
Abstract
Background:
National data on iodine status in Israel are lacking. Reliance on iodine-depleted desalinated water, the absence of a salt iodization program, and reports of increased use of thyroid medication in Israel suggest that the population's iodine intake is likely inadequate. The aims of this study were therefore to determine the iodine status of Israeli school-age children (SAC) and pregnant women (PW) in a nationally representative sample obtained by a novel approach of using pre-discard urinalysis samples collected from a centralized national laboratory.
Methods:
Spot urine samples from 1023 SAC and 1074 PW, representing all regions and major sectors in Israel, were collected during 2016 at the Maccabi Healthcare Services central laboratory. Urinary iodine concentration (UIC) was measured, and the results were analyzed by trimester, sex, region, and sector.
Results:
SAC were iodine deficient, with a median (interquartile range [IQR]) UIC of 83 μg/L (52–127 μg/L); 62% of SAC UICs were below the World Health Organization adequacy range for SAC (100–199 μg/L). PW were also iodine deficient, with a median (IQR) UIC of 61 μg/L (36–97 μg/L); 85% of PW UICs were below the adequacy range for PW (150–249 μg/L). For both SAC and PW, the median UIC was below the World Health Organization's adequacy range across all sectors, sexes, and districts. Among SAC, the median (IQR) UIC was lower among females (75 μg/L; 48–119 μg/L) than males (92 μg/L; 59–133 μg/L; p < 0.05). Median UIC values of PW correlated significantly with the median UIC for SAC by sub-district (R 2 = 0.3, p < 0.05).
Conclusions:
Urine sampling via a centralized national laboratory was efficient and cost-saving. Iodine deficiency in Israeli SAC and PW is a serious public-health concern. A national program of salt iodization and iodine supplementation of PW should be urgently considered.
Introduction
A
The World Health Organization (WHO) recommends universal salt iodization (USI), that is, the iodization of all salt for human and animal consumption, and this is the preferred strategy for controlling IDD (7). Mild-to-moderate ID now affects large populations in Europe and around the world and has reemerged as a major public-health concern in many industrialized countries, even those with USI programs, underscoring the importance of routine monitoring of population iodine status (8,9).
Israel is among the few countries where a national iodine survey has not been performed (10) and where there is no national program of iodine prophylaxis (e.g., USI) (11). Although a handful of studies documented the occurrence of endemic goiter in the north of Israel in the 1960s–1980s (12 –14), the prevailing view is that IDD is not a problem in Israel due to its proximity to the Mediterranean (15 –17). Perhaps for this reason, the issue has not been addressed until recently, and along with the absence of data regarding the iodine status, Israel similarly lacks current data on the incidence and prevalence of thyroid disease. While the extent of ID in Israel is unknown, self-reported use of thyroid medication among Israeli adults appears to be rising (18). This trend may be driven by Israel's increasing reliance on desalinated seawater, now accounting for approximately 80% of Israel's drinking water (19). It has previously been shown that this water is iodine poor (18,20).
The WHO recommends using the median of spot urinary iodine concentrations (UIC) among pregnant women (PW) in all stages of pregnancy and school-aged children (SAC) aged 6–12 years in a nationally representative sample to define the national iodine status (21,22). Moreover, focusing on these population groups is important, as they are vulnerable to the adverse effects of ID. Thus, the aims of this study were to obtain the first nationally representative data on iodine status in PW and SAC in Israel. To reach this goal quickly and efficiently, a novel approach was taken to obtain a nationally representative sample of urine samples using the available infrastructure of the Maccabi Healthcare Services (MHS), whose central laboratory processes all of the specimens provided for urinalysis by MHS members across the entire country on a daily basis.
Materials and Methods
Ethics
Ethical approval for this study was obtained from the MHS and the Israeli Ministry of Health supreme ethical committees. The ethics approval allowed for the collection and determination of iodine in anonymized urine samples that had been sent for clinical testing after the clinical test had been performed and before the samples were discarded.
Specimen collection
All urine specimens were collected at the MHS central laboratory (MHSCL). The MHSCL is a fully automated clinical laboratory that conducts routine urinalysis for every MHS clinic in the country on a daily basis. Because MHS insures more than two million people (∼25% of Israel's population), it was possible to obtain a large number of specimens efficiently and rapidly at a relatively low cost. For this study, pre-discard urine for SAC and PW was collected from March to September 2016. Women in Israel typically submit urine for a general urinalysis twice during pregnancy, and children submit urine for clinical indications. Due to ethical restrictions, it was not possible to access the clinical indication or test result for use as a criterion for specimen selection.
Representative sample generation
The sampling frame used by the Israeli Center for Disease Control for national surveys was employed to obtain a nationally representative sample of urine specimens. The primary sampling unit (PSU) was the community in which the MHS clinics and laboratories that provided the specimens were located. For each community, the overall population size, ethnic composition (percentage of secular and non-ultra-orthodox Jewish, ultra-orthodox Jewish [haredi], and Arab), and the proportion of the overall population served by each of 229 collection sites (PSU) were known. The number of urine samples required per PSU was calculated using census data from the Central Bureau of Statistics to account for the fraction of the general population in each PSU. Geographically adjacent PSUs were combined into clusters of known demographic characteristics, stratified by district (Fig. 1), sub-district, and community. This sampling scheme allows for stratification by geographic location and by Arab population (with 40 predominantly Arab PSUs distributed across every district of Israel), with 19 PSUs serving predominantly ultra-orthodox Jews.
Map of official districts in Israel as defined by the Israel Central Bureau of Statistics (
Procedures and assay
Before beginning the survey, it was ascertained that urinary iodine was stable under the survey conditions, and that the clinical and research procedures used did not compromise the iodine assay. Urinalysis at the MHSCL is fully automated. Urine is drawn directly from collection cups into vacutainer tubes with stabilizers (chlorhexadine, ethyl paraben, and sodium propionate) from which assays are performed by a robotic auto-sampler without dipstick testing that could otherwise contaminate the iodine assay. After clinical testing and before the specimens were discarded, specimens were set aside for weekly selection. A laboratory technician screened the specimen list and selected the survey samples until the number of samples required for each PSU was met. Specimens selected for inclusion in the survey were anonymized and given a unique study code. Only PSU location, urine collection date, sex, age, and pregnancy week were retained. The selected samples were then stored at −20°C until the entire population sample was complete. The remaining specimens were destroyed, and all identifying data were irreversibly deleted.
UIC determination was performed in the Human Nutrition Laboratory of the Swiss Federal Institute of Technology (ETH), Zurich, Switzerland, using a modified Sandell–Kolthoff reaction with spectrophotometric detection after ammonium persulfate digestion (23). The laboratory participates successfully in the Ensuring the Quality of Urinary Iodine Procedures (EQUIP) external quality control program of the U.S. Centers for Disease Control and Prevention.
Statistical analysis
Descriptive statistics and analyses were performed with JMP Pro v13 (SAS Institute, Cary, NC). The distribution of UIC in the overall population and subgroups was tested by Shapiro–Wilk W (normal distribution) and Cramer–von Mises W tests (Weibull distribution). Equality of variance across population subgroups was evaluated by both Levene and Bartlett tests. A nonparametric Kruskal–Wallis (rank sums) test followed by Wilcoxon tests were used to compare differences between each pair of subgroups as appropriate. A general linear model was used to determine whether UIC differed by trimester, ethnicity (by sector), and geographical location (by district) among PW. A two-tailed p-value of <0.05 was considered statistically significant.
Results
Iodine status in SAC
Valid results were obtained for 1023/1028 SAC urinary samples collected in 122 different communities across all districts and sub-districts of Israel. The female-to-male ratio was 57:43, and the ages did not differ by subgroup (Table 1). The overall median (interquartile range [IQR]) UIC in this population was 83 μg/L (52–127 μg/L; Fig. 2), which is below the WHO's adequacy range (100–199 μg/L) for SAC (21). The proportion of SAC for whom the UIC result was below this range was 62% (Table 1). The iodine status (median UIC, IQR) was significantly lower among females (75 μg/L, 48–119 μg/L; n = 581) than it was among males (92 μg/L, 59–133 μg/L; n = 442; p < 0.05). Significantly more females had low UIC than did males (67% vs. 55%; p < 0.05). Median UIC and proportion of results below the adequacy range did not differ significantly between sub-districts, districts, or sector (Table 1).
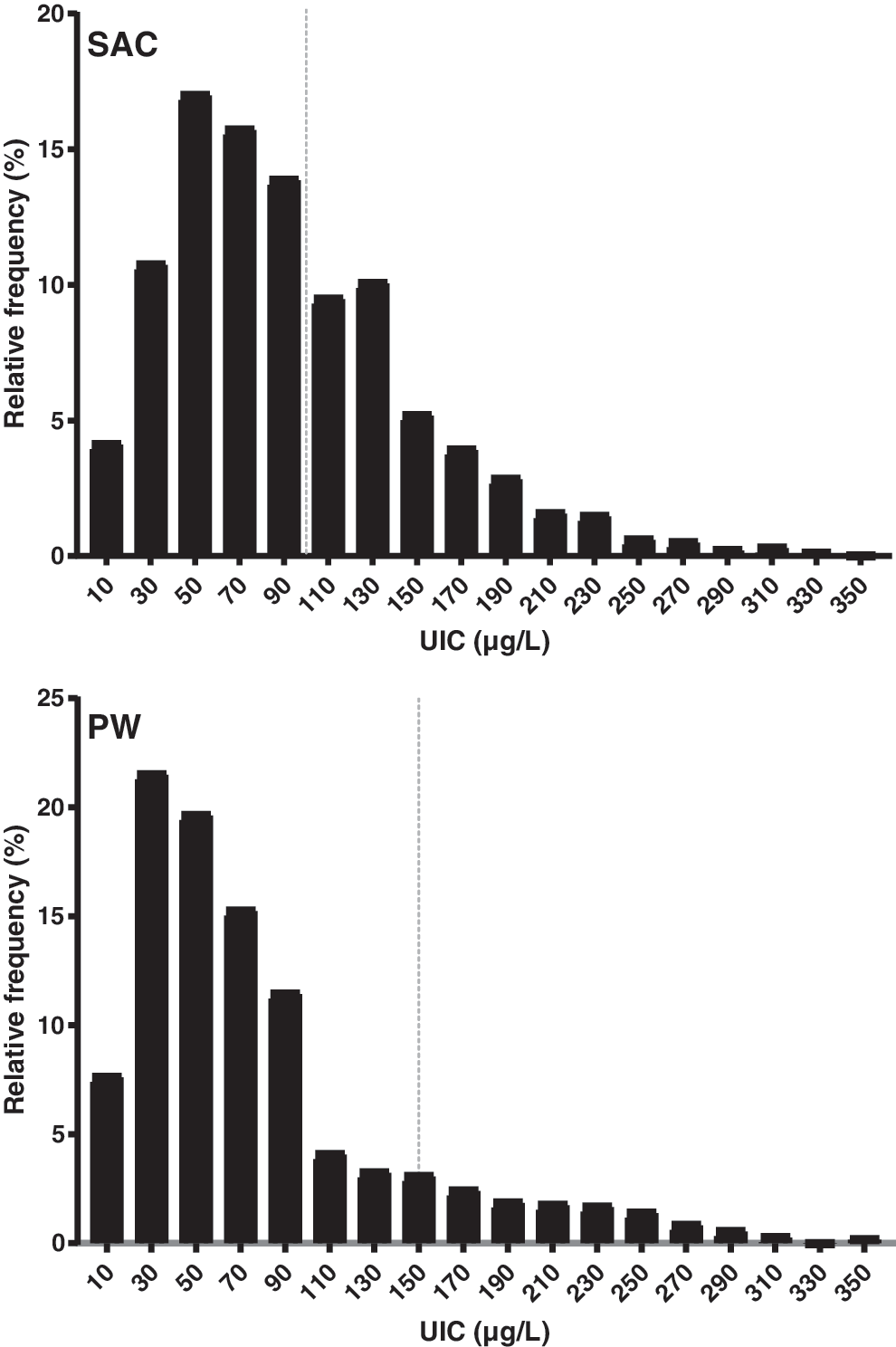
Histograms showing distribution of UIC for nationally representative samples of Israeli SAC (n = 1023) and PW (n = 1074). Gray vertical line shows threshold for median UIC defining adequacy in SAC and sufficiency in PW. PW, pregnant women; SAC, school-aged children; UIC, urinary iodine concentration; IQR, interquartile range.
Iodine sufficiency/adequacy threshold: UIC >150 μg/L for PW and UIC >100 μg/L for SAC (21).
Age-specific proportion of general Israeli population, aged 5–14 years for SAC and 20–54 years for PW, based on Central Bureau of Statistics census data for the year 2015.
Medians by sex without a common letter are significantly different (p < 0.05).
Medians by trimester without a common letter are significantly different (p < 0.05).
Medians by district without a common letter are significantly different (p < 0.05).
UIC, urinary iodine concentrations; PW, pregnant women; SAC, school-aged children; IQR, interquartile range; ND, no data.
Iodine status in PW
Valid UIC results were obtained for 1074 samples from the 1080 urinary samples of PW that were collected from 114 communities across all districts and sub-districts of Israel. The median (IQR) UIC in this population was 61 μg/L (36–97 μg/L; Fig. 2), which is below the WHO's adequacy range (150–249 μg/L) for PW (21). The proportion of PW for whom the UIC result was below this range was 85% (Table 1). Pregnant women in Israel's Central District (which does not include the Tel Aviv district; Fig. 1) had statistically higher though still insufficient UIC (median 75 μg/L; n = 256) than those residing in all other districts (p < 0.05). This difference remained significant after adjusting for district, trimester, and sector (p < 0.05). Median UIC from PW during the first trimester was statistically lower than that measured during the second though not the third trimester (59 μg/L, n = 337 vs. 63 μg/L, n = 457, and 61 μg/L, n = 280, respectively; p < 0.05; Table 1). Median UIC did not differ significantly across all three main sectors of Israeli society or across all 16 Israeli sub-districts.
Regional UIC variability
Figure 2 shows the median UIC distribution for both SAC and PW. The median UIC of SAC and PW did not achieve adequacy in any district (Table 1 and Fig. 3). Nevertheless, the median UIC values of PW correlated significantly with the median UIC for SAC by sub-district (R 2 = 0.3; p < 0.05), indicating subtle regional differences in intake (Fig. 4).
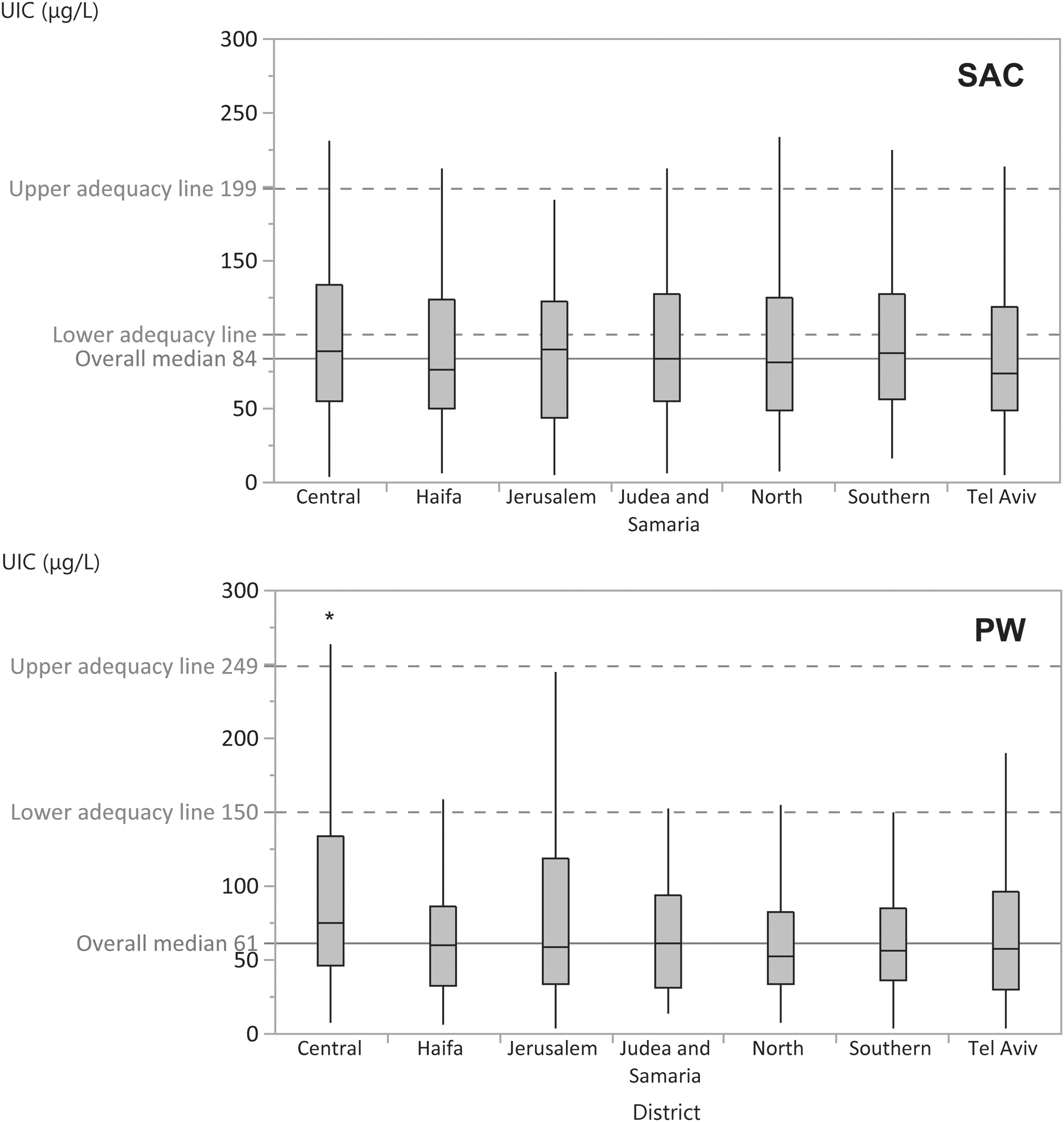
Box and whisker plots of median and IQR UIC for both Israeli SAC (n = 1023) and PW (n = 1074) by district. Whisker minimum and maximum values are 25th and 75th percentiles ±1.5*IQR. Outliers are not shown. Significantly higher than in all other districts (p < 0.05). Upper and lower adequacy lines are according World Health Organization (21).
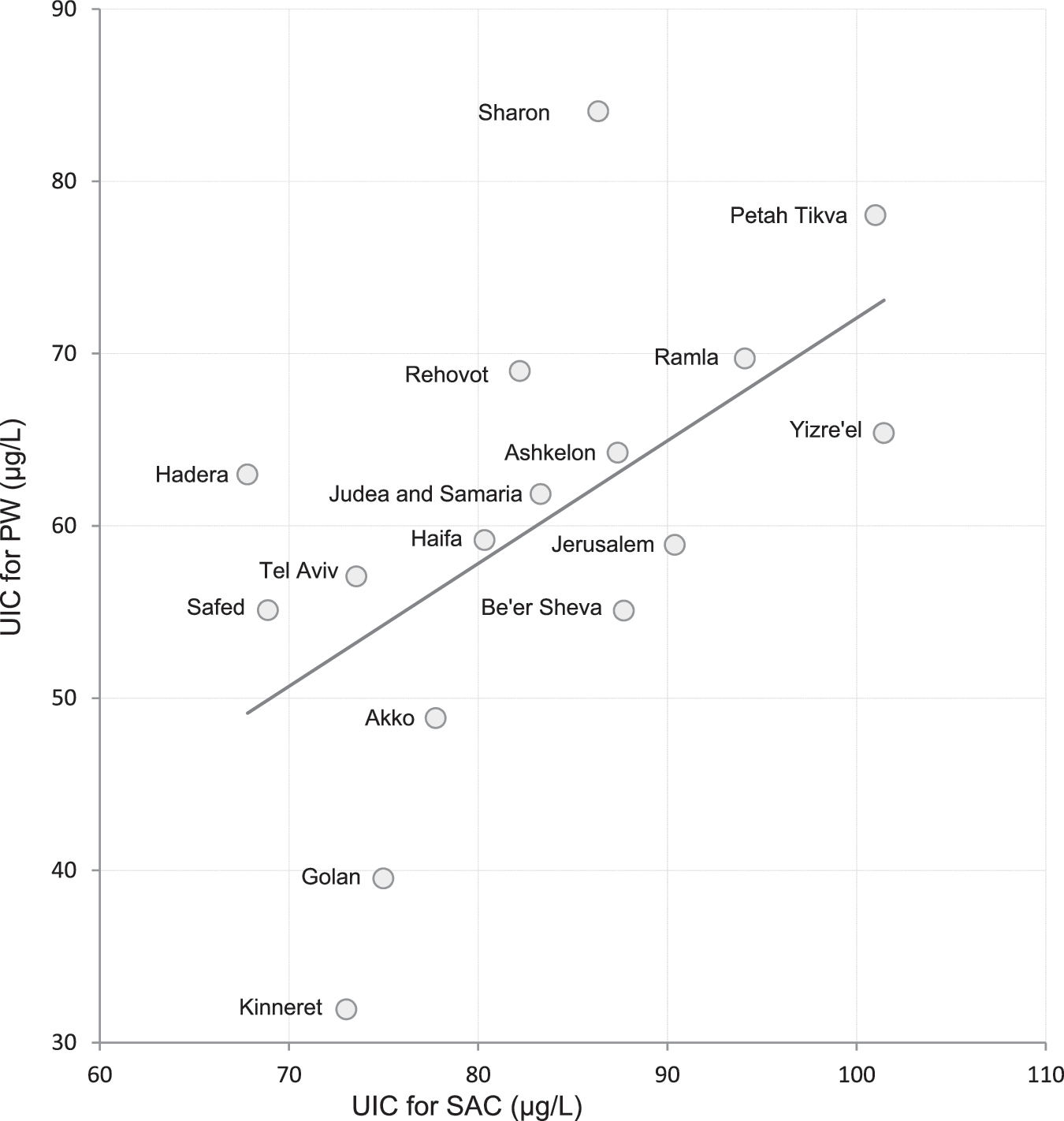
Scatter plot of median UIC values of PW (y-axis) plotted against median UIC of SAC (x-axis) for all 16 Israeli sub-districts. The regression line equation is y = 0.80 + 0.71(x), and R 2 = 0.324, p < 0.05.
Discussion
This is the first national iodine status survey conducted in Israel. It reveals a high prevalence of ID in the general population, as indicated by the low median UIC among SAC (21). The extent of deficiency in two key groups of Israel's population (PW and SAC) and among all sectors of its society across all of its regions is a cause for serious concern: At 61 μg/L, Israel's PW median UIC is one of the five lowest medians among 68 countries with updated national or subnational iodine status results in PW (24). For SAC, the median UIC of 83 μg/L was among the 10 lowest medians from 130 countries (24). The current survey also indicates that the ID pockets reported in the 1960s (12,13) and the 1980s (14), but which have not been studied since, are not an isolated public-health concern. On the contrary, in the absence of a national USI program and the negligible availability of voluntary iodized salt (11), as well as the heavy national reliance on iodine-depleted desalinated seawater as drinking and irrigating water (19,20), this study's results point to a major national public-health concern. Now that this survey has provided clear evidence that the Israeli population is iodine deficient, the prevalence of IDD in Israel should be determined.
While the median UIC among SAC defines the Israeli general population as “mildly deficient,” the proportion of children with spot UIC values below the adequate range is concerning. The observed distribution of spot UIC values reflects both intra- and inter-individual variance and therefore cannot be used to determine accurately the proportion of individuals in the distinct categories of severe, moderately, and mildly deficient. Nevertheless, the observed distribution suggests that iodine intake among a substantial proportion of Israeli children is well below the desirable range, including moderate to severe deficiency (Fig. 2). Severe ID among SAC causes impaired mental function and delayed physical development (1), but even mild ID can prevent children from attaining their full intellectual potential (25). Mild-to-moderate ID has been linked to decreased cognitive performance in children born to mothers with low iodine intake (26). Moreover, in children with inadequate intake, iodine supplementation may reverse some cognitive deficits. A randomized, placebo-controlled, double-blind trial in mildly iodine-deficient children in New Zealand (median UIC = 63 μg/L; n = 184; aged 10–13 years) showed that supplementation with150 μg/day for 28 weeks improved perceptual reasoning (25). A similar effect was achieved in children living in Albania who were moderately iodine deficient (median UIC = 43 μg/L; n = 310; ages 10–12 years) and received 400 mg of iodine as oral iodized oil for 23–24 weeks (3). ID is a key global risk factor for impaired child development (27), which is why the WHO recommends routine monitoring of population urinary iodine every three to five years (22,28), along with USI, as a means of sustainably controlling ID.
Similarly, the finding of insufficient iodine intake (UIC >150 μg/L) among 85% of PW also has serious implications. By comparison to data from other countries with a similar extent of deficiency, the present data suggest that in Israel, there is a high risk of both maternal and fetal hypothyroidism, as well as impaired neurological development of the fetus (4). A recent prospective study in the United Kingdom found that children born to women who were classified during pregnancy as only mild to moderately iodine deficient (UIC <91 μg/L) (2) were ∼60% more likely to have decreased scores for verbal IQ, reading comprehension, and reading accuracy at nine years of age than those whose mothers had above-median UIC during pregnancy, even after exhaustive adjustment for socioeconomic and other potential confounders. By extrapolation, given the rate of insufficiency in Israeli pregnant women, nearly all PW and their children might be at risk, implying that the majority of the population is unlikely to realize its full intellectual potential. As in the United Kingdom, in Israel, there is little dietary guidance on iodine, and the government has not acted yet on its own recommendations for USI (2,11) so that iodine intake is left entirely to chance through individual food choices and environmental factors. This is despite WHO recommendations for iodine supplementation in pregnancy and infancy in countries or regions where <90% of households are using iodized salt and the median UIC in SAC is <100 μg/L.
The iodine status within a national sample of Israeli PW (median UIC = 61 μg/L, n = 1074; 85% <150 μg/L) is low compared to PW residing in other regions without iodine prophylaxis. For example, PW from rural areas in Vietnam, which reports partial iodized salt use (29), had higher levels (median UIC = 70 μg/L; n = 413; 83% <150 μg/L). In Vienna, where USI was implemented in the past but only 25% of PW were estimated to consume iodized salt, levels were higher as well (median UIC = 87 μg/L; n = 246; 81% <150 μg/L) (30). Higher levels (median UIC = 89 μg/L; n = 2104; 80% <150 μg/L) were also found in the north of Spain (31), where the use of iodized salt is voluntary (32). In Israel, the availability of iodized salt is extremely low (3% of locally produced table salt) (11), and 80% of drinking water comes from iodine-depleted desalinated seawater (33). Furthermore, only 6% of Israeli PW report using iodine-containing prenatal supplements (Ovadia YS, Gefel D, Mabjeesh SJ, Dahl L, Goldsmith R, Troen AM. Low iodine intake from dairy foods in the Israeli population despite high milk iodine content. Eur J Nutr 2017; submitted). Although definitive evidence from randomized clinical trials showing benefits of iodine supplementation among PW in areas with mild ID has yet to be obtained (34), local guidelines for iodine-containing supplement use must be considered.
It is noteworthy that the present findings contradict the decades-old assumption that Israel is an iodine-sufficient country due to its proximity to the Mediterranean (15,16). This assumption was based on a commonly held notion that populations residing near the sea enjoy adequate iodine nutrition compared to those in inland areas due to the consumption of marine food and geophysical considerations (35 –37). This is clearly not true of Israel's population, which is heavily concentrated in metropolitan areas situated on the coast of the eastern Mediterranean and which was proportionally sampled in this survey. With modern technology enabling widespread desalination of seawater, close proximity to the sea cannot prevent ID, particularly in the absence of prophylactic measures such as USI (20). Even where salt is iodized, other secular trends can influence the consumption of dietary iodine, such as recommendations to restrict salt intake or changes in iodophor use in dairy farming (8,38 –41). In this context, the finding of prevalent ID in a coastal population underscores the vital importance of routine IDD monitoring, not only for Israel but anywhere.
An important strength of this study is that iodine status was assessed in both PW and SAC in parallel. In many countries, the iodine status of the general population is inferred from SAC alone. However, pregnant women have higher requirements for iodine and different dietary patterns than children do. For example, a substantial proportion of total iodine intake in Western diets comes from milk, and milk consumption is typically highest in children (42,43), while women in the same countries can have low intake (44). Thus, focusing on SAC alone can result in an underestimation of deficiency in this critical and vulnerable group (45,46). The finding of prevalent deficiencies in both groups, and of a greater extent of insufficiency among PW than among SAC, underscores the severity of the problem and confirms the value of performing parallel studies in both SAC and PW. Another strength is the innovative use of anonymous pre-discard urine samples collected via a centralized national laboratory (the MHSCL). This provided an efficient and cost-effective method, allowing two nationally representative samples to be generated in six months and at a fraction of the cost compared to other surveys on a similar scale (47,48). Advantage was also taken of the fact that MHS uses electronic records, which facilitated sample selection. Future monitoring surveys in Israel and elsewhere could adopt selected aspects of this effective and efficient model.
This study has several limitations. First, ethical considerations precluded the linkage and analysis of clinical and demographic information for the anonymous pre-discard specimens. Second, unlike the routine urinalysis specimens for PW, specimens collected for SAC were taken from children suspected of illness. We cannot rule out bias due to illness, which might influence dietary intake. Conditions causing change in urinary iodine excretion are rare, and dehydration would tend to increase UIC, suggesting that if there is bias, it would lead to an underestimation of ID prevalence. The high prevalence of low UIC values among SAC (62%) suggests this finding is robust. Third, as we collected urine over a six-month period in the spring and summer, the data may not capture potential annual variation in iodine intake. Several studies elsewhere have reported some seasonal variation of UIC among SAC and PW. A relatively small multicenter study of SAC in the United Kingdom (n = 165) found the median UIC in winter to be 22% higher than in summer. The authors attributed this difference to milk intake, as in England, winter milk iodine concentration is approximately double that of summer milk (49). Seasonal variation in the opposite direction was described in mildly iodine-deficient Nepalese PW (n = 1028) where UIC increased during the dry hot season. This was attributed to a seasonal effect on the availability of dietary iodine from iodized salt in Nepal (50). However, in Israel, where milk and dairy are dominant sources of dietary iodine (39,51), the iodine content of milk and dairy does not show seasonal fluctuations (Ovida YS et al. Eur J Nutr 2017;submitted). Furthermore, salt iodization in Israel is negligible (11), and therefore large seasonal fluctuations in UIC among the Israeli population are unlikely.
In conclusion, the present findings on the current national iodine status in Israel demonstrate that ID is a serious public-health and clinical concern. A USI and monitoring program should be urgently initiated. Caregivers should recommend adequate iodine intake and consider an appropriate iodine supplementation during pregnancy and lactation. A randomized clinical trial of risk and benefit for the correction of mild-moderate ID during pregnancy should be considered, and data on the incidence and prevalence of thyroid disorders in Israel must be urgently obtained.
Footnotes
Acknowledgments
We are indebted to Mrs. Deborah Ruoff from ETH for technical assistance with the UIC analysis; to Dr. Lia Supino from Maccabi Healthcare Services for assistance with data handling; and to Prof. Avi Porath from Maccabi Healthcare Services for discussion of study design. Grants for this study were obtained from the Israeli Ministry of Health Chief Scientists Office (no. 3-00000-12821) and from the Medical Research and Development Fund for Health Services—Jerusalem, with partial support from the Iodine Global Network and the European Union's Horizon 2020 research and innovation programme under “EUThyroid” (grant no. 634453).
Author Disclosure Statement
No competing financial interests exist.