GAPDH) mRNA levels using TaqMan™ Gene Expression Assays (Assay ID: Hs02758991_g1, Applied Biosystems). We employed DNA constructs subcloned in pCR2.1-TOPO™ (Invitrogen) as reference standards for SIGLEC1 and GAPDH. Using the reference standards as a template (0.25, 0.5, 1.0, and 10 pg), we performed PCR and calculated the SIGLEC1/GAPDH ratio. We defined the ratio 1.0 as 25 copies of SIGLEC1 mRNA.
Serum SIGLEC1 concentrations in 100 μL of serum from patients were measured using the human sialic acid-binding immunoglobulin-like lectin-1, siglec-1 ELISA kit with a rabbit polyclonal antibody raised against human SIGLEC1 (USCNLIFE, Wuhan, China).
Statistical analysis
Continuous data were reported as the mean ± standard deviation if normally distributed and as the median and interquartile range (IQR) if not normally distributed. An analysis of variance, the Student's unpaired t-test, and nonparametric Mann–Whitney U-test were used where appropriate. Categorical data were represented as n (%) and analyzed using the chi-squared test, Fisher's exact test, or kappa statistic where appropriate. The kappa statistic is a standardized measure of the extent of agreement among different tests beyond that expected by chance alone. The kappa coefficient equals one if there is complete agreement, zero if the level of agreement is equal to the expected agreement due to chance alone, and a negative number if the observed agreement is less than the expected agreement due to chance (14). An analysis of receiver operating characteristic (ROC) curves was also performed to examine the sensitivity and specificity of SIGLEC1 mRNA values of the relapse experience. Optimal cutoff points were obtained from the Youden index. In addition, likelihood ratio (LR) test statistics were used to compare model fitting. We compared models with and without SIGLEC1 mRNA levels and conducted LR tests between the two models.
In the prospective study, the cumulative risk of relapse was estimated by the Kaplan–Meier survival analysis. The log-rank test was used to evaluate the significance of differences in two groups divided by the optimal cutoff point of SIGLEC1 mRNA calculated by the ROC curve analysis and the reference value of serum TRAb levels. Hazard ratio was calculated as the effect size. p-Values <0.05 were considered to be significant. In the statistical analysis, concentrations that were greater than and below the threshold of the assay were given specific values. TRAb levels <0.3 IU/L were recorded as 0 IU/L. TRAb levels >40 IU/L were recorded as 40 IU/L. All statistical analyses were performed using SPSS 23.0 for Windows (IBM Japan, Ltd., Japan) and a post hoc power analysis was conducted using Stata/SE 13.1 for windows (StataCorp LP, College Station, TX).
Results
DNA microarray analysis to examine gene expression in peripheral leukocytes of a frequently relapsing patient with GD and a patient in long-term remission
In order to identify novel diagnostic biomarkers with the potential to predict long-term remission or GD relapse, we employed DNA microarrays to examine gene expression in the peripheral leukocytes of a frequently relapsing patient with GD (R patient) and a patient in long-term remission after the discontinuation of ATDs (non-R patient). As shown in Table 1, the expression of several genes in peripheral leukocytes was significantly stronger in the GD patient who frequently relapsed than in the patient who was in long-term remission. Among these genes, two different probes indicated strong expression for SIGLEC1 mRNA only in the patient with frequent GD relapse (Table 1). Furthermore, as described above, since sialic acids are related to thyroid gland proliferation, we focused on SIGLEC1 in subsequent experiments.
The ratio indicates relative expression in the R group (patients who relapsed) vs. the non-R group (patients who had been in long-term remission for 12 months or more after ATD discontinuation).
SIGLEC1 mRNA levels in peripheral leukocytes are significantly higher in patients with GD relapse experience than in those who were in long-term remission
The clinical features of 358 patients for the cross-sectional study are summarized in Table 2. Serum TSH levels were significantly higher in the non-R group, which was in long-term remission after the discontinuation of ATDs, than in the R group, which had experienced GD relapse, for both males and females. In contrast, serum fT4, fT3, and TRAb levels were significantly higher in the R group than in the non-R group for both males and females. SIGLEC1 mRNA levels in peripheral leukocytes were significantly higher in the R group than in the non-R group for both sexes.
R and non-R values are given as mean ± standard deviation (SD) or median [interquartile range (IQR)].
p < 0.05, ** p < 0.01, *** p < 0.001.
fT3, free triiodothyronine; fT4, free thyroxine; SIGLEC1, sialic acid-binding immunoglobulin-like lectin1; TRAb, thyrotropin receptor antibodies; TSH, thyrotropin.
The distribution of SIGLEC1 mRNA levels in the non-R and R groups is shown in Fig. 1A (non-R group: median = 201.1, IQR 104.4 to 332.7; R group: median = 368.8, IQR 210.7 to 700.4; p < 0.001).
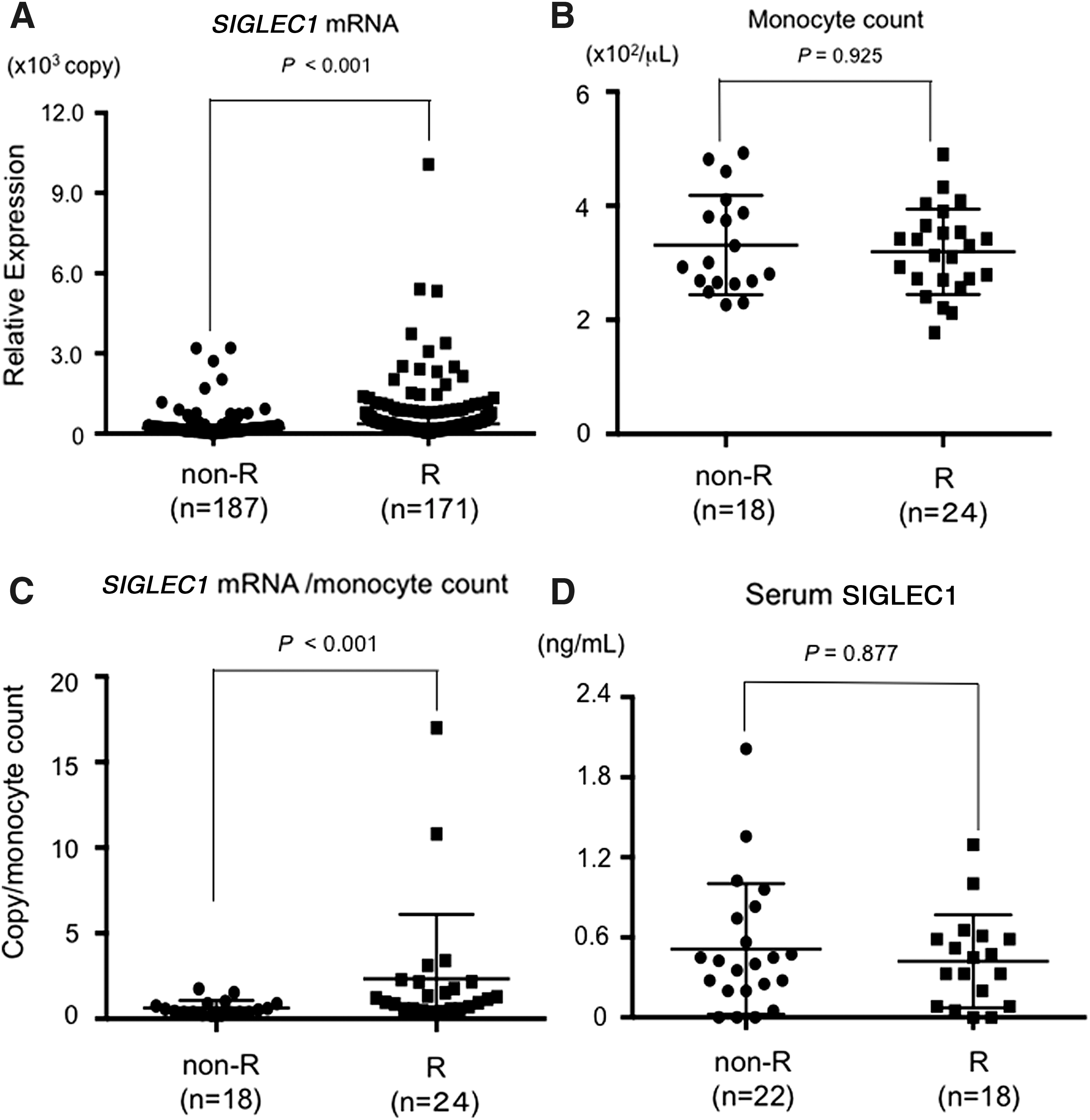
Distribution of sialic acid-binding immunoglobulin-like lectin1 (SIGLEC1) mRNA levels in peripheral leukocytes (
We evaluated differential white blood counts in some patients in both groups. No significant differences were observed in monocyte counts in peripheral blood between the non-R and R groups (Fig. 1B). We also adjusted SIGLEC1 mRNA levels with monocyte numbers and found that SIGLEC1 mRNA levels were significantly higher in the R group than in the non-R group (Fig. 1C).
A correlation was observed between SIGLEC1 mRNA levels and serum TSH, fT4, fT3, and TRAb levels (Table 3).
Serum SIGLEC1 concentrations were similar between R and non-R groups
We collected serum samples from some patients and measured serum SIGLEC1 concentrations. Serum SIGLEC1 concentrations were similar between the R and non-R groups (Fig. 1D) (non-R group: median = 0.414, IQR 0.20 to 0.766; R group: median = 0.389, IQR 0.084 to 0.594; p = 0.877).
Evaluation of the distinguishability of GD relapse experience by measuring SIGLEC1 mRNA and TRAb levels in a cross-sectional study
An ROC curve analysis was employed to clarify whether SIGLEC1 mRNA values measured in the course of GD distinguished GD relapse experience from long-term remission. The area under the curve of SIGLEC1 mRNA levels was 0.717, and the optimal cutoff value to significantly distinguish GD relapse was 258.9 copies (p < 0.001) with a sensitivity of 66.7% and specificity of 70.1% (Fig. 2). We performed a likelihood (LR) test and compared the distinguishability of GD relapse experience with and without SIGLEC1 mRNA levels. The −2 log-likelihood, which is a deviance, was 495.578 and 466.891 in the models with and without SIGLEC1 mRNA levels, respectively; therefore, the difference in the −2 log-likelihood between the models was 28.687. The LR test indicated that the difference was significant (p < 0.0001), suggesting that changes of SIGLEC1 mRNA levels are relevant.
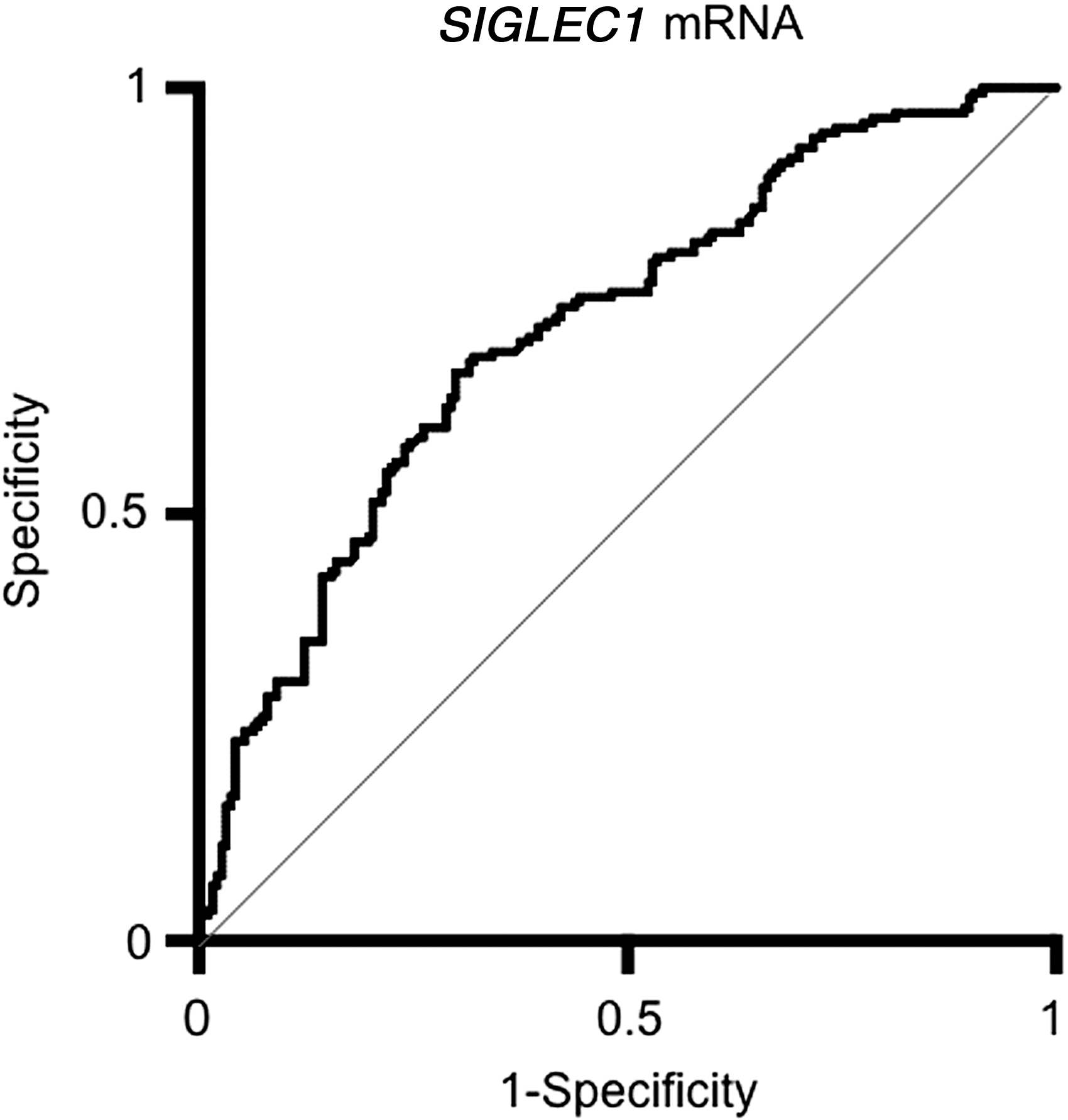
Receiver-operating characteristic analysis of SIGLEC1 mRNA levels. The areas under the curve for SIGLEC1 mRNA levels were 0.717 (95% confidence interval 0.665–0.770). Optimal cutoff value calculated by the Youden index method for SIGLEC1 mRNA levels was 258.9 (copies).
We dichotomized subjects in the cross-sectional study with the optimal cutoff value of SIGLEC1 mRNA levels (258.9 copies) obtained by the ROC analysis and the reference value of serum TRAb levels (2.0 IU/L), thereby constructing a cross tabulation for the R and non-R groups. We calculated the kappa statistic to assess concordance in the distinguishability of GD relapse experience between serum TRAb and SIGLEC1 mRNA levels. The kappa coefficients for the non-R and R groups were −0.099 and −0.055, respectively. Thus, even though a correlation was observed between serum TRAb and SIGLEC1 mRNA levels in continuous data (Table 3), no correlation was found between the two parameters in categorical data.
SIGLEC1 mRNA levels at ATD discontinuation may predict GD relapse
An additional 55 patients with GD (13 males and 42 females) were enrolled in a prospective study to examine whether SIGLEC1 mRNA levels at ATD discontinuation predict GD relapse. Eleven patients (3 males and 8 females) (20%) relapsed (R group) during the median follow-up period of 13.0 months (IQR 6.0 to 19.0), while 44 patients (10 males and 34 females) were in remission (non-R group). In the group of 11 patients that relapsed, ten were positive for SIGLEC1 mRNA, while the other was negative. On the other hand, in the non-R group of 44 patients, 22 patients (50%) were positive for SIGLEC1 mRNA. The median duration of the relapse-free period after ATD discontinuation was 31.5 months (IQR 24.0 to 59.0). No significant differences were observed in sex, age, or serum TSH, fT3, fT4, TRAb, or SIGLEC1 mRNA levels between the non-R and R groups (Table 4).
R and non-R values are given as mean ± SD or median [IQR].
When the optimal cutoff value estimated by the ROC curve analysis in the cross-sectional study was applied for SIGLEC1 mRNA positivity at ATD discontinuation, SIGLEC1-positive patients (n ≥ 258.9 copies) showed a significantly higher cumulative risk for relapse than SIGLEC1-negative patients (n < 258.9 copies) in the log-rank test (p = 0.022, hazard ratio = 7.508 [95% confidence interval (CI) 1.239 to 13.50]; Fig. 3A). However, when the reference value was applied to TRAb positivity after ATD discontinuation, no significant difference was noted in the cumulative risk of relapse between TRAb-positive (≤2.0 IU/L) and TRAb-negative (<2.0 IU/L) patients (log-rank test, p = 0.972, hazard ratio = 0.976 [95% CI 0.254 to 3.748]; Fig. 3B). In the prospective study, we hypothesized that a difference of 20% or more in the relapse rate may be detected between the two groups 60 months after ATD discontinuation. In a post hoc power analysis, the power for the hypothesis for a sample of 55 (R, n = 11; non-R, n = 44) was 0.814. Thus, the sample size employed for the prospective study was statistically appropriate to generate results.
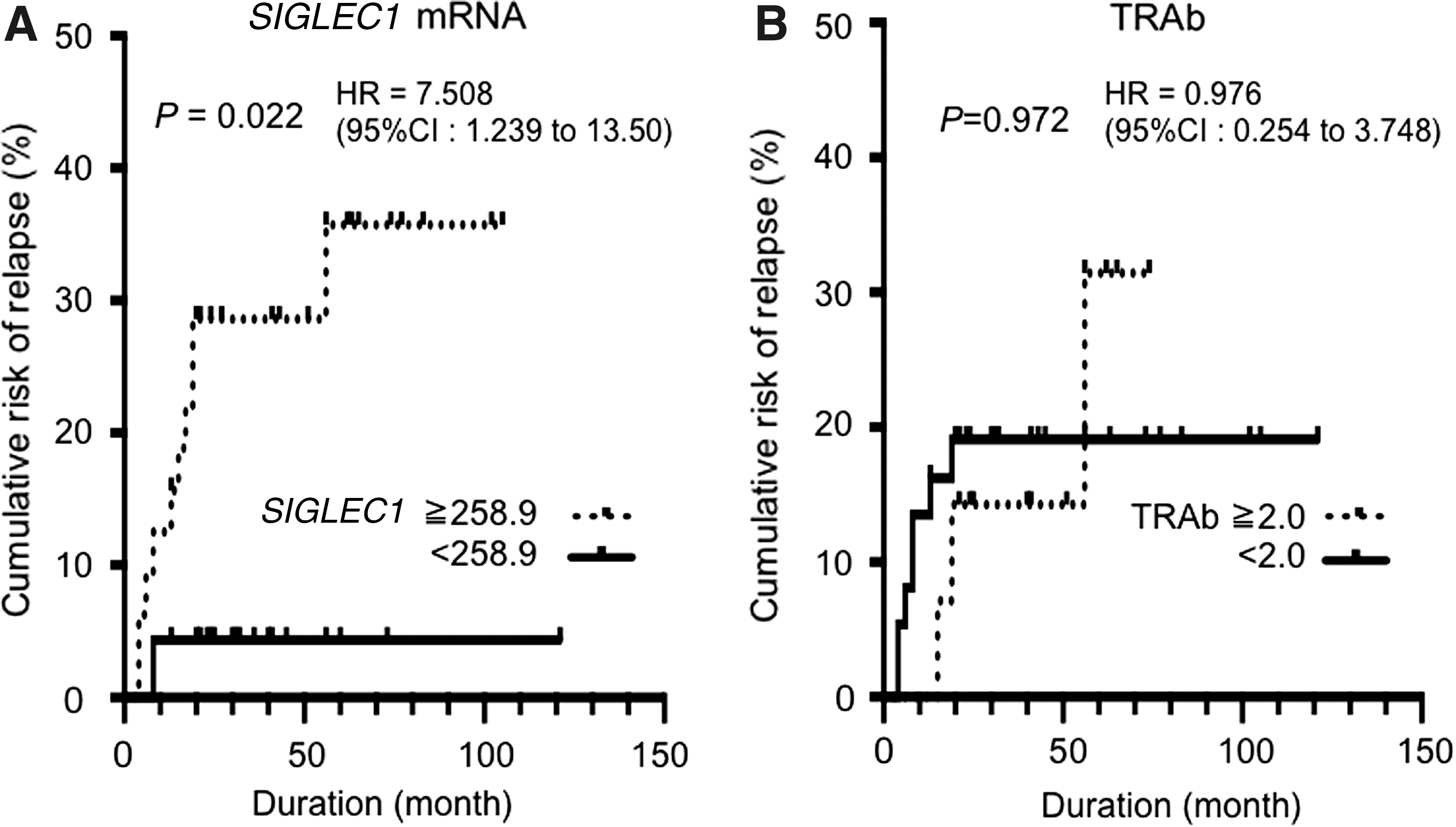
Cumulative risk (Kaplan–Meier method) of relapse in patients after discontinuation of antithyroid drugs: SIGLEC1 mRNA (
Alternations in SIGLEC1 mRNA levels in some individual cases
We also evaluated SIGLEC1 mRNA levels in some patients during the course of the disease (at diagnosis vs. 1 year after ATD administration, euthyroid state vs. upon relapse, at the first visit vs. 1 year later). Based on representative patient data (Table 5), SIGLEC1 mRNA levels, particularly when dichotomized into greater and less than the cutoff value (258.9 copies), did not appear to be affected by the thyroid status, such as remission and relapse.
Positive: SIGLEC1 ≥ 258.9; negative: SIGLEC1 < 258.9 (copies).
TRAb in first generation measurements (%), reference range: 0 ∼ 15%.
Discussion
This multicenter study consisted of cross-sectional and prospective studies. The cross-sectional study showed that SIGLEC1 mRNA levels in peripheral leukocytes were significantly higher in patients who had experienced GD relapse than in those in long-term remission.
Since Siglec1 is a monocyte/macrophage-restricted cell surface receptor (6), we adjusted SIGLEC1 mRNA levels in peripheral leukocytes with the monocyte count in some patients in the non-R and R groups. SIGLEC1 mRNA levels adjusted with the monocyte count were also significantly higher in the R group than in the non-R group (Fig. 1B, C), suggesting the appropriateness of SIGLEC1 mRNA levels in peripheral leukocytes in the present study.
SIGLEC1 mRNA expression is mainly induced by type 1 IFN. Type 1 IFN, such as IFNα and β, play critical roles in the pathogenesis of specific autoimmune diseases by exerting multiple immunomodulatory effects (15). The IFN signature, defined as the increased expression of type 1 IFN that regulates genes including IFNα-inducible genes (IFIGs), was originally characterized in patients with systemic lupus erythematosus and was found to be associated with increased disease severity (16). Furthermore, it has been identified in the peripheral blood of patients with other autoimmune diseases such as systemic sclerosis, rheumatoid arthritis, and primary pulmonary hypertension (17,18). Since the administration of steroids significantly reduces SIGLEC1 mRNA levels in peripheral blood monocytes (PBMC) (6), patients who underwent steroid therapy were excluded from this study.
Increasing evidence suggests that type 1 IFN may also be associated with the pathogenesis of GD. Kuang et al. reported that IFNα activity was present in the PBMC of most GD patients in the form of higher expression levels of IFIGs. They also demonstrated that the expression of IFIGs in GD patients was associated with elevated autoantibodies against the TSH receptor (19), which is consistent with the present results, namely, a positive correlation between SIGLEC1 mRNA and serum TRAb levels in continuous data (Table 3). The present study also showed that the expression of IFIGs, such as 2′,5′-oligoadenylate synthetase (OAS), interferon-induced protein 44 (IFI44), chemokine (C-X-C motif) ligand 10 (CXCL10), and Siglec1 (SIGLEC1), was upregulated in the R patient in a DNA microarray analysis (Table 1). This result suggests the presence of the IFN signature in the peripheral leukocytes of GD patients. The transcriptomic analysis of the thyroid glands of GD patients revealed that the IFN signature is present in those with a long clinical course, but not in those with a short clinical course, suggesting the potential of the IFN signature to assess the chronicity of the disease (20). Therefore, since SIGLEC1 mRNA levels are elevated in the peripheral leukocytes of R patients with GD relapse experience, SIGLEC1 mRNA levels may reflect chronic and intractable GD. On the other hand, since Siglec1 mRNA levels correlate with serum TRAb and thyroid hormone levels in continuous data (Table 3), SIGLEC1 mRNA levels may also reflect the current activity of GD.
Several genome-wide association studies have recently been performed on GD (21) and identified GD susceptibility genes such as human leukocyte antigen (HLA) class II, protein tyrosine phosphatase, non-receptor type 22 (PTPN22), and cytotoxic T-lymphocyte antigen 4 (CTLA-4). However, no genome-wide association studies have ever identified SIGLEC1, suggesting that SIGLEC1 is not applicable to predicting susceptibility to GD.
Ferreira et al. recently reported that SIGLEC1 expression by PBMC indicates the presence of the IFN signature, which precedes the clinical manifestation of autoimmunity in children genetically at risk of T1D (22). T1D is commonly associated with autoimmune thyroid diseases, such as GD, and is regarded as a variant of autoimmune polyglandular syndrome type 3 (23). Therefore, further studies are needed in order to clarify whether SIGLEC1 mRNA levels in peripheral blood cells are a biomarker for autoimmune polyglandular syndrome type 3.
Several studies attempted to identify potential predictors of remission or relapse after treatments with ATDs, either at the beginning or during therapy. Young age (<40 years); being male; smoking (particularly for men); and having large goiters (>80 g), Graves' ophthalmopathy, and/or high serum TRAb levels at the beginning and end of therapy were generally associated with higher relapse rates (24). Vos et al. also recently demonstrated that a lower age, higher serum free T4, higher serum thyrotropin-binding inhibitor immunoglobulin, and larger goiter sizes at diagnosis prior to ATD treatments were independent predictors of the recurrence of GD (25). We did not consider these factors, which may be a limitation of the present study. Using these parameters, Vos et al. constructed two simplified predictive models called the Graves' Recurrent Events After Therapy score, which provides a quick prediction of GD relapse (25). This score appears to be promising for assisting physicians with treatment decisions for their patients. However, in that study, the authors only employed a block and replacement regimen, consisting of 30 mg of MMI and levothyroxine at a dose to maintain normal serum fT4 levels, as ATD therapy and stopped this therapy one year later. Therefore, some patients with GD may not have been in remission at the end of therapy. On the other hand, in our prospective study, all patients with GD were treated based on the JTA guidelines by experts for thyroid disease and in remission at ATD discontinuation, which is a major difference from their study.
Since high serum TRAb levels are pathogenic factors for GD, they may have potential for predicting GD relapse. A meta-analysis of first-generation TRAb measurements, which was performed using radio- or enzyme-receptor assays, concluded that TRAb did not have the ability to predict relapse after ATD discontinuation with high accuracy (26). Second-generation TRAb measurements using anti-monoclonal TRAb and human recombinant TSH receptors improved sensitivity. However, based on several studies, overall predictivity for GD relapse after ATD discontinuation had a sensitivity of 67.0% and specificity of 65.0%, which are low predictive values (27 –31). Third-generation TRAb measurements using the human monoclonal thyroid-stimulating antibody M22 (M22-TRAb) (32) were employed in the present study. Hwang et al. estimated the optimal cutoff value for M22-TRAb by analyzing the ROC curve at the end of the ATD treatment. They reported that setting an M22-TRAb cutoff value of 2.23 IU/L resulted in sensitivity and specificity values of 56.3 and 76.7%, respectively (33), suggesting that M22-TRAb is still not sufficient for predicting GD relapse.
In the cross-sectional study, the optimal cutoff value of SIGLEC1 mRNA levels (258.9 copies) obtained by the ROC analysis showed marginal distinguishability for GD relapse experience (sensitivity, 66.7%; specificity, 70.1%), suggesting that the cutoff value has a limitation. By the nature of the current cross-sectional study, it is possible that we enrolled patients with high SIGLEC1 mRNA levels in the non-R group, who had not yet experienced relapse because they were still in the early stages after ATD discontinuation, and those with low SIGLEC1 mRNA levels in the R group, who relapsed long before the measurement of SIGLEC1 mRNA levels and were currently in long-term remission. In addition, some patients among those who were categorized into the R group by interview might have suffered from thyrotoxicosis due to silent thyroiditis, which is often seen in the course of GD, rather than a true GD relapse (34, 35). These may explain the limitations of the cutoff value and its sensitivity-specificity to distinguish GD relapse experience. Therefore, further prognostic studies may provide a more appropriate cutoff value of SIGLEC1 mRNA levels to predict GD relapse. Moreover, categorical data highlighted discordance in the distinguishability of GD relapse experience between serum TRAb and SIGLEC1 mRNA levels, suggesting the different nature of the two parameters. We assume that serum TRAb levels may reflect the current GD activity, whereas SIGLEC1 mRNA levels may reflect intractable GD.
In the prospective study, SIGLEC1 mRNA levels at ATD discontinuation were stronger predictors of GD relapse than serum TRAb levels, suggesting the high predictivity of SIGLEC1 mRNA levels for GD relapse. This discrepancy between the cross-sectional and the prospective studies further supports our hypothesis that serum TRAb levels may reflect current disease activity with a diagnostic value, whereas SIGLEC1 mRNA levels, in addition to the current disease activity, may also be used for the assessment of intractable GD.
As shown in Table 5, marginal fluctuations in SIGLEC1 mRNA levels were noted in some patients in the course of GD, which may partly support the hypothesis that SIGLEC1 mRNA levels reflect chronic and intractable GD.
Since the expression of some IFIGs such as OAS, IFI44, and CXCL10 was significantly increased in the R group in the DNA microarray analysis (Table 1), predictions employing a combination panel of the expression of these genes including SIGLEC1 mRNA levels in peripheral leukocytes warrant further study.
SIGLEC1 is a type 1 transmembrane protein with an extracellular region containing 17 immunoglobulin-like domains. It may function in its secreted and membrane-bound forms (36). However, the physiological significance of the secreted forms of SIGLEC1 remains currently unclear. Moreover, under certain conditions, such as inflammation, secreted soluble forms of SIGLEC1 may become anchored within the extracellular matrix and mediate adhesive cellular interactions (36). In the present study, serum SIGLEC1 levels were almost undetectable and similar between the R and non-R groups (Fig. 1D). Therefore, we assume that serum-soluble Siglec1 is difficult to detect and does not reflect GD activity. Therefore, in future studies, a fluorescence-activated cell sorting analysis needs to be performed in order to evaluate SIGLEC1 anchored on the cell membranes of monocytes in GD patients.
In conclusion, this study provides the first evidence for SIGLEC1 mRNA levels in peripheral leukocytes being significantly higher in GD patients with relapse experience than in those in long-term remission. Furthermore, we show that SIGLEC1 mRNA levels after ATD discontinuation may predict GD relapse. The results of this multicenter study suggest not only that SIGLEC1 has potential as a novel biomarker for GD, but also provides novel insights into SIGLEC1 as an IFN signature in the pathogenesis and development of GD.
Footnotes
Acknowledgments
This work was supported in part by the Research Program of Intractable Diseases provided by the Ministry of Health, Labour, and Welfare of Japan (K.H.), Grants-in-Aid for Scientific Research (KAKENHI) from the Japan Society for the Promotion of Science (JSPS); grant number JP 26461376 (K.H.), the Japan Thyroid Association (K.H.), Kurozumi Medical Foundation (K.H.), and Daiwa Securities Health Foundation (K.H.). The authors gratefully acknowledge financial support from Dr. Kazuya Miyashita (Miyashita Clinic, Takasaki, Gunma, Japan).
Author Disclosure Statement
No competing financial interests exist.