
Abstract
Background:
Facing the prevailing concept that increased diagnosis with no change in mortality drives the increased incidence of differentiated thyroid cancer (DTC), considerable modifications have been introduced in the new edition of the tumor node metastasis (TNM)/American Joint Committee on Cancer (AJCC) staging system. The aim of this study was to compare a group of DTC patients before and after restaging, by mortality, disease severity, and disease outcomes.
Methods:
DTC patients (N = 433) were restaged according to the eighth TNM/AJCC edition, and the results were compared to the seventh edition for clinicopathologic data, treatment modalities, and disease outcomes.
Results:
When switched to the eighth edition, 97.5% of patients fell into stage I-II compared to 76.4% before, and only 11/102 patients remained in stages III–IV. Disease-specific mortality was recorded in 11/433 patients, six of whom were in stages I–II upon restaging, compared to none before (p > 0.05). In addition, more recurrences were seen in stages II (p = 0.05) and III (p = 0.03) using the eighth edition compared to the seventh edition. Stage II was affected the most, with recurrence risk increasing from 29% to 76% (p = 0.001) and persistence at last visit from 19% to 43% when switching to the eighth edition (p = 0.01). Considering stages I and II together, the recurrence risk increased from 16.7% to 28.2% (p = 0.01), lymph node metastases from 1.9% to 26.5% (p = 0.01), and persistence at last visit from 10% to 15% (p > 0.05). Of the 129 patients in the 45- to 54-year-old age group, 53 shifted to stage I (20 from stage II, 29 from stage III, and 4 from stage IV) and five shifted to stage II (all from stage IV). When comparing this age group in stage II only, the eighth edition showed more lymph node metastases (p = 0.001), more distant metastases (p = 0.003), higher recurrence risk (p = 0.002), and more persistence at the last visit (p > 0.05).
Conclusion:
The eighth TNM/AJCC edition provides a more accurate system to discriminate mortality and persistence in DTC patients. Yet, the severity of disease, especially in the 45- to 55-year-old age group and in stage II patients, should not be underestimated following the downstaging of these patients.
Introduction
D
The first American Joint Committee on Cancer Staging Manual was published in 1977 but was only incorporated into the SEER program in 2004, at that time in its sixth edition (6). Thus, the SEER database was enriched with more individual data, allowing a better-stratified analysis of mortality. The American Joint Committee on Cancer/Union for International Cancer Control (AJCC/UICC) reconvened in 2016 to update the tumor node metastasis (TNM) staging system and came up with its eighth edition (7), in which significant changes were introduced regarding thyroid cancer. Following the numerous developments in the field since the seventh edition was published in 2009 (8), the eighth edition presented a more accurate categorization. The main changes are shown in Table 1 and include a rise in the age cutoff from 45 to 55 years for the dichotomous staging system, and the removal of lymph node metastases (LNM) from the T3 definition. In addition, microscopic extrathyroidal extension is no longer considered for staging. As a result, a large proportion of patients are shifted to stage I, with minimal or no impact on the expected 10-year disease-specific survival (DSS) for this stage. The new edition is also expected to improve the allocation of patients at high risk of dying from thyroid cancer into more advanced stages of disease (9).
AJCC/UICC, American Joint Committee on Cancer/Union for International Cancer Control; TNM, tumor node metastatis.
The present study aimed to compare the seventh and eighth editions, not only for mortality but also for disease severity at diagnosis and response to treatment during follow-up.
Methods
The study was conducted in the Assaf Harofeh Medical Center (Israel) and was approved by the local institutional ethical board. A computer search was performed using “thyroid neoplasm” as a keyword for all the hospital's records for 1995–2015. Medical charts were reviewed, and patients with a proven diagnosis of epithelial-derived thyroid carcinoma were included.
The following clinical variables were collected from the registry: patient age and sex, type and time of surgery, histopathology findings, extent of primary disease, extrathyroidal extensions, TNM staging, 131I therapy, and number and type of additional treatments. Stimulated thyroglobulin (stTg) levels measured postoperatively, just before ablation, and during follow-up were recorded as well.
All patients were monitored by standard methods, including clinical examination, thyroid function tests, neck sonogram, radioiodine scan, and serum Tg and anti-Tg antibodies levels. Some patients also underwent other radiological tests, as required, including computed tomography, positron emission tomography/computed tomography, magnetic resonance imaging, and bone scan.
Persistent or recurrent disease was diagnosed based on histopathology, imaging studies, and Tg levels. Disease-free status or remission was defined as the absence of structural disease combined with undetectable suppressed Tg and/or at least one stTg measurement <2 ng/mL in the absence of anti-Tg antibodies. All patients were staged based on the AJCC TNM seventh edition system and compared to the recently published eighth edition (Table 1). For the prediction of recurrence and/or persistence, patients were classified according to the 2015 modified ATA initial risk-stratification system (5).
Quality control of the registry data was performed by data verification on several occasions. Levels of thyrotropin, free thyroxine, Tg, and anti-Tg antibodies were measured by chemoluminescence assay (Immulite 2000; Diagnostic Products Corp.). For the Tg assay, the functional sensitivity was 0.9 ng/mL, and the analytical sensitivity was 0.2 ng/mL.
Statistical analysis
Numerical data are expressed as mean ± standard deviation, and categorical data are expressed as percentages. An independent t-test was used to evaluate between-group differences, and a chi-square test was used to evaluate the relationship between clinical characteristics. A p-value of <0.05 was considered significant.
Results
During 1962–2015, a total of 441 non-medullary thyroid cancer patients were treated at the authors' institution (414 during 1990–2015). Their clinicopathologic characteristics were: mean age 47.7 years (60%> 45 years old), female 75.5%, familial 9.5%, radiation exposure 7.2%, PTC 89.1% (classical 63.3%, follicular variant 25.8%), follicular thyroid cancer 6.7%, and others 4.2%. Disease extent at diagnosis was microcarcinoma 33%, multifocality 38.3%, extrathyroidal extension 20%, LNM 27.4%, DM 4.2%, and TNM seventh edition stages III–IV 25.7%. Near-total thyroidectomy was performed in 86.6% and neck dissection in 25.7% of patients. Radioactive iodine (RAI) therapy was administered to 86.5% patients, with a mean first dose of 110 mCi. Additional treatment during follow-up included reoperation in 8.5% and repeated RAI in 34.8%, for a median cumulative dose of 130 mCi (25% received >200 mCi). Overall, out of 427 patients with available data, 35 (8.2%) presented DM, 18/427 (4.2%) at diagnosis and 17/427 (4.0%) during follow-up. Persistent disease was recorded in 25% of patients at one year and 16% at the last visit. With a mean follow-up of 9.7 ± 8.8 years, the overall mortality (OM) was 8.8% (39/441) and disease-specific mortality (DSM) was 2.5% (11/441).
Comparison of AJCC/UICC TNM eighth versus seventh editions
Out of the 441 DTC patients, 433 patients had complete data, which allowed them to be included in the comparison of the seventh and eighth editions of the AJCC/UICC staging system. Their TNM distribution by stage and edition is presented in Table 2 and Figure 1. The data revealed that while the TNM stage was unchanged in most patients, it was downstaged in 127 (29.3%) of them (Table 3). When shifting to the eighth edition, 97.5% (422/433) were in stages I–II compared to 76.4% (331/433) when using the seventh edition (Table 3). PTC classical and follicular variants were equally distributed: 90% and 89.5% in both editions.
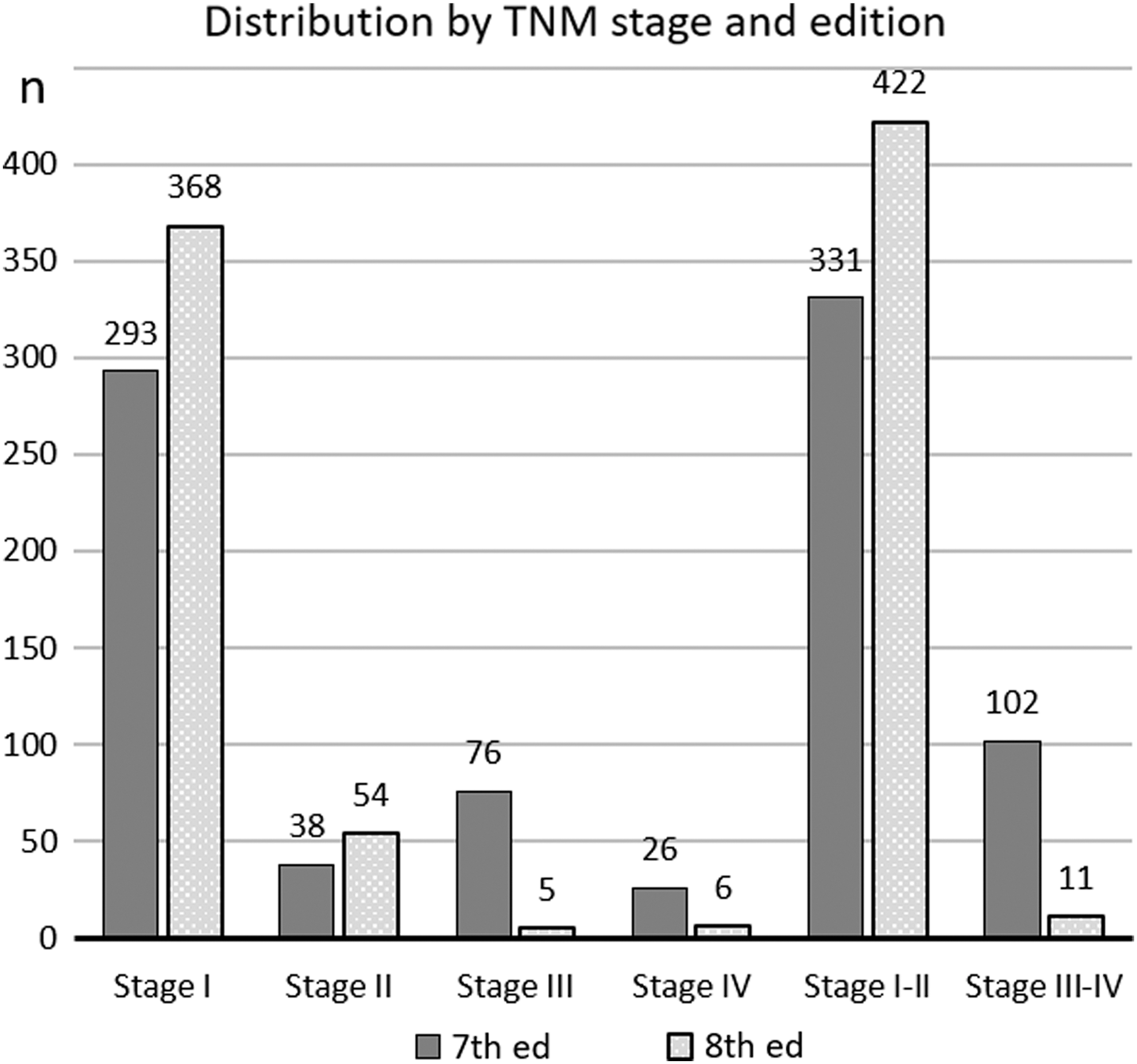
Proportion of patients with differentiated thyroid cancer in stages I–IV according to the tumor node metastasis (TNM) seventh (dark bars) and eighth (light bars) editions.
Statistically significant values are shown in bold.
ATA, American Thyroid Association; RAI, radioactive iodine; PTC, papillary thyroid cancer; PTCFV, follicular variant of PTC; DM, distant metastases; LN, lymph nodes; ns, not significant.
When comparing the seventh and eighth editions for stages I–II only, the proportion of intermediate/high-risk patients increased from 16.7% (54/323) to 28.2% (117/414; p = 0.001), LNM from 1.9% (6/320) to 26.5% (112/422; p = 0.001), all DM from 5.2% to 8.3%, and DM at diagnosis from 2.2% to 3% (p > 0.05). RAI at initial treatment was given to 82.4% and 85% patients (p > 0.05), at a mean dose of 102.6 ± 45 mCi versus 110.6 ± 46 mCi (p = 0.04), respectively. Reoperation was performed in 5% versus 8.1% of patients, and additional RAI treatment was given to 17.3% versus 20.4% of patients, with a median cumulative dose of 102 versus 130 mCi (p > 0.05). A trend toward more disease persistency at one year (from 17.7% to 22.7%) and last visit (from 8.7% to 13.5%) was observed as well.
Regarding stage I, no significant differences were noticed between the eighth and seventh editions, with an OM of 5.4% versus 4% and DSM of 0.5% versus 0%, respectively. In contrast, shifting 45 stages III–IV patients to stage II resulted in the new stage II category being affected the most (Fig. 2). According to the eighth edition, stage II patients have more LNM (65% vs. 2.7%; p = 0.001), a 4- and 1.7-fold increase in intermediate and high recurrence risk (p = 0.01), more reoperations (20% vs. 0%; p = 0.01), more persistency at last visit (43% vs. 19%; p = 0.04), and a nonsignificant increase in DSM (7.5% vs. 0%), compared to previous stage II patients. Of note, 5/54 patients in stage II according to the eighth edition were stage IV in the seventh edition.
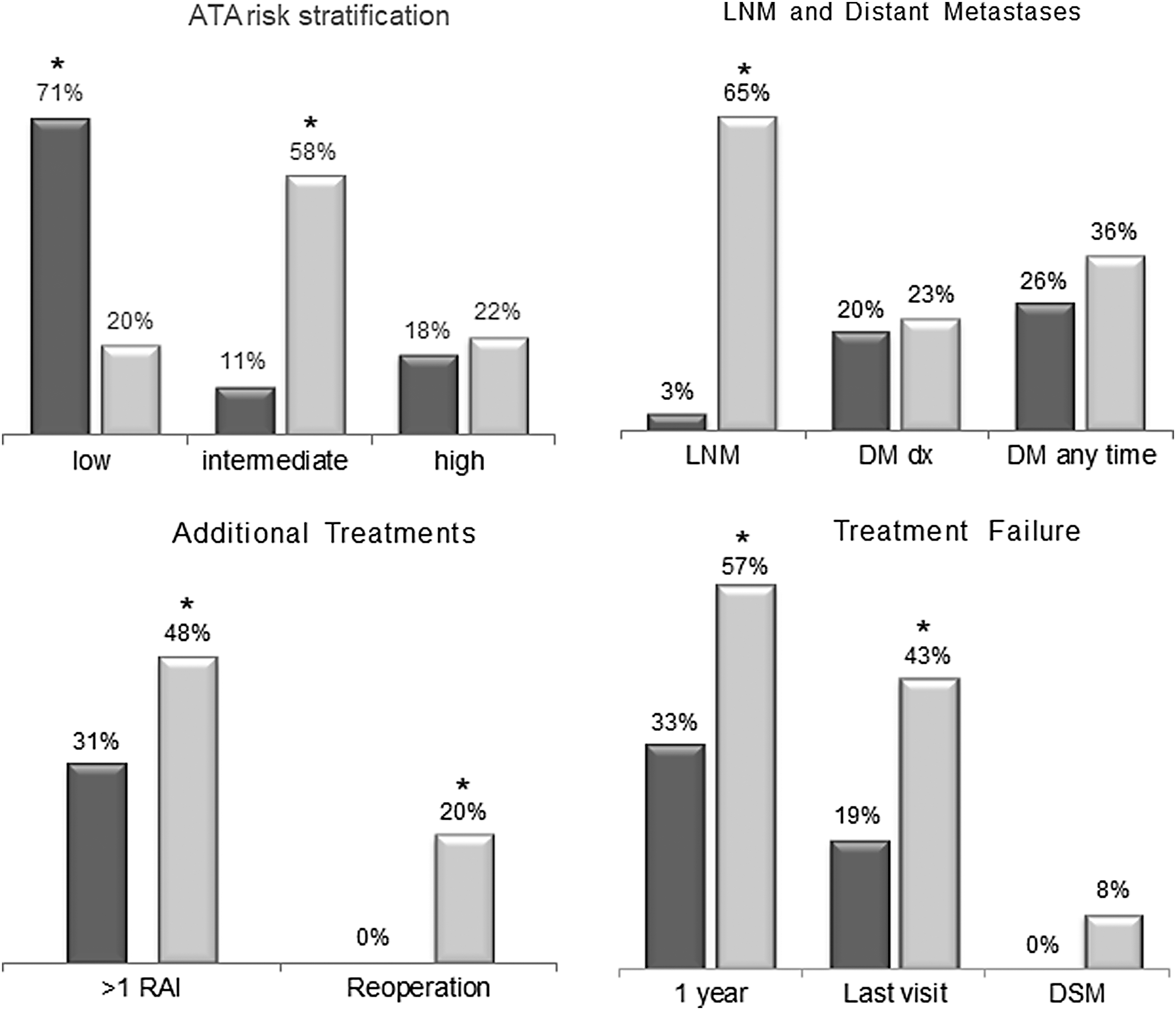
Disease severity and outcome in stage II differentiated thyroid cancer patients according to the seventh (n = 38; dark bars) and eighth (n = 52; light bars) TNM editions (*p ≤ 0.05).
Of the 371 stage I patients according to the eighth edition, 293 were stage I before, but 78 were not (stage II = 31, stage III = 42, and stage IV = 5). Stage III patients according to the seventh edition (n = 76) were shifted to stage I (n = 42) and stage II (n = 34), while those in stage IV (n = 26) were shifted to stage I (n = 5), stage II (n = 11), and stage III (n = 4), with six remaining in stage IV. Overall, only 10 (2.3%) patients according to the eighth edition were at stages III–IV compared to 102 (23.5%) before.
ATA risk stratification in eighth edition versus seventh edition
In the present cohort, 425 patients with sufficient data were categorized according to the ATA persistence/recurrence risk-stratification system as follow: 69.9% (297/425) low-risk group, 25% (106/425) intermediate-risk group, and 5.2% (22/425) high-risk group. The available data showed persistence/recurrence disease in 15.8% (42/266) of low-risk patients, 35.9% (32/89) of intermediate-risk patients, and 80.9% (17/21) of high-risk patients.
The ATA risk stratification shifted between editions (Table 2). According to the eighth edition, the low-risk group was shifted in stage I from 85% to 79%, in stage II from 72.7% to 28.3%, and in stage III from 39% to 0%, while no shift was seen for stage IV in either edition. The intermediate-risk group shifted in stage I from 15% to 20.6%, in stage II from 6.1% to 43.5%, in stage III from 61% to 75%, and in stage IV from 39.1% to 0%. The high-risk group in stage I shifted from 0% to 0.4%, in stage II from 21.2% to 28.2%, in stage III from 0% to 25%, and in stage IV from 60.9% to 100%.
While rates of persistence/recurrence of disease in stage I were similar in both editions, persistence/recurrence rates were significantly higher in stages II (p = 0.05) and III (p = 0.03) in the eighth edition compared to the seventh edition (Fig. 3). When considered together, stages III–IV in the eighth edition captured 80% (8/10) of persistence/recurrence compared to 57% (45/79) in the seventh edition (p > 0.05).
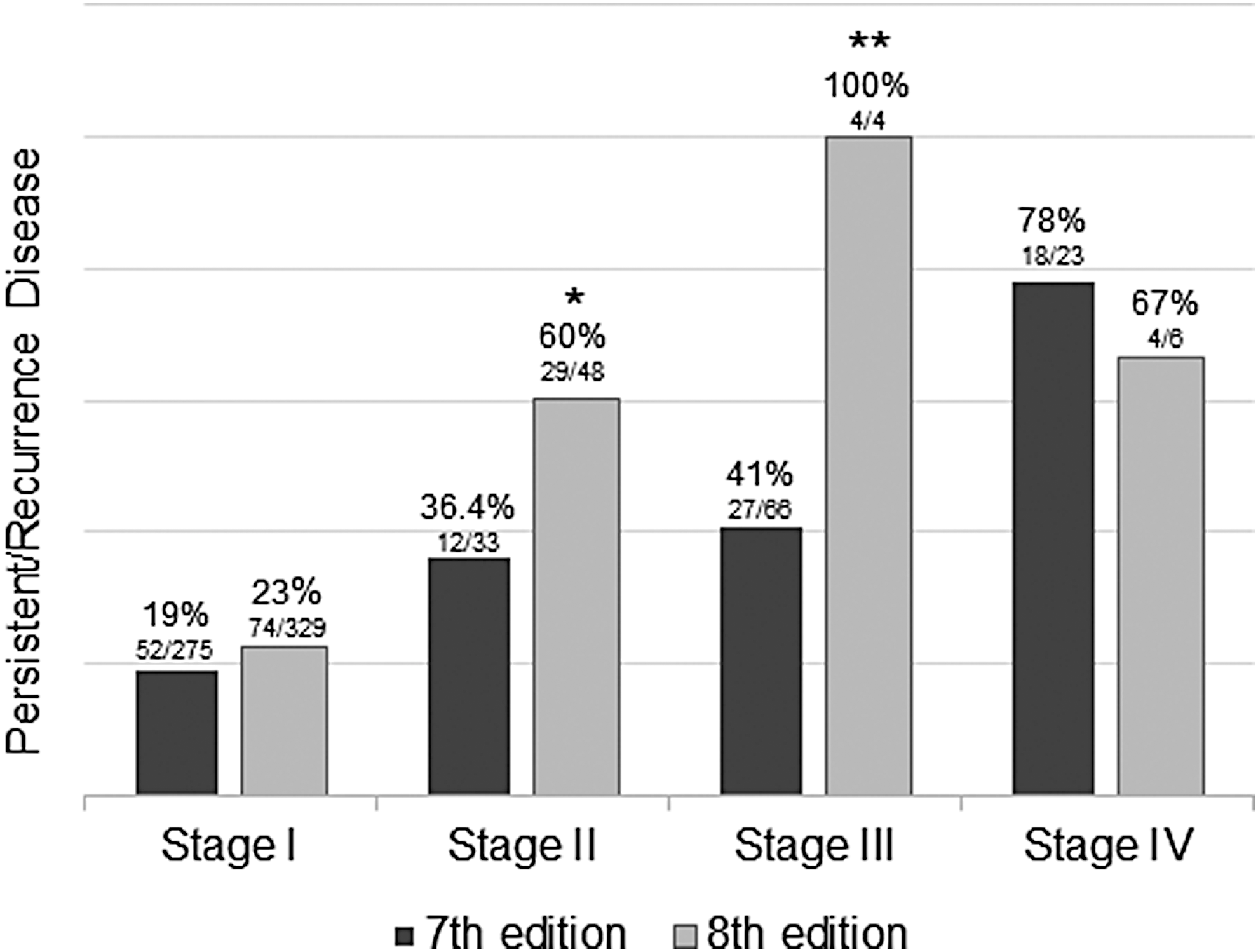
Comparison of the number of patients with persistence/recurrence of disease according to the seventh (dark bars) and eighth (light bars) TNM editions (*p = 0.05; **p = 0.03).
OM and DSM
Throughout 9.7 ± 8.8 years of follow-up, 38/432 (8.8%) all-cause death events were recorded. When comparing the eighth edition to the seventh, 33/421 (7.8%) were stages I–II versus 15/331 (4.5%), and 5/11 (45.4%) were stages III–IV versus 23/101 (22.8%; p > 0.05). Overall, DSM occurred in 11/432 (2.6%) of patients. Using the eighth edition, 6/421 were stages I–II compared to 0/331 before (p > 0.05), and 5/11 were stages III–IV compared to 11/100 before (p = 0.001). Thus, 54.5% of all DSM occurred in stages I–II when using the eighth edition compared to none using the seventh edition. The distribution of disease mortality by stages in the eighth edition was stage I = 2/368, stage II = 4/53, stage III = 1/5, and stage IV = 4/6, while in the seventh edition it was 0/293, 0/38, 5/76, and 6/25, respectively.
Restaging of DTC patients in the 45- to 55-year-old age group
After the restaging of all 127 patients in the 45- to 55-year-old age group, those who were previously in stage III (n = 29) and stage II (n = 20) were shifted to stage I, while those in stage IV (n = 9) were shifted to stage II (n = 5) and stage I (n = 4; Table 4). By definition, no patient in the 45- to 55-year-old age group remained at stage III or IV following restaging. In this group, the proportion of intermediate risk among stage I patients increased from 5.7% to 18.5% (p = 0.04), and those at high risk in stage II increased from 0% to 100% (p = 0.002). There was also a significant increase in the rate of LNM, DM, and disease persistency, both at one year and at the last visit (Table 4). Mortality could not be assessed due to the small sample size. However, among the 45- to 55-year-old patients in stages I–II according to the eighth edition, there were two cancer-related deaths compared to none according to the previous edition, representing an increase in DSM from 0% to 1.5% for this age group upon restaging. The characteristics of 53 patients restaged to stage I are shown in Table 4. This group has significantly more males (37.7% vs. 18.3%), LNM (50% vs. 1.4%), intermediate ATA risk (36% vs. 6%), all-time DM (9.6% vs. 1.4%), and one-year persistency (32% vs. 11%) compared to the original stage I patients according to the seventh edition. Moreover, a nonsignificant trend of more persistency at last visit (13% vs. 4.6%) and cancer-related deaths (1/53 vs. 0/70) was noted.
p vs. Stage I, 7th edition.
SD, standard deviation.
Discussion
The current study used mortality, disease severity at diagnosis, and response to treatment during follow-up to compare the seventh and eighth editions of the TNM staging of DTC. After restaging the cohort of DTC patients using the new TNM eighth edition, nearly one-third of patients shifted from stages III–IV to stages I–II, and this was mainly because of the changes in tumor stage and age-group cutoff introduced in the new edition. The downgrading of size and minimal extrathyroidal extension resulted in a shift of T3 and N1 patients from stages III–IV to stage II. Furthermore, the proportion of intermediate/high ATA risk patients in stages I–II according to the eighth edition increased considerably compared to the previous edition, resulting in 60% more patients at higher ATA risk within this stage category. Accordingly, more LNM and more residual disease were observed in stages I–II when using the eighth edition. Considering each stage group separately, the 18% of patients reclassified to stage I, with the estimated 10-year mortality unchanged (<1%), had more LNM as the only statistically significant difference. In contrast, the stage II patients reclassified by the eighth edition had not only more LNM but also more intermediate and high recurrence risk, more reoperations, more persistency at last visit, and a nonsignificant increase in DSM compared to the previous edition.
The second major change between the two editions was transferring the age cutoff from 45 to 55 years (7). As the dichotomous use of age in the staging of thyroid cancer patients is being challenged by data showing higher risk with age as a continuous variable (10 –12), the rise in the age cutoff introduced in the eighth edition appears to follow an opposite direction. In the present cohort, moving one-third of patients in the 45- to 55-year-old age group from stages III–IV to I–II resulted in a higher risk of recurrence, more all-time DM, a higher rate of persistent disease at last visit, and an elevation in the DSM incidence. These data clearly demonstrate the presence of more aggressive disease and worse outcomes in some patients within stages I–II as defined by the eighth edition compared to this stage of the seventh edition. Similar results were observed by Rosario (13), who reported about a 3% disease mortality rate among 68 patients in this age group, all of whom were moved to stage I from stage IV upon switching editions.
Although the TNM system was meant to assess mortality (14), the boundaries between mortality and severity of disease overlap because the latter is strongly and independently affected by the T, N, and M status. Thus, by moving 30% of DTC patients from TNM stages III–IV to stages I–II in this study, the eighth edition may induce a false impression of less aggressive disease. This is in contrast with the fact that nearly half of the cancer-related deaths are now seen in stages I–II compared to none in the previous edition. Nevertheless, the eighth edition performed better for stage IV by recording DSM in 4/6 patients compared to 7/25 in the previous edition.
Shortly after the eighth edition became available, two studies were published comparing the eighth and seventh editions for thyroid cancer. The first one by Kim et al. (15) was a hospital-based analysis of 1613 DTC patient. Similar to the present data, a shift in patients in stages I–II from 64% to 97%, leaving only 3% at stages III–IV, was reported. Despite the small sample, DSS rates for the eighth versus seventh editions were reported as follows: stage I 96.6% versus 99.7%, stage II 95.4% versus 98.2%, stage III 83.2% versus 98.8%, and stage IV 48.6% versus 72.3%. The authors concluded that the eighth edition outperformed the seventh edition due to the ability to capture high-risk mortality patients. However, as in the present study, their sample was too small; the conclusions were based on only 32 events of cancer-related deaths. The second study published by Pontious et al. (16) used the SEER program (n = 64,342) and the National Cancer Database (NCDB; n = 179,698) for comparison. A shift in patients in stages I–II from 83% to 98%, leaving only 2% in stages III–IV, was reported when using the new edition. The baseline characteristics of the study population were at variance with other hospital-based registries such as the present one, with <50% of patients receiving RAI therapy at initial treatment, lower rates of LNM and DM at diagnosis, higher incidence of stage I (76%), and lower incidence of stage III (12%), as defined utilizing the seventh edition. Due to the short follow-up (median 54 months) in the study by Pontious et al., only the five-year DSS rates were reported for the eighth versus seventh editions as follows: stage I 99.7% versus 99.8%, stage II 96.7% versus 99.1%, stage III 85.2% versus 98.8%, and stage IV 66.9% versus 88.2%. This contrasts with the expected 10-year DSS of 60–70% and <50% for stages III and IV, respectively, as estimated by a senior author of the new TNM edition (9).
For the prediction of disease mortality to be accurate, any staging system should include data on treatment modalities and individual response to treatment. At the authors' institution, as in many others, the approach to thyroid cancer is a dynamic process that changes over time. Guidelines are not uniform and are updated as more research evolves. Therefore, patients today are not treated as they were 20 years ago. Yet, the TNM system only refers to the time of diagnosis, irrespective of many other variables that may affect the risk of dying from thyroid cancer. Disease survival in stage I patients would not be the same if BRAF and TERT promoter mutations were present, or if DM develop during follow-up, or if the patient was only partially treated. Today, there are at least 17 different staging systems for the prediction of DTC mortality. Lang et al. (17), in a comparative study from 2007, investigated the differences between systems, concluding that the MACIS, TNM sixth edition, and EORTC performed the best. When the seventh TNM edition came out three years later, it became the most widely accepted system. The issue of whether the AJCC TNM eighth edition will outperform the previous one still needs to be validated (9).
A selection bias in the present cohort cannot be excluded, since our institution is a tertiary referral center, and it may have treated a relatively high number of patients with DM. Furthermore, the data are at variance with the low rate of DM at diagnosis in the SEER database (16). Other authors have also reported rates for DM at diagnosis in the range of 2–4% (15,18,19), and up to 6.3% on long-term follow-up (20).
A main limitation of this study is its small sample size and the few DSM events. Although the TNM staging system is a tool used to predict mortality, mortality from DTC is very rare. While disease persistency and progression are noted in up to 20–35% of patients in most series, the rate of DSM is only 2–4% (5) To validate the 55-year cutoff age, Nixon et al. (10) needed to combine 10 different hospital-based registries to reach 9500 patients that yielded 224 thyroid cancer deaths. Furthermore, most systems of recurrence risk prediction are based on the T, N, and M characteristics of the initial tumor. Thus, the implications of the above are as follows. First, mortality analysis can be conducted only by using large databases such as the SEER or NCDB. However, large population-based registries lack the individual data necessary for better accuracy, as shown by Lim et al. (2). Second, the focus in clinical research should be to minimize persistency and disease progression, which results in additional treatments, leading to a worse quality of life. To some extent, this has been addressed by the TNM editorial board, with a pilot chapter on “Risk-assessment models” included now for lung, prostate, melanoma, breast, and colon cancer in the new edition (6). By doing so, the TNM editorial board acknowledged the importance of the current trend toward a more personalized approach (6).
Specifically, for thyroid cancer, where persistency/recurrence outnumbers mortality by 10- to 20-fold, there is a need to reconsider the goals of the TNM system, so that it will be more clinically applicable (9). The present study is unique in that both editions are compared in the context of the ATA persistence/recurrence risk system. There was nearly a twofold increase in persistence/recurrence disease rates for stages II–III patients according to the eighth edition compared to the same stages in the seventh edition. These findings add to the improvements of the new edition to discriminate patients better at high risk of not only disease mortality but also disease recurrence.
While the cohort is too small to make conclusions on mortality, it emphasizes that physicians caring for DTC patients should base their prognosis assessment not only on mortality but mainly on persistence/recurrence risk stratification systems, such as the ATA classification or similar. They should also be aware that, at variance with the previous version, the downstaging of DTC patients according to the TNM eighth edition does not necessarily reflect less aggressive disease in all patients.
Footnotes
Author Disclosure Statement
The authors confirm that there is no conflict of interests.