
Abstract
Background:
Although The Bethesda System for Reporting Thyroid Cytopathology has provided clinicians with a standardized classification scheme for the diagnosis of thyroid fine-needle aspiration cytology (FNAC) specimens, the indeterminate categories of Bethesda III (B3)—atypia of undetermined significance/follicular lesion of undetermined significance (AUS/FLUS)—and Bethesda IV (B4)—follicular neoplasm/suspicious for follicular neoplasm (FN/SFN)—continue to pose challenges with regards to ideal diagnostic and therapeutic management. Having previously demonstrated the presence of nuclear atypia as a high-risk subgroup in B3, the objective of this study was to evaluate the malignancy rates in the B4 subgroup with nuclear atypia.
Methods:
A retrospective review of all thyroid FNACs diagnosed as B4 (FN/SFN) between 2008 and 2015 was conducted at a tertiary referral center in Singapore. Data on patient demographics, sonographic features, and final histological diagnosis were collected. This was compared to data from a previous analysis on all nodules diagnosed as B3 (AUS/FLUS) over a similar period.
Results:
A total of 137/309 (44.3%) and 88/111 (79.3%) FNACs diagnosed as B3 and B4, respectively, underwent surgical excision yielding final histopathological diagnoses. The malignancy rate of B4 was 31/88 (35.2%) compared to B3, which was 37/137 (27.0%). Subclassification based on the presence of architectural versus nuclear atypia showed significantly higher malignancy rates in B4 nodules with nuclear atypia (21.8% vs. 57.6%; p < 0.01). These findings corroborate previous results within the B3 category (malignancy rate of 14.7% vs. 36.8%; p < 0.01). The only sonographic features predictive of malignancy were the presence of macrocalcifications in B4 compared to irregularity of margins in B3.
Conclusion:
The presence of nuclear atypia identifies subgroups with significant differential malignancy risks within both the B3 and B4 categories. This supports the notion that subclassification is a useful risk stratification tool that can guide diagnostic and therapeutic management of indeterminate thyroid nodules with heterogenous risk profiles.
Introduction
T
The current standard of care in the diagnosis of thyroid cancer is the use of fine-needle aspiration cytology (FNAC), as it is the most accurate and cost-effective method for evaluating thyroid nodules, with cytopathologic reporting based on The Bethesda System for Reporting Thyroid Cytopathology (TBSRTC) as recommended by the 2015 American Thyroid Association (ATA) management guidelines (5).
TBSRTC was introduced in 2009 with the purpose of standardizing terminology and therefore triaging nodules in terms of surgical management. It classifies FNAC diagnoses into six different cytopathologic categories, each with its corresponding estimated risk of malignancy (6). This standardized system has not only allowed clinical correlation in the form of risk stratification, but has also proven to be a robust and accurate classification scheme since its implementation (7), reducing unnecessary surgery, thereby reducing the risk of possible recurrent laryngeal nerve injury, hypoparathyroidism, and the need for completion total thyroidectomy (8).
Despite this improvement, there remains a unique indeterminate group of FNAC diagnoses, namely Bethesda III (B3)—atypia of undetermined significance/follicular lesion of undetermined significance (AUS/FLUS)—and Bethesda IV (B4)—follicular neoplasm/suspicious for follicular neoplasm (FN/SFN). Prior to TBSRTC, indeterminate lesions accounted for a highly variable group consisting of lesions that could not be confidently labeled benign or malignant, including atypical lesions, cellular follicular lesions, and follicular neoplasms, thus resulting in highly variable malignancy rates and frequent non-therapeutic thyroidectomies (9). However, despite post-Bethesda classification into B3 (AUS/FLUS) and B4 (FN/SFN), both groups continue to exhibit wide inter-institutional variability in terms of predicting malignancy, with malignancy rates ranging from 15.7% (10) to 81% (11) and 11.1% (12) to 65.7% (13), respectively. This is in contrast to the proposed risk of malignancy by TBSRTC of 5–15% and 15–30%, respectively (6).
Several studies have proposed the use of subclassification of the B3 category in view of this heterogeneity to identify higher-risk subgroups and to refine management protocols, in particular, based on the presence of nuclear atypia. For B3, several studies have shown an increased risk of malignancy in nuclear atypia subgroups (14 –17), while for B4, the same can also be demonstrated (18 –20). The international panel for the second edition of TBSRTC supports this notion, recommending subclassification of B3, particularly with respect to the presence or absence of nuclear atypia, while also commenting on classifying follicular patterned lesions with atypia as B4 instead of suspicious for malignancy, in view of the introduction of noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) (21).
This retrospective study sought to compare the malignancy rates and outcomes of FNACs diagnosed as B3 (AUS/FLUS) and B4 (FN/SFN) at a tertiary referral center and to explore the effects of subclassification in identifying high-risk groups. Through this, the study sought to identify possible relationships between the two Bethesda groups and among the subgroups in order to provide a more clinically meaningful viewpoint that can better guide management.
Materials and Methods
A retrospective review was conducted at the National University Hospital (NUH), Singapore, which is a tertiary referral center. This study was approved by the Institutional Review Board (IRB number: 2016/00142). The database of the Department of Pathology was searched for all thyroid FNACs with the keyword “follicular neoplasm” between the dates January 1, 2008, and September 30, 2015, and subsequently filtered down to a list of all B4 (FN/SFN) FNAC diagnoses. Full cytology reports were reviewed for all cases, and for inconsistent reports or pre-Bethesda cases in particular, cytology slides were re-evaluated by a single experienced cytopathologist to ensure consistency of reporting and diagnoses with cytological findings according to the latest terminology.
All FNACs were performed by experienced clinicians, cytopathologists, or radiologists using a 23–25 Fr gauge needle, with two to five passes performed mostly under the guidance of ultrasound imaging. FNAC samples were subjected to rapid on-site evaluation of adequacy by trained cytotechnologists using air-dried smears stained with Hemacolor stain. Remaining slides were fixed in alcohol and stained with the Papanicolau stain for final cytopathologic analysis.
Nodules with follicular cells arranged predominantly in microfollicular or trabecular arrangements were classified as FN/SFN. Nodules composed exclusively of oncocytic cells without a history of Hashimoto's thyroiditis were denoted as FN, Hürthle cell variant.
For each FNAC sample, patient demographics, follow-up data, preoperative ultrasound findings, and postoperative histopathological results were retrieved. This included age, sex, previous and repeat FNAC results, and ultrasound features such as number of nodules, size of nodule, laterality, heterogeneity, echogenicity, presence of micro (<1 mm) or coarse (≥1 mm) calcifications, and presence of internal vascularity. Histopathological data of those who underwent surgical treatment were correlated with the corresponding cytological diagnosis.
Malignant outcomes were designated as papillary (PTC), follicular (FTC), medullary (MTC), and anaplastic thyroid carcinoma (ATC), with further subclassification of PTCs into classical (CPTC) or follicular variants (FVPTC), and FTCs into minimally invasive or widely invasive. FVPTC slides were further examined, and histopathological reports were corroborated, where available, to establish a retrospective diagnosis of NIFTP based on the criteria proposed by Nikiforov et al. (22). Lymphomas were also included as malignant outcomes. Incidental papillary microcarcinomas in the samples were classified as indolent lesions in accordance with the 2015 ATA management guidelines (5).
The only exclusion criterion for this study was patients who had a FNAC record but no retrievable patient data.
The results of this study were compared and analyzed to that of a previous study addressing the outcomes and clinical and radiological features of thyroid nodules, with cytology results classified into the TBSRTC B3 (AUS/FLUS) category (17). The nodules within this category were subdivided into those with only architectural atypia (microfollicular formations, crowding) versus nuclear atypia (nuclear enlargement, pallor, grooves) (17). For clarity, nodules in which both architectural and nuclear atypia were seen were placed in the nuclear atypia group.
Statistical analysis was performed using IBM SPSS Statistics for Windows v23 (IBM Corp., Armonk, NY). Ordinate variables were assessed for significance using Pearson's chi-square analysis, while continuous variables were evaluated using an independent samples t-test, with the significance level set at p < 0.05.
Results
A total of 309 and 111 FNACs were diagnosed as B3 (AUS/FLUS) and B4 (FN/SFN), respectively, over the study period. The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram in Figure 1 illustrates the outcomes of these patients. For AUS/FLUS and FN/SFN, 137 (44.3%) and 88 (79.3%) patients, respectively, underwent surgical resection to obtain final histopathological diagnosis and were included in this study.
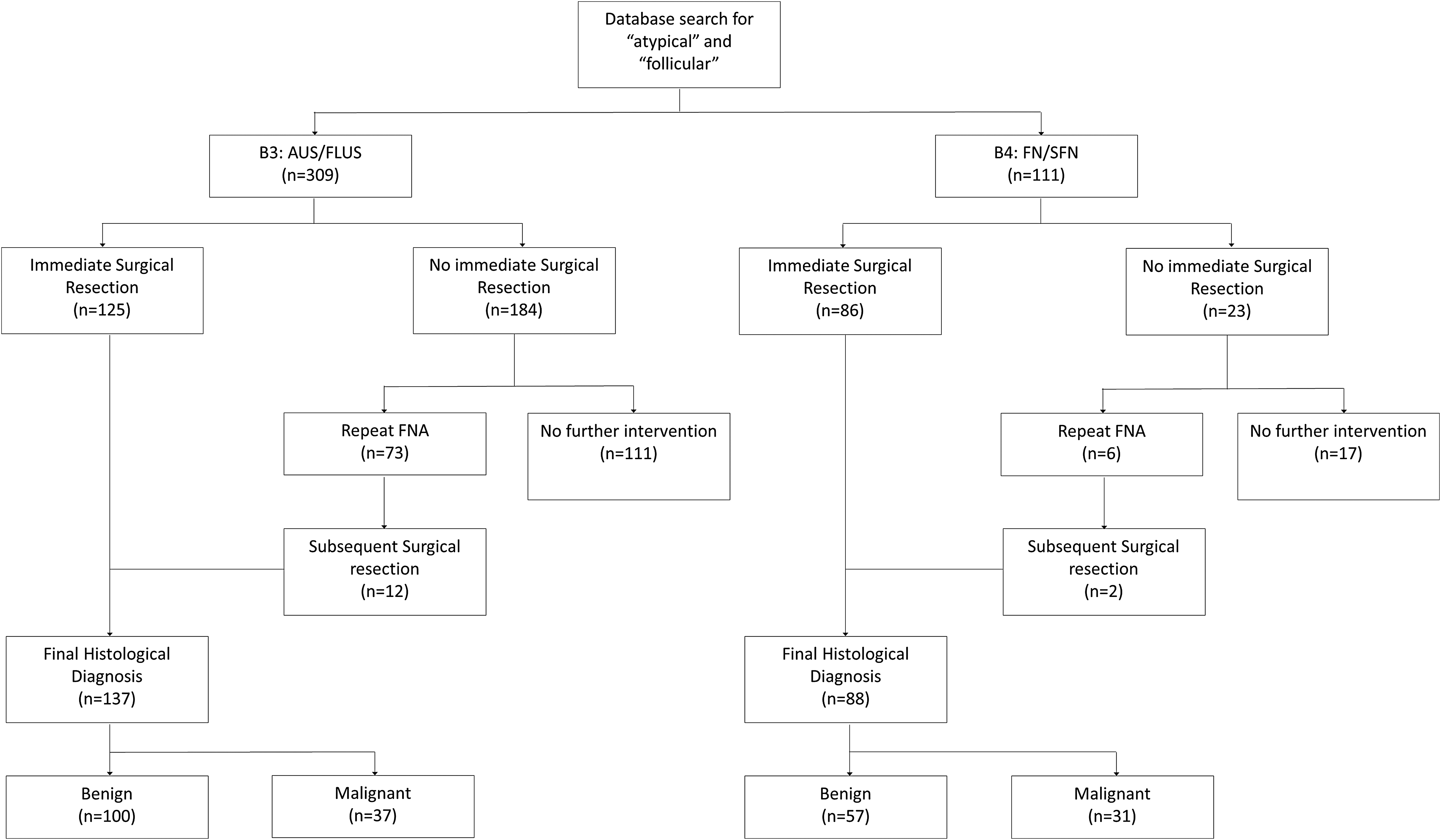
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram illustrating follow-up of 309 and 111 patients who had fine-needle aspiration cytology (FNAC) diagnosed as Bethesda III (B3) and Bethesda IV (B4), respectively. AUS/FLUS, atypia of undetermined significance/follicular lesion of undetermined significance; FN/SFN, follicular neoplasm/suspicious for follicular neoplasm.
The B4 group in the current study had a median (interquartile range) age of 49.0 years (34.3–57.0 years) and a sex distribution of 34 (38.6%) males and 54 (61.4%) females, as indicated in Table 1. When compared to the demographics of the B3 group from a previous study, only sex distribution showed borderline significance, with the B3 group having more females (p = 0.05) (17), as depicted in Table 2.
IQR, interquartile range; NS, not significant; SEM, standard error of the mean.
With regards to the malignancy rate of the B4 group, 31 (35.2%) of the resected nodules were malignant, comprising 11 PTCs, 19 FTCs, and two MTCs. Of the 11 PTCs, eight were reported as FVPTC. All cases were either partially encapsulated or well demarcated from the normal thyroid parenchyma without a definite capsule. None of the eight cases could be classified as NIFTP due to the presence of lymphovascular invasion (n = 4), >1% papillae (n = 3), focal infiltration into the adjacent parenchyma (n = 1), the presence of significant insular component (n = 1), and the presence of psammoma bodies (n = 1). In some tumors, more than one criterion for exclusion was present (22).
Benign nodules comprised neoplastic lesions such as follicular/Hürthle cell adenomas and non-neoplastic lesions such as adenomatous/hyperplastic nodules and multinodular goiters. This is comparable to the B3 group from a previous study, wherein 37 (27.0%) of the resected nodules were malignant, comprising 22 PTCs, seven FTCs, one MTC, one ATC, and six lymphomas (17).
In terms of ultrasound features predictive of malignancy, only the presence of macrocalcifications (>1 mm) was significant in predicting malignancy in the B4 group (p < 0.01), as indicated in Table 1.
Comparative analysis of ultrasound features showed some significant differences between B3 and B4, as depicted in Table 2. With regards to laterality, there were significantly more unilateral nodules in the B3 group (p = 0.04) compared to the B4 group, which was predominantly bilateral (p < 0.01). In terms of nodule components, there were more solid nodules (p < 0.01) in the B4 group but more solid/cystic nodules (p = 0.01) in the B3 group. For sonographic characteristics, there were more isoechoic nodules (p < 0.01) in the B4 group.
Subgroups with nuclear atypia
Subgroup analysis was performed for the B4 group and compared to the B3 group according to the presence of nuclear atypia, as depicted in Table 3. For B4, the malignancy rate was significantly higher in the FN with nuclear atypia group at 57.6% (19/33) compared to the FN without nuclear atypia group at 21.8% (12/55; p < 0.01). This demonstrates a similar trend previously observed in the B3 group, whereby the malignancy rate was also significantly higher in the nuclear atypia group at 36.8% (21/57) compared to the architectural atypia group at 14.7% (11/75; p < 0.01) (17).
FN, follicular neoplasm; CPTC, classical papillary thyroid carcinoma; FVPTC, follicular variant papillary thyroid carcinoma; FTC, follicular thyroid carcinoma; MTC, medullary thyroid carcinoma; ATC, anaplastic thyroid carcinoma; MALT, mucosa-associated lymphoid tissue.
When comparing the malignancy outcomes of B4 to the B3 subgroups, B4 had a significantly higher malignant outcome compared to the B3 architectural atypia group (p = 0.04), but there was no significant difference compared to the B3 nuclear atypia group (p = 0.86). In other words, the malignancy rate in the B3 group with nuclear atypia was comparable to the overall malignancy rate in the B4 group.
Discussion
TBSRTC has been well established as an accurate, reliable, and valid reporting system for thyroid cytology since its inception, bringing about standardization that is invaluable in not only the diagnosis, but also the management of thyroid nodules based on a risk of malignancy approach (7). Under the current TBSRTC established in 2009, the risk of malignancy for B3 (AUS/FLUS) and B4 (FN/SFN) is estimated at 5–15% and 15–30% respectively (6). In contrast, both the previous B3 study (17) and current B4 study have shown the authors' institutional malignancy rates to be higher at 27.0% and 35.2%, respectively. With regards to the B4 group, the malignancy rate of 35.2% is comparable to other studies (32.1–36.4%) (23 –30). This is also corroborated by a meta-analysis of the TBSRTC done by Straccia et al. in 2015, which included a total of 51 studies evaluating the indeterminate categories of B3 and B4, showing an overall rate of malignancy of 27% and 31%, respectively (31).
There was no significant difference between the malignancy rates when comparing B4 to B3 in the present study (p = 0.23). This is interesting because despite a significant difference in surgery rates between B3 and B4 lesions (44.3% and 79.3%, respectively), the malignancy rates are similar. One of the possible reasons for the increased malignancy rate observed in the B3 group could be due to the fact that a subset of patients in this category did not undergo surgery. This is consistent with the 2015 ATA guidelines, which recommend repeat FNAC and follow-up rather than a diagnostic lobectomy for B3 (5). In the present study, only 44.3% (137/309) underwent surgery for a definitive histopathological diagnosis, but this is similar to other studies and possibly overestimates the risk of malignancy due to inherent selection of patients with additional clinical risk factors (32,33).
There are other inherent differences between the B3 and B4 groups beyond the cytological criteria. Differences were found in terms of nodule laterality between the two groups, but this was likely due to an unequal distribution of the total number of nodules, as there were simply many more B3 than B4 nodules.
There were also differences in ultrasound features between the B3 and B4 groups. It was observed that there were more solid (p < 0.01) and isoechoic (p < 0.01) nodules in the B4 group, while mixed solid/cystic nodules (p = 0.01) were more frequent in the B3 group. This is consistent with the fact that follicular lesions are predominantly solid and hyperechoic/isoechoic in echotexture, thus accounting for a greater representation in the B4 group (34). The presence of microcalcifications was greater in the B3 group (30.3% vs. 14.3%; p = 0.02), likely reflecting a greater likelihood of papillary lesions found in B3 compared to B4 (35).
When evaluating for sonographic features predictive of malignancy in the previous study, irregularity of margins in the B3 group was significantly associated with malignancy (p = 0.01) (17). This is in keeping with the 2015 ATA guidelines, which consider irregular margins as a highly suspicious sonographic feature (5).
On the other hand, in the B4 group, it was found that the presence of macrocalcifications was significantly associated with malignancy (p < 0.01). While the association of microcalcifications with malignancy is widely known, that of macrocalcifications is more controversial. Historically, macrocalcifications have generally been considered as an indicator of a benign nodule (36 –38). However, in recent times, more studies have shown that macrocalcifications are not infrequently associated with malignancy. Taki et al. and Kim et al. demonstrated malignancy rates of 43% and 63%, respectively, among thyroid nodules with eggshell calcifications, of which all were PTCs (39,40). In the present study, there were a total of six nodules in the B4 group with macrocalcifications, all of which proved to be malignant: four (66.7%) FTCs, one (16.7%) FVPTC, and one (16.7%) MTC. One of the possible reasons behind the finding of more FTCs could be due the fact that this sample was limited to the B4 category. Furthermore, there is also an increasing literature showing that FTC is an important differential to consider in the setting of a thyroid mass with macrocalcification (41). For example, a recent study by Zhang et al. comparing sonographic features between FTC and follicular adenomas (FA) showed that the presence of macrocalcifications was more common in FTC than in FA (55.6% vs. 7.7%; p < 0.05) (42). The hypothesis behind this observation is that calcifications represent a secondary reaction to tissue necrosis or hemorrhage, which is more common in FTCs (43). With regard to the patterns of calcification, it has been thought that irregularities and interruptions in peripheral calcifications signify malignant invasion, while central calcifications limit assessment of nodules due to posterior acoustic shadowing obscuring possibly malignant features such as solid components or microcalcifications (41,44,45). Both of these were observed in the nodules with macrocalcifications in this study, as shown in Figure 2.
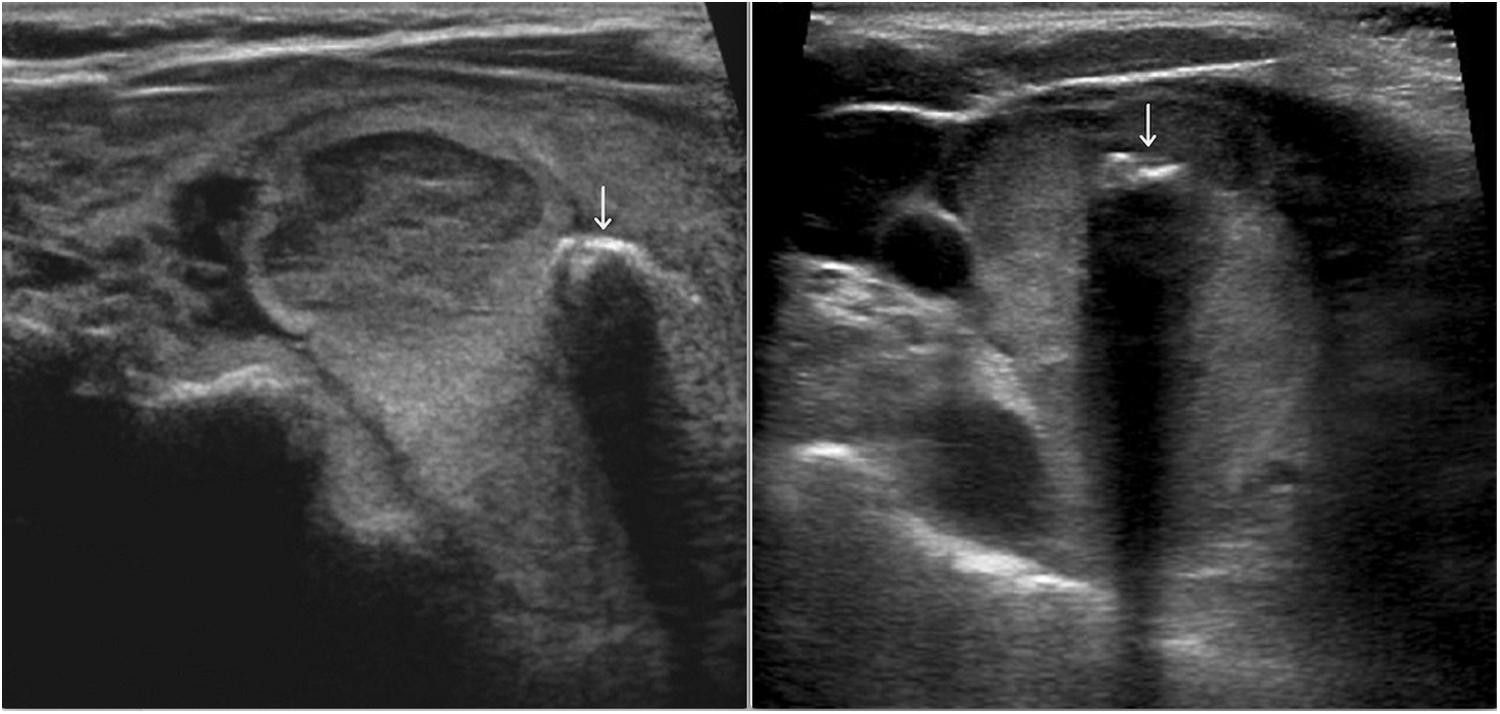
Peripheral macro-calcification demonstrating an irregular and interrupted pattern (left), and central macro-calcification demonstrating posterior acoustic shadowing, obscuring a significant portion of the thyroid nodule (right).
It is prudent to note that heterogeneity remains a significant issue for both the indeterminate categories of B3 and B4, placing doubt on the true malignancy rates of these two categories and hence the rationale of recommending a single course of action within each category. Some of the factors influencing this include inter-observer variability in cytological interpretation and differences in patient populations (46 –51). To control for this heterogeneity better, it may be useful to subclassify indeterminate categories further to delineate the large differential risk of malignancy between FNACs with architectural and nuclear atypia features. The concept of subclassification is not novel and has long been evaluated in the indeterminate categories, especially B3. There is a multitude of studies that have shown significant differential malignancy rates within the B3 group based on subclassification into nuclear and architectural atypia. These rates range from 10% to 33% in nodules with only architectural atypia and from 32% to 76% in those with nuclear atypia (14,16,52 –58).
In contrast to the B3 category, there is a paucity of literature investigating the subclassification of B4. In the pre-Bethesda era, Goldstein et al. found that follicular neoplasms with nuclear atypia had a significantly higher malignancy rate of 44.4% compared to 6.8% in those without nuclear atypia (18). In the post-Bethesda era, Ustun et al. subclassified follicular neoplasms into three categories: (i) microfollicular-patterned neoplasm; (ii) Hürthle cell neoplasm; and (iii) follicular lesion with some features suggestive of but not diagnostic of the follicular variant of papillary thyroid carcinoma. The malignancy rates were 29%, 26%, and 73%, respectively, indicating that follicular neoplasms with even subtle nuclear atypia had a high positive predictive value for malignancy (20).
Currently, the management of indeterminate nodules as recommended by TBSRTC and supported by the 2015 ATA guidelines is clinical correlation and repeat FNAC for B3 (AUS/FLUS) and diagnostic lobectomy for B4 (FN/SFN) (5,6).
In view of the present findings, the subclassification of B3 into architectural atypia and nuclear atypia seems to connote a significant differential malignancy risk (14.7% vs. 36.8%; p < 0.01) that may warrant serious consideration for surgical management for these high-risk B3 nodules, since the malignancy rate exceeds the “intermediate risk” threshold of 15–30% for diagnostic lobectomy as recommended by TBSRTC (6). Furthermore, in the comparative analysis between B3 with nuclear atypia and B4, no significant difference was found between the malignancy rates of the two groups (36.8% vs. 35.2%; p = 0.86). This, however, represents the Western approach whereby a malignancy risk threshold of 15–30% in patients with follicular neoplasms is deemed sufficient for surgery. This is in contrast to the more conservative Japanese perspective. The Japan Thyroid Association (JTA) published new guidelines for the clinical management of thyroid nodules, which included an updated cytological reporting system that recommends subclassification of follicular neoplasms for the purpose of risk stratification. Based on features of cellular atypia, loss of cellular cohesiveness, loss of cellular polarity, and structural abnormalities such as trabecular, tubular, and microfollicular growth pattern, follicular neoplasms are subclassified into three categories: A-1, favor benign; A-2, borderline; and A-3, favor malignant. These categories have recommended risk of malignancy rates of 5–15%, 15–30%, and 40–60%, respectively (59). This subclassification of follicular neoplasms was supported by a follow-up study done by Kakudo et al., which showed a high malignancy rate for A-3 (favor malignant) lesions of 60–75%, with good inter-observer reliability (κ = 0.77). This malignancy rate was significantly higher than that in the other two subcategories of A-1 (favor benign) and A-2 (borderline) of 0–37.5% (p < 0.01; κ < 0.40) (60).
Comparing the subclassification in the present study to that of the JTA's reporting system, the combined results of subclassifying both B3 and B4 nodules actually parallels the JTA classification system, which separates the indeterminate category into (A) follicular neoplasms (follicular-patterned lesions, possibly neoplastic), which have been elaborated above with regards to the three subcategories, and (B) others (all other histological types, excluding follicular neoplasms, which includes cases with equivocal features of PTC, features suggestive of chronic thyroiditis, and malignant lymphoma, or cases with questionable features for C-cell carcinoma, poorly differentiated carcinoma, undifferentiated carcinoma, intrathyroidal epithelial thymoma/carcinoma showing thymus-like differentiation and metastatic carcinoma) (59).
As depicted in Table 4, the follicular lesions with subgroup malignancy rates of 14.7% (B3—FLUS), 21.8% (B4—FN without atypia), and 57.6% (B4—FN with atypia) observed in this study correspond closely to the malignancy rates of the JTA's “follicular neoplasm” subcategories: 5–15% (A-1—favor benign), 15–30% (A-2—borderline), and 40–60% (A-3—favor malignant). The malignancy rate of the B3 (AUS) group was 36.8%, but when including the AUS/FLUS (lymphoid) cases in which all five nodules turned out to be malignant, the malignancy rate rose to 41.9%, demonstrating that the non-follicular lesions were similar to the JTA's “others” group of 40–60%.
JTA, Japan Thyroid Association; NUH, National University Hospital; B3, Bethesda III; B4, Bethesda IV; AUS/FLUS, atypia of undetermined significance/follicular lesion of undetermined significance; FN/SFN, follicular neoplasm/suspicious for follicular neoplasm.
In thyroid cytopathology, risk of malignancy based on cytological classification has become the crux and focus in guiding management. While this approach may be appropriate for benign and malignant diagnoses where cytology alone is accurate enough for a confident diagnosis due to high negative and positive predictive values of 96.3% and 98.6%, respectively (7), the same cannot be said for indeterminate lesions. Currently, the indeterminate categories are identified as “intermediate risk,” but this is based on an average risk of malignancy that is derived from a highly heterogeneous population, as evidenced by studies showing malignancy rates for B3 and B4 ranging from 15.7% to 81% and 11.1% to 65.7%, respectively (10 –13). This study also demonstrated that subclassification within this indeterminate category reveals different subgroups that are unique to each other with regards to malignancy rates, supporting the notion that indeterminate nodules are not well characterized in the current Bethesda classification system. Therefore, using risk of malignancy alone as a guide for the management of indeterminate nodules may not be an appropriate approach considering the wide spectrum in this gray area. Risk stratification within these indeterminate categories is of significant clinical importance and impacts surgical triage. Looking at this issue from an alternate perspective, the average malignancy rates of B3 at 27% and B4 at 31% (31) indicate that approximately 70% of patients in the indeterminate categories are unnecessarily subjected to the morbidities of surgery, highlighting the suboptimal nature of FNAC alone as a triage for definitive surgical diagnosis in this group. As such, the malignancy rate in the indeterminate categories is more of a representation of how well we triage patients for surgery, rather than an “intermediate risk” for cancer. Accordingly, appropriate risk stratification would thus reduce resection rates for benign nodules and increase malignancy rates in resected nodules.
According to the JTA system, further risk stratification is required before selecting surgical candidates, in view of the fact that the internationally reported risk of malignancy for follicular neoplasms overlap with baseline risks both in Western countries (10–20%) as well as in Japan (12.4–15.9%) (61 –66). A retrospective study by Takezawa et al. from Japan analyzed 1606 cytological samples using the Bethesda classification system with 115 (7.9%) cases of B3 (AUS/FLUS) and 61 (4.2%) cases of B4 (FN/SFN). The resection rates of both B3 (30.4%) and B4 (36.0%) nodules were low, but yielded malignancy rates of 88.6% and 72.4%, respectively (67), significantly higher than what is reported in the Bethesda classification (6). This notion that indeterminate FNAC diagnoses need to be further risk stratified is supported by Crippa and Dana, who acknowledge that although FNAC is the most important deciding factor with regards to the management decision, it is not the only important factor and therefore must be integrated with other diagnostic procedures (68) such as ultrasound imaging or molecular methods so as to achieve the best therapeutic decision for the patient.
There are several limitations to this study due to its retrospective nature. First, there is a possibility of selection bias, as only 44.3% of B3 and 79.3% of B4 nodules underwent surgery for final histopathological diagnosis and were included in the risk of malignancy calculation. This can cause an overestimation of the true malignancy rate due to clinical bias. Second, due to the nature of the authors' institution as a cytopathologic tertiary referral center, not all clinical data and histopathological slides could be retrieved, as some patients were treated at other institutions. Lastly, although the study did not formally evaluate for inter- and intra-observer variability in the reporting of FNAC diagnoses, it should be noted that in a real diagnostic cytology and pathology service, inter-observer variability is unavoidable due to the fact that in most laboratories, cases are not reported by a single pathologist but typically by several pathologists. However, in this study, all cytology and histology reports and, where necessary, cytology slides, were reviewed by a single experienced pathologist in order to optimize consistency of subclassification into nuclear versus architectural atypia, as well as the final histologic diagnoses.
In conclusion, the overall malignancy rates of the indeterminate categories in the present cohort were 27.0% for B3 (AUS/FLUS) and 35.2% for B4 (FN/SFN). The only clinically significant predictors of malignancy were suspicious sonographic features: irregularity of margins in B3 and macrocalcifications in B4. Significant differential malignancy rates were observed when subclassifying both B3 and B4 based on the presence of nuclear atypia. Such observations should spur TBSRTC to reevaluate its current categories and place more emphasis on the presence of nuclear atypia in indeterminate nodules.
On the basis of these data, the aims of thyroid nodule management in the indeterminate category should be centered on a risk-stratification approach, taking into account not only TBSRTC classification but also the presence of high-risk cytological features such as nuclear atypia. This, along with the consideration of clinical factors and adjunct investigations, will hopefully lead to better selection of surgical candidates and reduction of non-therapeutic thyroidectomies. Nonetheless, further prospective studies will be required to build on what has been demonstrated so as to answer questions better pertaining to optimal management.
Footnotes
Acknowledgments
We thank Dr. Shen Liang, Senior Biostatistician from the Medicine Dean's Office, National University of Singapore, for her guidance in statistical analysis. We also thank Dr. Tiffany Gan, National University Hospital, for her invaluable work on the B3 group, which formed the foundation of our comparative study.
Author Disclosure Statement
No competing financial interests exist.