
Abstract
Background:
The objective of this study was to determine the effect of a home-based exercise program on fatigue, anxiety, quality of life (QoL), and immune function of thyroid cancer patients taking thyroid hormone replacement after thyroidectomy.
Method:
This quasi-experimental study with a non-equivalent control group included 43 outpatients taking thyroid hormone replacement after thyroidectomy (22 in the experimental group and 21 in the control group). After education about the home-based exercise program, subjects in the experimental group underwent 12 weeks of aerobic, resistance, and flexibility exercise. A comparative analysis was conducted between the two groups.
Results:
Patients in the experimental group were significantly less fatigued or anxious (p < 0.01). They reported significantly improved QoL (p < 0.05) compared to those in the control group. Natural killer cell activity was significantly higher in the exercise group compared to that in the control group (p < 0.05).
Conclusion:
A home-based exercise program is effective in reducing fatigue and anxiety, improving QoL, and increasing immune function in patients taking thyroid hormone replacement after thyroidectomy. Therefore, such a home-based exercise program can be used as an intervention for patients who are taking thyroid hormone replacement after thyroidectomy.
Introduction
C
Thyroid cancer patients who undergo total thyroidectomy must take and maintain high doses of thyroid hormones. Physical and psychological discomfort can lead to increased fatigue (4,6). However, clinical trials tend not to address patient (dis)comfort or psychological well-being when evaluating treatment efficacy.
Interventions designed to manage symptoms in cancer patients have included a variety of therapies. Among these, exercise is the most common intervention. Several studies have reported that exercise can reduce fatigue, anxiety, and fear. It can enhance activities of daily living; improve physical, psychological, and social functions; promote social interaction; and enhance immune response (7 –9).
The objectives of this study were to develop a home-based exercise program and to determine the effect of such a program on fatigue, anxiety, QoL, and immune function of thyroid cancer patients taking thyroid hormone replacement after thyroidectomy. The results of this study will establish an empirical basis for using such an exercise program as an intervention for thyroid cancer patients.
Patients and Methods
Subjects
The data collection period was from October 2015 to March 2016. Subjects were thyroid cancer patients who were taking thyroid hormone medicine after thyroidectomy. All patients provided informed consent after the advantages and disadvantages of each procedure were explained to them. The procedure that the patient would undergo was selected using a random number. A home-based exercise education program was provided to subjects in the study group. They underwent the home exercise intervention for 12 weeks. For subjects in the control group, no intervention was provided for 12 weeks. After 12 weeks, the same home-based exercise education program was provided to subjects in the control group. The same strategy to sustain their home exercise for 12 weeks was also offered.
Inclusion criteria were: (i) diagnosis of thyroid papillary carcinoma; (ii) treatment with thyroid hormone medication after thyroidectomy; (iii) lack of radioactive iodine treatment within the past six months; (iv) blood hemoglobin level >10 g/dL; (v) pain scale score <3 points on a 0–10 numeric rating scale (NRS); (iv) not taking drugs that could affect their immune function (e.g., immunosuppressants such as cyclosporin and steroids); (vii) lack of regular exercise; (viii) age 18–75 years; (ix) comprehension of participation questionnaire and ability to respond to questions in writing or verbally; and (x) provision of written informed consent by the subject or a designate. Exclusion criteria were: (i) abscess or inflammation suspected by preoperative tests; (ii) history of head or neck malignancy; or (iii) radiation therapy.
Sample size
To determine the number of study subjects needed for this study, calculation was performed with statistical power (1-β) of 0.85, level of significance (α) of 0.05, intermediate effect size of 0.25, and correlation coefficient between repeated measures (r) of 0.50 in repeated measures analysis of variance (ANOVA) using G*Power 3.1.7 program. As a result, 19 people were required for each group. Anticipating dropouts, 23 individuals were selected for the experimental group and 23 subjects for the control group. One subject from the experimental group and two subjects from the control group dropped out due to blood contamination during the six-month data-collection period. Therefore, 22 subjects in the experimental group and 21 subjects in the control group were finally analyzed in this study.
Ethical considerations
After obtaining approval (GNUH 2015-06-033-004) from the Gyeongsang National University Hospital Biomedical Research Institutional Review Board, suitable subjects were selected and written informed consent was obtained from each subject. This study was performed following the guidelines of the Declaration of Helsinki.
Research design
As a quasi-experiment research to verify the effect of a home-based exercise program on thyroid cancer patients who underwent thyroidectomy, this research had a nonequivalent control group with pretest–posttest design. A quasi-experiment is an empirical study used to estimate the causal impact of an intervention on its target population without random assignment. Quasi-experimental research shares similarities with traditional experimental design or randomized controlled trials. However, it specifically lacks the element of random assignment to treatment or control. Instead, quasi-experimental design typically allows researchers to control assignment to the treatment condition using a criterion other than random assignment.
Research Tools
A questionnaire consisting of 50 questions (13 questions pertaining to general characteristics and disease-related characteristics for subjects, 9 questions on fatigue, 7 questions on anxiety, and 21 questions for QoL) was used in this study.
Fatigue assessment
To assess fatigue, this study used the Brief Fatigue Inventory (BFI) developed by Mendoza et al. (10). The BFI is a tool for measuring the degree of fatigue and the degree of fatigue disturbance on daily life perceived by subjects. It consists of nine questions evaluated on a scale ranging from 0 (no fatigue) to 10 (fatigue causing severe trouble), with a higher score indicating higher fatigue. To assess fatigue of cancer patients quickly and easily, the BFI is a tool recommended by the Pain Research Group of MD Anderson Cancer Center (Houston, TX). The degree of fatigue was classified based on the average value of nine questions, with 0, 1–3, 4–6, and 7–10 points depicting no fatigue, mild fatigue, severe fatigue, and serious fatigue, respectively.
Anxiety assessment
To assess anxiety, this study used the Hospital Anxiety-Depression Scale-Anxiety (HADS-A) of Hospital Anxiety-Depression Scales (HADS) developed by Zigmond and Snaith (11). This tool consists of seven items on a four-point scale (0–3 points). Its score ranges from 0 to 21 points, with a higher score indicating higher anxiety. The degree of anxiety was classified based on the total score, with 0–7, 8–10, 11–14, and 15–21 points depicting normal range of anxiety, mild anxiety, severe anxiety, and serious anxiety, respectively.
QoL assessment
To assess QoL, this study used the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 (EORTC QLQ-C30). As a tool for assessing health-related QoL of cancer patients, the EORTC QLQ-C30 consists of 30 questions with three subscales: function QoL, symptom QoL, and overall health QoL.
In this study, the symptom QoL subscale was modified for thyroid cancer patients because the original symptom QoL subscale consisted of symptoms that cancer patients would generally experience in the cancer treatment process. However, thyroid cancer patients as subjects of this study did not receive chemotherapy or radiation therapy. Therefore, they did not experience most of the symptoms listed in the original symptom QoL subscale of ECORTC QLQ-C30. Thus, items on pain, insomnia, and appetite loss were used for symptoms based on previous literature on thyroid cancer patients (12).
For functional scales and symptom scales/items, they were evaluated in a four-point scale ranging from 1 (“not at all”) to 4 (“absolutely yes”). Global health status/QoL was evaluated with a seven-point scale ranging from 1 (“very bad”) to 7 (“very good”). Based on the EORTC QLQ-C30 Scoring Manual provided in the Quality of Life Unit of EORTC, QoL scores were converted into scores of 0–100 points by adding the sum of individual items in each subscale, with higher scores indicating a higher degree of QoL.
Development of a home-based exercise program
A home-based exercise program was developed so that it could be applied to thyroid cancer patients. This program was based on the following evidence-based programs: physical self-management rehabilitation program for cancer survivors (13), an exercise and education cancer recovery program (14), 2012 American Cancer Society practice guidelines (15), and 2010 American College of Sports Medicine practice guidelines (16). This study program was modified after it was reviewed by two exercise experts. Their opinions were sought to verify its validity. The home-based exercise program included exercise instructions, a 12-week exercise regimen, and a long-term strategy (Table 1 and Supplementary Data; Supplementary Data are available online at
RPE, ratings of perceived exertion.
The home-based exercise program included home-based exercise as a 12-week program with a long-term strategy for adherence to exercise routine. Training was provided in an outpatient training room for 30–40 minutes. A booklet was provided to participants to explain the necessity and benefits of regular exercise, methods and precautions for aerobic and resistance exercises, and the necessity of flexibility exercises. A video instruction produced with the help of exercise experts was also available (Supplementary Video S1). During training, the concentration of subjects on the program was maintained. Subjects asked questions and received answers appropriately. Thus, a training time of 30–40 minutes was considered appropriate.
Subjects were asked to save the video directly on their cell phone so that they could watch and follow the movements of the exercise expert as required. The video was also considered appropriate because subjects were using the video during the study period. This 12-week home exercise program involved medium-intensity exercises. Subjects were instructed to perform aerobic exercise (walking for 3–5 days a week for at least 150 minutes a week), resistance exercise (upper and lower body exercise, twice a week, more than two sets per time), and flexibility exercise (5 minutes for 12 weeks before and after aerobic and resistance exercises).
Research procedures
Pre-survey
The scope and purpose of this study was fully and clearly explained to participants. Informed written consent was obtained from each participant. Subject characteristics, levels of fatigue, anxiety, and QoL were recorded using the questionnaire. Blood was collected to determine immune function.
Thyroid hormone therapy
Thyroid hormone was prescribed for thyrotropin (TSH) suppression in differentiated thyroid cancer patients. Several studies have suggested that thyroid hormone for TSH suppression can improve clinical outcomes and decrease recurrences in patients with differentiated thyroid cancer (17 –19). According to the Korean Thyroid Association guidelines, the target of TSH suppression is 0.1–0.5 mIU/L in high-risk patients and 0.3–2 mIU/L in low-risk patients (20). The dose of thyroid hormone was adjusted at every visit to obtain the desired TSH target level.
Experimental treatment
After pre-survey, an exercise training and demonstration session was held in the outpatient training room for 30–40 minutes. The session consisted of an explanation of the need for a home-based exercise program and the possible benefits of aerobic exercise (walking) and resistance exercise. Proper walking style was demonstrated. Time and intensity for aerobic exercise and methods for upper- and lower-body resistance exercises were recommended. For resistance exercises, the experimental group was instructed on proper breathing during exercises along with appropriate use of a resistance band and correct exercise motions. These motions were demonstrated by using an instructional video (video clip—Supplementary Video S1) produced with the help of an exercise expert.
The exercise program lasted 12 weeks. Exercise intensity was tiered, including an introductory stage (1–4 weeks) followed by an improvement stage (5–12 weeks). Subjects were asked to walk for the recommended time, perform the required number of resistance exercises, and record their performance in a journal at the end of each exercise. The progress of each subject was monitored through calls and text messaging throughout the 12-week study. Concurrently, participants were encouraged to maintain their exercises. Information was provided for any exercise-related questions.
Post-survey
Questionnaire responses concerning fatigue, anxiety, and QoL were solicited from subjects from experimental and control groups in an outpatient training room setting after the 12-week program. On the same day, subjects visited endocrine and internal medicine clinics to collect blood samples for immune function assays.
Immune function and laboratory test
Natural killer cell activity (NKCA) was determined as the percentage of dead K562 cells after 15 hours at an effector-to-target cell ratio (E:T) of 20 × 105 cells/mL NK cells to 1 × 105 cells/mL target K562 cancer cells. In addition, blood tests including thyroid function tests, lipids, glucose, and protein levels were performed to check thyroid hormone status and compliance with the exercise program.
Data analyses
IBM SPSS for Windows v21.0 (IBM Corp., Armonk, NY) was used for all data analyses. Characteristics of experimental and control groups were analyzed with real numbers, percentages, and mean and standard deviation. Chi-square test, Fisher's exact test, and Student's t-test were used to compare characteristics of experimental and control groups and to determine homogeneity of research variables. Shapiro–Wilk verification was carried out using pretest scores of research variables to verify normality of variables for experimental and control groups. Repeated-measures ANOVA was carried out to verify the effect of research variables on the home-based exercise program. If the interaction between each group and time was significant, a paired t-test was used for comparison between measurement points. The reliability of the measurement tool for fatigue, anxiety, and QoL was measured by Cronbach's alpha. Statistical significance was considered at a p-value of <0.05.
Results
Subject characteristics and homogeneity
Demographic and clinicopathologic characteristics of subjects and homogeneity results of these characteristics in experimental and control groups are summarized in Table 2.
Fisher's exact test.
SD, standard deviation; BMI, body mass index.
Compliance rates by period in the experimental group
The aerobic exercise compliance rate was 73.3% for average walking time per week and 68.7% for average walking minutes per week. The resistance exercise compliance rate was 75.0% for average exercise minutes per week. It was also 75.0% for average exercise set per time (Table 3).
Effect on exercise on fatigue and anxiety
Fatigue levels in subjects in the experimental group were significantly (p = 0.002) reduced from a pre-exercise value of 4.48 points to a post-exercise value of 3.52 points. Corresponding values for the control group were 4.37 points and 5.12 points (p = 0.001), respectively. Anxiety levels in subjects of the experimental group were significantly reduced (pre exercise 13.86 points; post exercise 11.32 points; p < 0.001). Corresponding levels for the control group were 12.43 points and 13.00 points (p = 0.180; Table 4).
Repeated-measures ANOVA for anxiety revealed no significant (p = 0.910) difference in anxiety between the two groups. However, the level of anxiety depending on time (p = 0.001) and interaction between time and group (p < 0.001) were significant, with anxiety in the experimental group being significantly lower than that in the control group over time.
Effect of exercise on QoL
QoL functional scales in the experimental group were increased significantly (p < 0.001) from 70.51 points before exercise to 82.73 points after exercise. Corresponding values for the control group indicated a decrease (71.85 points to 69.10 points), although the decrease was not statistically significant (p = 0.063). Symptom scales/items in the experimental group were increased significantly (p = 0.011) from 78.03 points before exercise to 84.85 points after exercise. However, the control group displayed a significant decrease from 75.00 points to 67.46 points (p = 0.024). Overall health QoL (global health status/QoL) of the experimental group was increased significantly from 55.30 points before exercise to 72.35 points after exercise (p < 0.001). However, it was decreased in the control group (from 56.35 points to 52.38 points), although the decrease was not statistically significant (p = 0.227; Table 5 and Fig. 1).
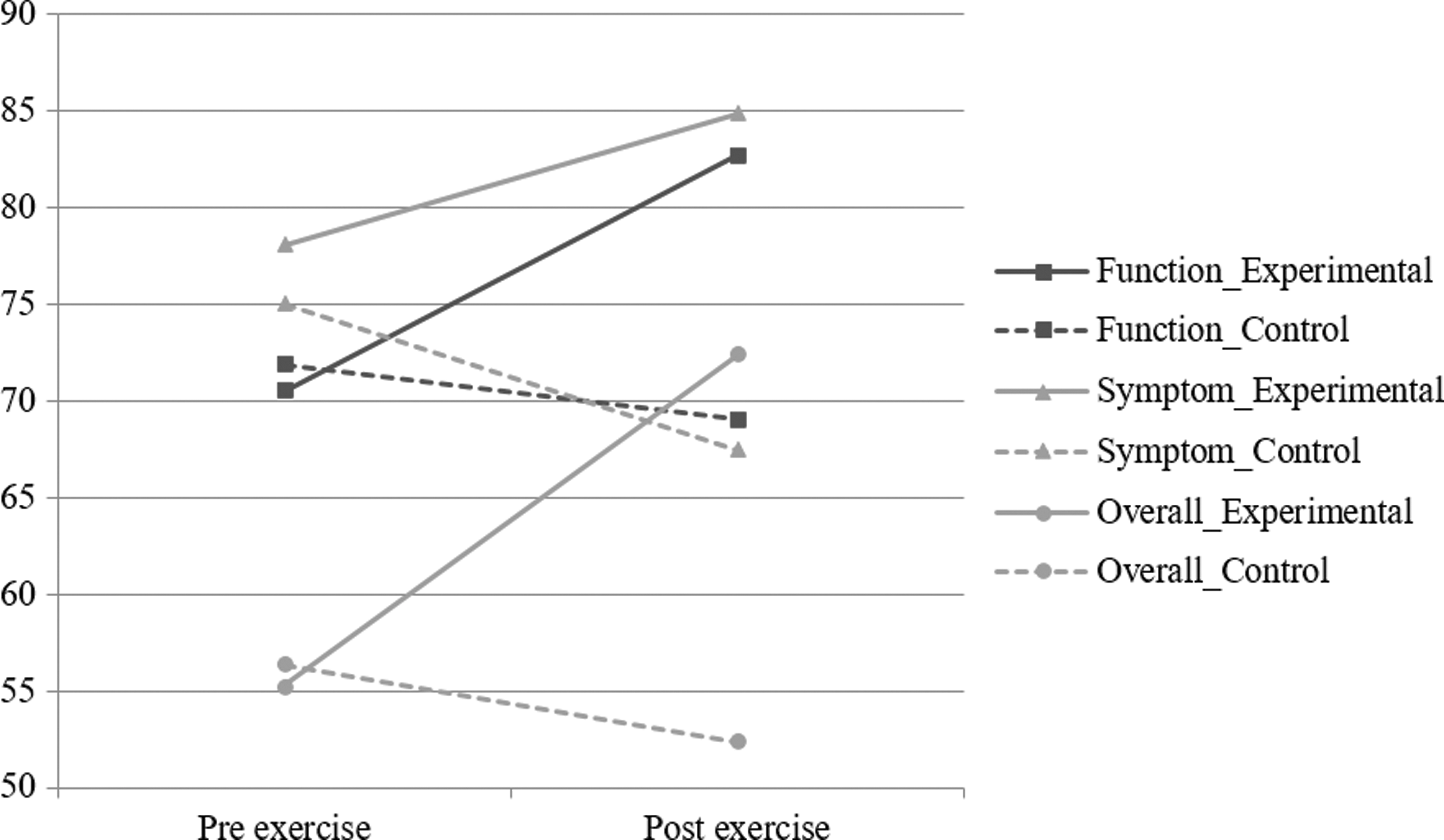
Changes in quality of life by period in the experimental group and the control group.
Effect of exercise on NKCA
NKCA cytotoxicity in the experimental group was increased significantly (p = 0.041) from 11.09% before exercise to 14.46% after exercise. It was decreased from 14.50% to 13.14% in the control group, although the decrease was not statistically significant (p = 0.543). NK cell levels in the experimental group were increased from 10.93 × 109/L before exercise to 12.65 × 109/L after exercise. They were decreased from 11.76 × 109/l to 11.36 × 109/L in the control group. However, differences between these two groups were not statistically significant (Table 6).
NKCA, natural killer cell activity; NKCC, natural killer cell count.
Effect of exercise on other hematological factors
Hematologic analyses revealed significant increases of triiodothyronine (T3) and albumin levels in the experimental group (p < 0.05). TSH levels decreased, while free thyroxine (fT4) levels were increased in the experimental group. However, these changes were not statistically significant. In the control group, TSH levels increased, while fT4 and T3 levels decreased, although these changes were not statistically significant. However, the control group displayed a significant increase in cholesterol, triglycerides (TG), high-density lipoprotein (HDL), and low-denisty lipoprotein (LDL) cholesterol levels (p < 0.05; Table 7).
TSH, thyrotropin; T4, thyroxine; T3, triiodothyronine; Thyro Ag, thyroglobulin antigen; Thyro Ab, thyroglobulin antibody; TG, triglyceride; HDL, high-density lipoprotein; LDL, low-density lipoprotein.
Discussion
Many cancer patients experience anxiety and fatigue due to the uncertainty about their future health. They have a feeling of helplessness in coping with their cancer (21). They also have fear of recurrence (22). Despite the thyroid surgeries which have been developed (23 –27), and the often-good prognosis of thyroid cancer, many patients experience psychological distress that can be heightened by blood testing every three to four months, secondary effects of surgery and/or radioactive iodine treatment, and treatment with supra-physiologic doses of thyroid hormones (28). The latter can result in subclinical hyperthyroidism, which can produce fatigue (4,29 –31). Thyroid cancer patients can experience severe fatigue, with significantly higher prevalence than present in the general population (10,32). These results suggest the need for an intervention to alleviate anxiety and fatigue of thyroid cancer patients.
Previous studies have described exercise training programs for cancer patients (13,14). Exercise is recommended in the guidelines of the American Cancer Society (15) and the American College of Sports Medicine (16). Some previous studies have designed and studied the impact of exercise on thyroid cancer patients and measured the same variables used in this study (33 –37). The first randomized controlled trial of an exercise intervention in thyroid cancer survivors was published by Vigário et al. (36,37). An additional observational study has been published, supporting this study's general conclusion (33). In addition, systemic reviews and meta-analyses have been performed to determine the role of exercise in the management of fatigue and improvement of QoL of cancer survivors (34,35). These previously published trials have reported the benefit of supervised exercise for reducing fatigue and improving QoL. This prompted the present study to gauge the effect of a home-based exercise program for thyroid cancer patients and to verify its effect on fatigue, anxiety, QoL, and immune function of these cancer patients who underwent thyroidectomy. An important difference between previous trials and the present study is that the exercise intervention used in previously published trials was a supervised exercise program, whereas a home-based program was used in the present study.
The fatigue of subjects in the experimental group who engaged in the home-based exercise program was significantly reduced compared to that in the control group. The reduction in fatigue in the experimental group might be due to increased activity. In fact, secondary fatigue due to decreased activity has been reported to be a cause of fatigue in cancer patients, while regular exercise can decrease their fatigue level (38). In addition, subjects in the experimental group reported that their stress level reduced, indicating a reduction in emotional discomfort (38). A significant increase in fatigue in the control group is considered to be due to the vicious cycle described by the psychobiological entropy model, in which decreased activity from thyroid medication-related fatigue can cause structural and biochemical changes in the body, which further deplete the body's energy, leading to secondary fatigue as energy is diminished (3).
Those engaged in the home-based exercise program experienced decreased anxiety, while those in the control group displayed increased anxiety. Exercise-related improvement in physical conditioning might have lessened the feeling of helplessness regarding the threat of recurrence and instilled more optimism concerning their future. Exercise also leads to increased secretion of neurotransmitters such as dopamine and serotonin to help maintain the body's homeostasis and boost vitality by affecting mood changes (39,40). Subjects in the experimental group opined that regular exercise made them feel healthier and instilled a sense of pride in their self-management of their health. This is consistent with a prior report showing that exercise-related psychological distress is diminished in thyroid cancer patients during treatment follow-up (6).
Symptom scales/items and global health status/QoL of subjects in the experimental group with the home-based exercise program were increased, while these were decreased in the control group. The improved QoL in subjects participating in the exercise program might have reflected the decrease in fatigue and anxiety as the two important influential factors of QoL of thyroid cancer patients (6). These decreases might be due to an exercise-related increase in the secretion of dopamine and serotonin (39,40). Subjects in the experimental group also reported that they felt less tired and had an increased level of vitality. The increasingly positive attitude with their day-to-day living might have been reflected as improved QoL.
NKCA levels in the experimental and control group were increased and decreased, respectively. However, there were no significant differences in numbers of NK cells between the two groups. The exercise-related increase in NK activity in the experimental group in this study might have enhanced immune function due to improved endocrine activity (41) and changes in sympathetic nervous system activity (42). NK cells are important in mediating surveillance for cancer cells. They participate in cell death. NKCA is a clinically useful indicator of immune health, as NK activity impacts the prognosis of patients with cancer (43).
Regarding the effect of exercise on hematological features, the control group showed increases in cholesterol, TG, HDL, and LDL levels. The increase of these parameters in the control group reflect the lack of exercise. This also strongly suggests compliance with the exercise program in the experimental group.
In the experimental group, T3 and albumin levels were increased. Thyroid hormone substitution used in this study was based on the researcher's empirical experience and rule of thumb. Thus, the prescription of the thyroid hormone dose might be subject to some bias. It might affect thyroid function tests and QoL of subjects in both the experimental group and the control group. However, there was no significant difference in body weight or thyroid hormone supplementation between these two groups. No difference in weight-adjusted thyroid hormone dose was found either. The significantly higher T3 level in the experimental group might be due to exercise because patients in both groups underwent thyroidectomy. Exercise might affect thyroid hormone concentrations due to an impact on peripheral conversion. Some studies have reported a reduction in reverse T3 and an increase in T3 after acute exercise in untrained subjects. However, thyroid hormone metabolism during strenuous exercise in young adults has shown controversial results (44 –47). In addition, no study has reported changes in thyroid hormone levels after exercise in thyroidectomized patients. Thus, the observed effect on T3 levels in thyroidectomized subjects will require further studies.
The home-based exercise program was effective in reducing fatigue and anxiety. It also increased QoL and immune function. Data validation is needed in the future by including the use of this exercise program in patients without contraindication to exercise soon after thyroidectomy. Efforts to maximize compliance and maintenance of the program are also needed in the future by incorporating monitoring equipment such as pedometers, smart bands, and software applications.
Based on self-reporting results, the degree of exercise compliance of subjects for this study involved performing aerobic exercises at an average of 120 minutes a week, resistance exercises at an average of twice a week with four sets, and flexibility exercises totaling 10 minutes before and after resistance exercise. Aerobic exercises were performed for slightly less time than recommended. In the future, subjects should be provided with devices such as a pedometer as an incentive to attain the full recommended times and to increase exercise adherence. Based on information from calls during the home-based exercise training and experiment periods, most subjects only performed aerobic exercises, thinking that flexibility exercises were unnecessary or inconvenient for aerobic exercises (walking), despite the fact that flexibility exercises were advocated as being important. In the future, an effective program to emphasize the need for flexibility exercises further should be considered.
To establish a home-based exercise program into a long-term strategy, patients were asked to keep a journal. They received reminders via text messages and weekly phone calls during the 12-week exercise period. Through this regular contact, the degree of exercise compliance and performance of these subjects was checked, and information on any exercise-related questions was provided. The enrolled subjects expressed that they were encouraged to exercise and felt a sense of belonging. Although they exercised at home by themselves, these patients felt that they were being cared for.
In conclusion, a home-based exercise program was effective in reducing fatigue, diminishing daily anxiety, improving QoL, and enhancing immune function in patients receiving thyroid hormone substitution after thyroidectomy. These findings support the use of exercise for patients undergoing therapy for thyroid cancer.
Footnotes
Author Disclosure Statement
No financial or material support has been received for this work. The authors declare no financial interests in companies or other entities that could have an interest in information provided in this study.