
Abstract
Background:
The hobnail variant of papillary thyroid carcinoma (HPTC) has an aggressive behavior. The aims of this prospective study were to define the clinical/molecular characteristics of HPTC, and to compare them to those of conventional papillary thyroid carcinoma (PTC).
Methods:
From 2010 to 2016, 25 cases of HPTC, characterized clinically and molecularly (BRAF, RAS, TERT promoter, and TP53 mutations), were compared to a series of 165 consecutive cases of PTC. All patients underwent total thyroidectomy and received radioactive iodine treatment. Follow-up was available for 19 HPTC patients.
Results:
Among the HPTC patients, 64% had a hobnail component ≥30%, and 64% had multifocal disease. The mean tumor size was 30 mm; 96% of tumors were angio-invasive; 68% were N1, and 12% were M1; 58% harbored the BRAFV600E mutation, 12% had a mutation in the TERT promoter, 17% had a TP53 mutation, and not had a RAS mutation. At a mean follow-up of 39 months, 32% of patients had biochemical and/or structural disease. Tumor size was the only significant difference between patients with persistent disease and those with an excellent response (40 mm and 24 mm, respectively; p = 0.02). Compared to the PTC control group, the HPTC patients had larger tumors (30 mm vs. 16 mm; p < 0.001), more frequent lymph node involvement (68% vs. 38%; p = 0.01), and remote disease (16% vs. 3%; p < 0.0001), a similar prevalence of the BRAFV600E mutation (58% vs. 59%), a higher prevalence of TP53 mutations (17% vs. 1%; p < 0.05), and a worse outcome (structural/biochemical disease: 32% vs. 9%; p < 0.0001).
Conclusions:
HPTC is an aggressive variant, characterized by large tumor size, lymph node involvement, a tendency to metastasize, and a worse outcome.
Introduction
D
In addition to traditional histopathological risk factors, particular molecular profiles (e.g., simultaneous BRAF and TERT mutations) appear to predict an additional risk of extrathyroid extension, lymph node involvement, and distant metastases (8 –10). While these observations need further validation, it seems likely that a given molecular profile is of prognostic significance, and could be considered in traditional stratification systems.
Hobnail PTC (HPTC) is a recently identified, rare histological variant with an aggressive behavior. It typically has a higher stage at presentation, a tendency for lymph node and distant metastases, and a significant mortality rate, with a disease-specific survival rate of 46–66% (6,11 –22). From a molecular standpoint, the most common mutational events identified in HPTC involve the BRAF (71%) and TP53 (56%) genes, but recent studies have also reported RET/PTC1 rearrangements and TERT promoter mutations (23 –25).
The aims of the present monocentric, prospective study were: (i) to clarify the clinical and molecular features of HPTC, and its outcomes, in a large series of patients followed up at the authors' institution; and (ii) to compare the characteristics of HPTC to those seen in a consecutive series of patients with conventional PTC histotypes.
Materials and Methods
Patients
From September 2010 to October 2016, 2620 cases of PTC were analyzed, and 25 cases with hobnail features were found. The histological diagnosis of HPTC was established according to the classification proposed by Asioli et al. (6,14) in 2010. Specifically, cases of nonsolid PTC with ≤10% tall/columnar/diffuse sclerosing components, loss of polarity/cohesiveness and prominent hobnail features in ≥10% of the tumor cells, and a detectable micropapillary architecture were classified as HPTC.
The HPTC cases were compared to a group comprising a consecutive series of 165 cases of PTC with conventional histotypes (131 classical, 13 follicular, and 21 oncocytic variants of PTC) (26). The patients' molecular status was established initially on fine-needle aspirates obtained from the thyroid nodule.
The patients' clinical data were obtained from the electronic medical records. The surgical pathology specimens were analyzed by two expert pathologists, and pathological staging was done according to the seventh edition of the TNM system (27). In the event of multiple foci, the largest tumor was considered.
This study was conducted according to the guidelines laid down in the Declaration of Helsinki. All patients participating in the study gave their written informed consent.
DNA extraction and mutation analysis
Genomic DNA was extracted from frozen tissues after surgery using the DNeasy Blood and Tissue kit (Qiagen, Milan, Italy), according to the manufacturer's protocol. Mutational analysis was performed for BRAF (NM_004333.4), N-RAS (NM_002524.3; exons 2 and 3), K-RAS (NM_033360.2; exons 2 and 3), H-RAS (NM_005343.2; exons 2 and 3), TERT proximal promoter (NM_198253.2), and TP53 (NM_000546.5 exons 5-8) by direct sequencing (ABI PRISM 3130; Applied Biosystems, Foster City, CA), as described elsewhere (28,29).
Treatment and outcome
All patients (in both the HPTC group and the PTC control group) underwent total thyroidectomy, and received radioactive iodine (RAI) ablation or treatment. When a second treatment was indicated, it involved surgery, RAI, or external beam radiation.
Based on recent American Thyroid Association (ATA) guidelines (30), four possible outcomes were identified: excellent, biochemically incomplete, structurally incomplete, and indeterminate response. Only cases with a follow-up of at least 12 months were considered in terms of final outcome.
Statistical analysis
Categorical data were summarized using frequencies and percentages. Distributions of the continuous variables were assessed, and data were summarized accordingly. The comparison between continuous variables (age at diagnosis, tumor size, and follow-up) in the two histological groups was done with the t-test on independent samples and the Mann–Whitney test. Group comparisons of categorical variables were run using the chi-square test. A p-value of <0.05 was considered statistically significant.
Results
Histological and molecular features, and final outcome in HPTC patients
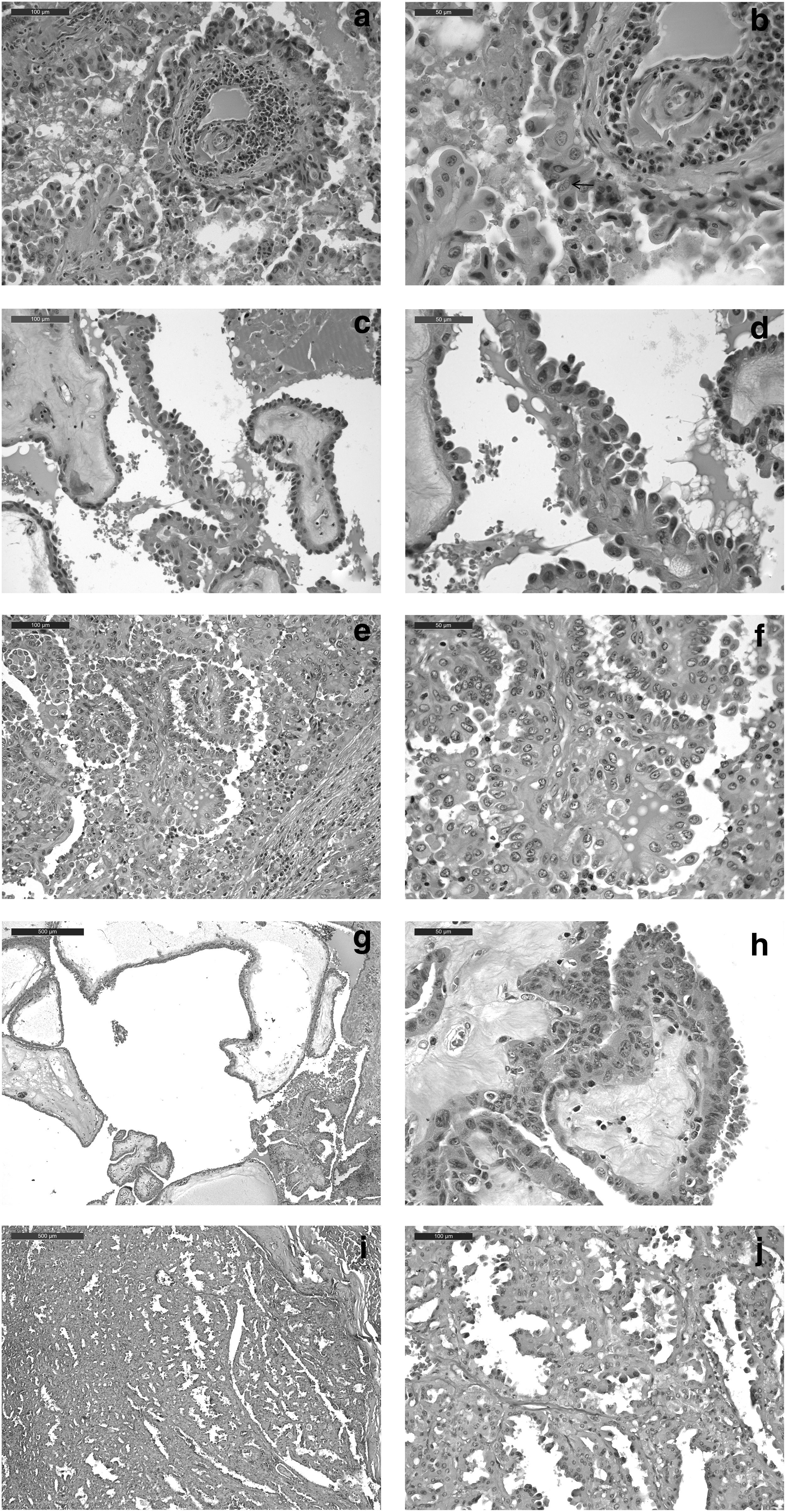
The characteristics of the HPTC cases are summarized in Table 1 and shown in Figure 1.
(
wt, wild type; ER, excellent response; P/S, persistence/structural disease; P/B, persistence/biochemical disease; n.a., not available.
Of the 25 cases, 15 (60%) were female and 10 (40%) were male. The mean age of the sample at diagnosis was 48 years (min 24, max 73; standard deviation [SD] ±14). The cytological analysis of fine-needle aspiration biopsy samples pointed to PTC (Bethesda 4–5) in 21/24 (87%) cases, while three were Bethesda 3, and no cytological analysis was available for one patient.
On histology, of the 25 HPTC cases, 16 (64%) had a hobnail component ≥30%, and in 9 (36%) it ranged between 10% and 29%.
Of the 25 cases, five (20%) were staged as T1, three (12%) were T2, 15 (60%) were T3, and two (8%) were T4. Sixteen (64%) of the 25 patients had multifocal tumors. The mean tumor size was 30 mm (min 7, max 80; SD ±18), and women had smaller tumors than men (24 mm vs. 38 mm; p = 0.06). In 24 (96%) of the 25 cases, the tumor was angio-invasive, 11/25 (44%) revealed perineural invasion, and 24/25 (96%) showed areas of intraneoplastic sclerosis.
Lymph node involvement was detectable at the time of initial diagnosis in 17/25 (68%) cases, and a lateral neck compartment was involved (N1b) in 7 (41.17%) of these cases. At the time of their diagnosis, 3/25 (12%) patients had distant metastases: two to the lung, and one to bone. Two of these three patients were >45 years old, and one was younger.
According to the seventh TNM classification, 12/25 (48%) patients were in stage I, 1/25 (4%) was in stage II, 8/25 (32%) were in stage III, and 4/25 (17%) were in stage IV.
The mutational status of the tumors was as follows: 14/24 (58%) harbored the BRAFV600E mutation; 3/24 (12%) had a mutation in the TERT promoter, with two harboring a C228T mutation, and one a point mutation −74C>T (C178T) plus a deletion −71delG (175delG; this last patient was stage III at diagnosis, but had an excellent response after 24 months of follow-up, and it remains unclear whether this mutation affects TERT promoter function; Fig. 2); and 4/24 (17%) had TP53 mutations. No H-K-N-RAS gene mutations came to light. Cancer tissue was unavailable for one patient.
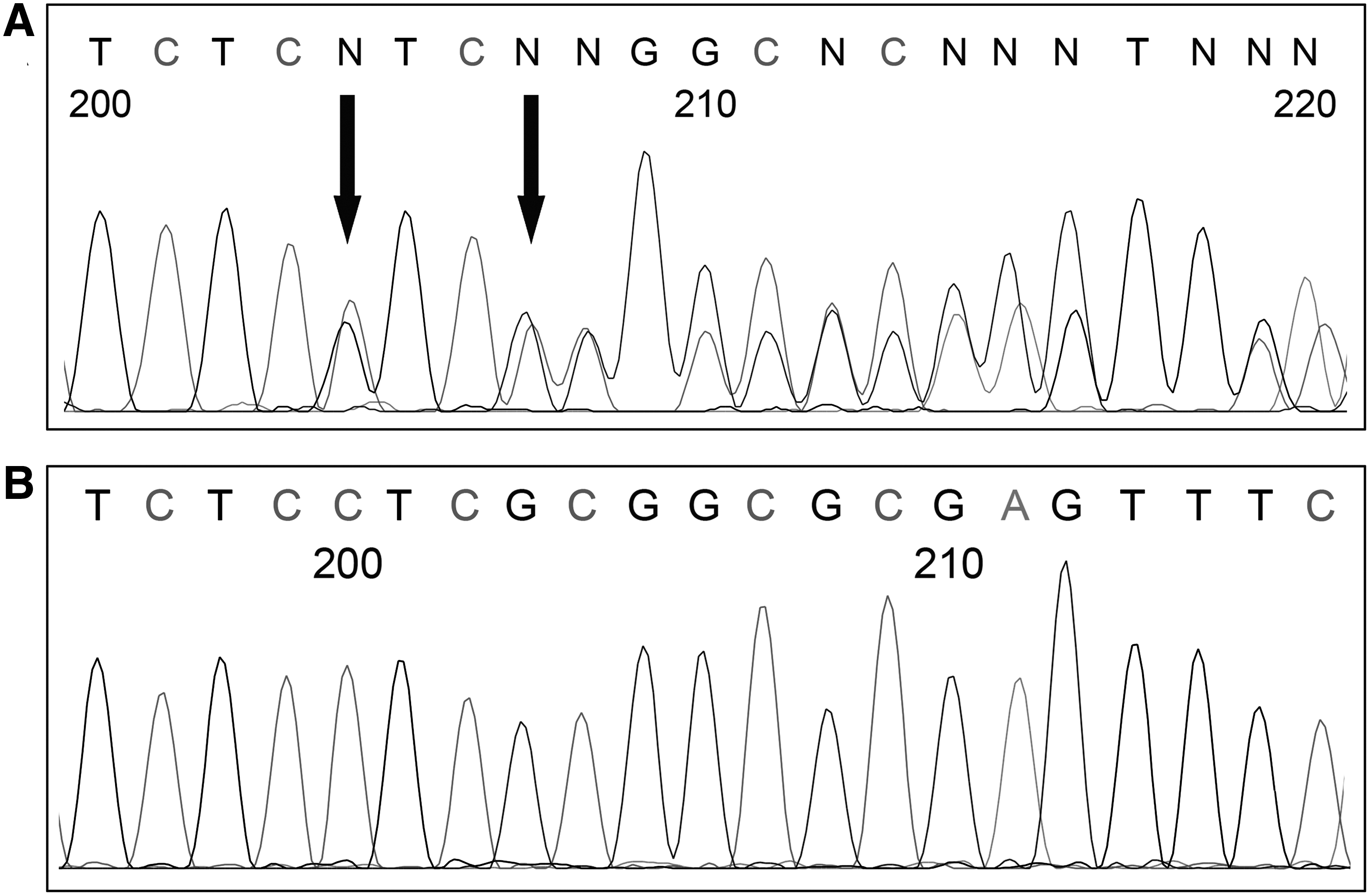
Representative electropherograms of TERT promoter. (
Based on the criteria outlined in “Treatment and outcome” above, the disease status was analyzed in 19 patients, with a mean follow-up of 39 months (min 13, max 67; SD ±16). Of these 19 patients, 13 (68%) had an excellent response, one (5%) had a biochemically incomplete response, and five (26%) had a structurally incomplete response (i.e., locally persistent disease in one, and distant metastases in four: to the lung and liver in one, to the lung alone in two, and to the bone in one). Patients with locally persistent disease had larger tumors at diagnosis than patients in remission (M = 40 mm, range 7–80 mm, SD ±28 in the former; mean 24 mm, range 11–50 mm, SD ±13 in the latter; p = 0.02). No statistically significant differences emerged in terms of the following: lymph node involvement (83% in cases of structurally/biochemically incomplete response vs. 54% in disease-free subjects), cancer multifocality (67% vs. 46%), or age at time of diagnosis (48 years vs. 46 years). There were also no significant differences between the patients with a hobnail component <30% and those with a component ≥30% (Table 2).
F/M, female/male; DS, deviation standard.
Among the HPTC patients with a structurally/biochemically incomplete response to treatment, the mutational status was known in five cases: three (60%) were BRAF wild type, two (40%) were BRAF mutated; and one (20%) showed the classic TERT promoter mutation.
In case 15, a novel TERT mutation never previously described in the literature was detected (Fig. 2). This mutation was localized within the promoter and consisted of a point mutation (178C>T) followed by a deletion of a single nucleotide (175delG). The novel mutation was confirmed by resequencing a second DNA sample from the same patient, a female with chronic lymphocytic thyroiditis, who was 60 years old when her HPTC was diagnosed. She had a large (50 mm) tumor with a 30% hobnail component that, despite its size, did not invade the extrathyroidal tissues (Fig. 1A and B). At 23 months of follow-up, her response to treatment was excellent.
Case 20 revealed a concomitant BRAFV600E and C228T TERT promoter mutation. This male patient was 72 years old at the time of his HPTC diagnosis. He had bilateral, multifocal disease, the largest tumor 41 mm in size. The hobnail component was 10%, and the tumor was very aggressive, angio-invasive, with extrathyroid tissue involvement and intratumoral necrosis. The patient also had positive laterocervical lymph nodes. At the time of the study, his follow-up was <12 months.
Cases 9, 16, 24, and 25 revealed simultaneous BRAFV600E and TP53 mutations. These patients were females, ranging in age from 30 to 69 years and with a tumor size ranging from 11 mm to 41 mm at the time of diagnosis. The hobnail component was ≥30% in two of these cases. Follow-up data were available for two subjects, and they had both an excellent response to treatment.
Comparison between HPTC and conventional PTC
The clinical and molecular characteristics of the cases in the HPTC and the PTC control groups are summarized in Table 3. The patients' mean age at diagnosis was similar in the two groups (both 48 years). Mean tumor size was significantly larger in the HPTC group than in the PTC control group (30 mm, range 7–80 mm, SD ±18 vs. 16 mm, range 2–60 mm, SD ±10, respectively; p < 0.001). The two groups did not differ significantly in terms of multifocality (64% in HPTC cases vs. 53% in controls), but lymph node involvement at diagnosis was more common in the HPTC group (68% vs. 38%; p = 0.01). Among the HPTC patients with positive lymph nodes, 10/25 (40%) were N1a and 7/25 (28%) were N1b, as opposed to 38/165 (23%) and 35/165 (15%), respectively, among the PTC controls. Distant metastases were also more common in the HPTC group (16% vs. 3%; p < 0.0001). No differences emerged between the two groups in terms of mutational status, except for a higher prevalence of TP53 mutations among HPTC cases (17% vs. 1%; p < 0.05).
PTC, papillary thyroid carcinoma.
Patient outcome differed significantly, however. The response to treatment was excellent in 13/19 (68%) HPTC patients after a mean follow-up of 39 months, and in 146/165 (88%) PTC cases after a mean follow-up of 72 months. A structurally or biochemically incomplete response was seen in 6/19 (32%) HPTC patients and 15/165 (9%) controls (p < 0.0001).
Discussion
PTC is the most common endocrine malignancy and generally has an excellent prognosis. Some histological variants are known to be associated with a poorer outcome, however, and the recently identified hobnail histotype has been classified among the more aggressive forms of PTC. From a clinical standpoint, most studies conducted to date have describe HPTC as a thyroid cancer presenting as larger masses, rarely multifocal, and frequently with lymph node involvement and distant metastases. The most common mutations associated with this variant involve BRAFV600E and TP53 (6,14,23).
For this prospective monocentric study, 25 cases of HPTC diagnosed from September 2010 to October 2016 were recovered, indicating a prevalence of around 0.9%, in line with previous studies (23), and confirming the rarity of this histological form (though a Sicilian study reported an incidence rate of 2.7%) (22).
The histological and molecular characteristics of the sample and the patients' outcomes were analyzed. The data confirmed that the hobnail variant is associated with several known negative prognostic factors in PTC: larger tumor size at diagnosis, vascular invasion and intraneoplastic sclerosis, and a marked propensity to metastasize. In line with the most recent studies conducted on HPTC (24,31), the male-to-female ratio in the present series tipped less toward the female side (1:1.5), indicating that this variant probably affects men more frequently than other PTC histotypes (though this proportion differs from the one reported in some of the earliest studies on HPTC and from the Sicilian case) (6,14,22). On the other hand, the findings differ from other published data in that multifocality was more common than previously reported (24), while older age at diagnosis did not seem to relate to the HPTC variant.
Regarding patient outcomes, HPTC was found to behave quite aggressively in the present series. At a mean follow-up of 39 months, nearly one in three (31%) patients had a biochemically/structurally incomplete response, sometimes in combination with distant metastases. These findings are comparable with other reports. A recent review of 55 cases of HPTC collected from nine different studies found persistent disease in 17% and a disease-related death rate of 19% after a follow-up of 4–274 months (24). Another recent multicentric analysis conducted by Asioli et al. (23) on 18 HPTC showed persistent disease in 39% of cases at a mean follow-up of 49 months, and a disease-related death rate of 22% after a mean of 22 months. The present study only has a follow-up of 39 months, with no disease-related deaths so far. However, four of the patients with distant metastases are currently followed, and three of them have systemic involvement and are expected to fare poorly over the coming months. Like Asioli et al. (14), it was found that the amount of hobnail component had no influence on patient outcome.
The results of the mutational analysis differ from those of previous reports. In the present sample, the prevalence of the BRAFV600E mutation was 58%—lower than in other studies in which it was at least 71% (23,24). The current sample also revealed no association between BRAF mutations and outcome, in contrast with the recent review by Asioli et al. (23), according to which BRAFV600E mutations, alone or combined with TP53 mutations, were associated with a higher mortality risk. The current study also found a 12% prevalence of TERT promoter mutations, which is lower than previously reported (23). Moreover, a 17% prevalence of TP53 mutations was found. This percentage is lower than recent findings reported by others (56%) (23). This difference is perhaps due to the different method of analysis employed and, more likely, due to the fact that the current series is both consecutive and monocentric, which differs from previous reports. As in previous series, the number of HPTC cases was limited, and further studies are needed to clarify broadly the molecular status underlying this new histological entity.
More importantly, the present monocentric study compared 25 HPTC cases with 165 consecutive cases of PTC with conventional histological patterns (all cases diagnosed, treated and followed according to the same standard of care at the same institution). The comparison was based on histology, molecular findings, and patient outcome. By comparison with the PTC control group, the hobnail variant appears to have a less marked predilection for the female sex, a larger tumor size (p < 0.001), and a higher frequency of lymph node involvement (p = 0.01), and distant metastases (p < 0.0001), already at diagnosis. As expected, patient outcome clearly differed between the two groups. In the HPTC group, a local and/or distant, structurally or biochemically incomplete response was apparent in nearly one in three cases, whereas only 9% of the PTC controls were not cured (p < 0.0001).
Regarding case 20, this patient had many different disease-related risk factors for structural disease recurrence (30,32) or death, in addition to having HPTC associated with the simultaneous presence of two mutations. This 72-year-old male had a large, angio-invasive mass (41 mm) with intratumoral necrosis, a significant lymph node involvement in the lateral neck compartment (11/34 lymph nodes removed were positive), and a follow-up of only eight months. It could be of interest to examine the impact of his mutational status over time, but for the time being, his follow-up is too short to enable any conclusions to be drawn.
In the last decade, more attention has been paid to the different histologic forms of PTC, and more than 10 variants have been documented (33), some of them associated with a more aggressive behavior. HPTC is probably the most recent addition to the list of aggressive variants, and the latest ATA guidelines (30) have accordingly included the hobnail variant among the thyroid cancers with an unfavorable outcome, such as tall-cell and columnar-cell PTC. The data presented here concern a mono-institutional experience of 25 cases of HPTC that, to the authors' knowledge, is the largest monocentric series described to date. Confirming previous findings, this study found this histotype associated with an aggressive behavior, and known risk factors for a different course from the normally indolent PTC. In fact, the very different outcome of patients with HPTC was already clearly evident, with a follow-up of just 39 months. Further studies are needed to define this more recently defined variant better from a molecular, histological and clinical standpoint.
As we are now moving toward novel approaches to thyroid cancer management in an effort to limit its increased detection and over-treatment, it is even more crucial to recognize the rare forms of PTC that take a different clinical course, and consequently require tailored management and personalized follow-up protocols. The rare hobnail variant probably demands a more intensive initial treatment and follow-up than classical PTC variants to deal with its aggressive clinical and pathological features, and improve the otherwise poor prognosis for patients with this histological variant.
In conclusion, the aggressiveness of HPTC and the related worse outcome for patients are confirmed. Further investigations may clarify the relationship between this variant of PTC with known risk factors, hopefully leading to a more thorough understanding of their particular molecular drivers.
Footnotes
Acknowledgments
This research was conducted using the resources of the Tissue Bank at the 1st Surgical Clinic, Padova University Hospital. We thank Mrs Frances Coburn and Christina Drace for text editing.
Author Disclosure Statement
The authors have nothing to disclose.