
Abstract
Background:
Patients with anaplastic thyroid cancer (ATC) have a dismal prognosis, despite systemic cytotoxic chemotherapy. The objective of this study was to investigate the efficacy and safety of targeted therapy in ATC patients when used outside of a clinical trial.
Methods:
This is a retrospective review from April 2015 to May 2016 at a single academic institution where 16 ATC patients receiving targeted therapy outside of a clinical trial were studied. Ten patients (eight BRAF wild type and two BRAFV600E mutant tumors) were started on lenvatinib, and six with BRAFV600E -mutated tumors received a combination of dabrafenib plus trametinib. Best response evaluated by RECIST v1.1, progression-free survival, and overall survival were determined. Adverse events were evaluated for safety.
Results:
The majority of patients (63%) were men, and all had distant metastases or radiation-resistant primary disease at the time of treatment. In the entire cohort, 6/16 (38%) had a partial response, 6/16 (38%) had stable disease, and 2/16 (12%) had progressive disease. Two (12%) patients died before restaging. Median follow-up time was 11.8 months. Median progression-free survival was 3.7 months [confidence interval 1.8–7.6] in the entire cohort, 2.7 months for lenvatinib, and 5.2 months for dabrafenib plus trametinib. Median OS was 6.3 months [confidence interval 1.8–7.6] for the entire cohort, 3.9 months for lenvatinib, and 9.3 months for dabrafenib plus trametinib. Adverse events were as expected and manageable.
Conclusions:
Targeted therapies, lenvatinib, and dabrafenib plus trametinib (for BRAFV600E mutants) may provide clinical benefit in ATC patients who are unable to participate in clinical trials, and toxicities are manageable.
Introduction
A
Recently, several driver mutations have been identified in ATC and have led to a better understanding of this heterogeneous disease (2,4). As in differentiated thyroid cancers (DTC), BRAF and RAS mutations represent early mutational events in ATC, and are present in 25% and 28% of cases, respectively (5). This suggests that ATC is often derived from well-differentiated thyroid cancers. Late events such as TERT promoter and PIK3CA and TP53 mutations often co-exist with the early event mutations. TP53 mutations are the most common alterations found in ATC and are present in 73% of cases (5).
The response rate to cytotoxic chemotherapy is 15–25%, but these responses are short-lived (6 –10). The largest clinical trial in ATC to date studied cytotoxic chemotherapy plus fosbretabulin (a vascular disrupting agent) versus cytotoxic chemotherapy alone (control arm), and showed a median OS of 5.2 versus 4 months, respectively (10). This trial closed early due to slow accrual, in part due to strict inclusion criteria. Disappointingly, previous studies with targeted therapies, specifically sorafenib and pazopanib, have shown an OS of 3.9 and 3.6 months, respectively (11,12). However, some of the newer targeted therapies have shown promising results in the treatment of ATC (13 –15). Unlike DTC, there are no Food and Drug Administration (FDA)-approved targeted therapies for the treatment of ATC in the United States. However, one kinase inhibitor, lenvatinib, is approved in Japan. Lenvatinib is a multikinase inhibitor targeting VEGFR1-3, FGFR 1-4, PDGFR-α, RET, and c-kit. The Phase 2 trial using single-agent lenvatinib included 17 ATC patients and led to the approval of this drug in Japan (15). Lenvatinib is currently being studied in clinical trials in the ATC population (NCT02657369). Selective BRAF inhibitors (e.g., dabrafenib and vemurafenib), alone or in combination with a MEK inhibitor (e.g., trametinib and cobimetinib), have also shown promise in BRAF mutant ATC (5,15 –18). Recently, a basket trial with the combination of dabrafenib and trametinib was reported, and showed significant clinical benefit in ATC patients (14). However, most ATC patients do not qualify for investigational studies due to stringent eligibility criteria or are unable to participate due to these trials not being offered near their homes. Thus, the goal of this study was to investigate the efficacy and tolerability of targeted therapies in ATC patients who were treated outside of the context of a clinical trial, particularly because clinical trial results often are not generalizable to the broader population.
Materials and Methods
Study population
Under an Institutional Review Board approved protocol, the ATC database was queried for patients who were initiated on molecularly targeted therapy at The University of Texas MD Anderson Cancer Center over a one-year period (April 2015–May 2016). Patients who were treated in a clinical trial and who received targeted therapy outside the institution were excluded. All pathologic diagnoses of ATC were confirmed by a dedicated head and neck pathologist at The University of Texas MD Anderson Cancer Center.
Evaluations and definitions
The objective of this study was to describe the efficacy and tolerability of targeted therapy in ATC patients. Efficacy of targeted therapy was based on best overall response (BOR) by Response Evaluation Criteria in Solid Tumors version 1.1 (RECIST v1.1) (19), progression-free survival (PFS), and OS. Responses were defined as follows: progressive disease (PD), ≥20% increase in the sum of target lesions size or new metastatic lesion; stable disease (SD), any change in the sum of target lesions size between a 19% increase and a 29% decrease; and partial response (PR), ≥30% decrease in the sum of target lesions size. Clinical benefit was defined as SD plus PR. PFS was defined as the time elapsed between initiation of the targeted therapy and progression or death due to any reason, whichever occurred first. OS was defined as the time elapsed between initiation of the targeted therapy and death. Duration of clinical benefit was defined as the time from the first date the response (PR/SD) was observed to the date of progression. A single radiologist reviewed all cross-sectional images obtained at baseline and during treatment with targeted therapy. Patients who were lost to follow-up were excluded. Patients who did not have restaging scans were excluded from BOR analysis but were included in the survival analysis. Adverse events (AEs) were evaluated using Common Terminology Criteria for Adverse Events version 4.0 (CTCAE v.4.0) (20). The aforementioned evaluation was limited to the first-line targeted therapy.
Statistical analysis
The BOR for individual patients was calculated as percent change in the target lesions from baseline and depicted graphically as a waterfall plot. Kaplan–Meier curves were used to describe median OS and median PFS. Descriptive statistics were used to summarize patient characteristics and AEs. Statistical analyses were performed using Spotfire S + 8.2 for Windows (TIBCO Software, Inc.).
Results
Study population
Thirty-six new or actively followed ATC patients were identified from the institutional database during the study period. Of these, 24 (49%) ATC patients were initiated on targeted therapy, of whom seven (29%) patients were excluded from the analyses because they were treated in a clinical trial. Thus, 17/24 (71%) received targeted therapy outside of the context of a clinical trial. One patient was excluded due to being treated at an outside institution and not being followed up at the authors' institution, yielding 16 evaluable patients. The baseline characteristics of the patients are summarized in Table 1. Of the 16 patients, 10 (63%) were men. At the time of diagnosis, 4/16 (25%) patients were stage IVB, and 12/16 (75%) were stage IVC. Two patients with stage IVB had progression of their locoregional disease, despite high-dose external beam radiotherapy (EBRT) to the neck. Two of the stage IVB patients, treated previously with radiotherapy, developed distant metastases prior to starting targeted therapy. The site of metastases at start of targeted therapy included the lungs in all patients with stage IVC disease. Of these, one also had a metastasis to the rib and one to the pericardium. All patients' tumor tissues were submitted to mutational analysis using a next-generation sequencing (NGS) approach covering a 50-gene panel. Eight of the analyzed tumors harbored a BRAFV600E mutation. Of the 16 patients, eight had a mixed histology (ATC plus papillary thyroid cancer), and six of these eight (75%) patients whose tumors had mixed histology bore a BRAF mutation.
One patient did not have his performance status documented in the chart.
PTC, papillary thyroid cancer; ATC, anaplastic thyroid cancer.
Of the 16 patients, 13 (81%) had received prior treatment for ATC. Of these, eight (50%) patients underwent surgery, seven (44%) patients received EBRT with or without radiosensitizing chemotherapy, and nine (60%) patients received systemic cytotoxic chemotherapy prior to initiating targeted therapy. Of the nine patients who were exposed to chemotherapy, six received it as a “bridging” therapy. Bridging chemotherapy, defined as chemotherapy used to bridge patients to targeted therapy, was necessary due to the potentially long wait for patients to be approved for targeted therapy and to receive drug(s). The time on bridging chemotherapy ranged from one to eight weeks. Bridging chemotherapy with weekly nab-paclitaxel, until the targeted therapy is procured, is part of the standard of care for ATC patients at the authors' center. None of the patients receiving bridging chemotherapy clinically progressed while awaiting targeted therapy. Details of the individual patients' tumor genomics, as well as the treatment modalities received, are described in Supplementary Figure S1 and Supplementary Table S1, respectively.
Three patients presented with stridor at the time of treatment with targeted therapy. One patient had severe dysphagia from esophageal stricture due to previous radiation and locally advanced disease, requiring a percutaneous endoscopic gastrostomy tube for maintaining nutrition and hydration. She did not qualify for a trial due to her inability to swallow pills. Emergency use Investigational New Drug (IND) for dabrafenib and trametinib suspension was granted by the FDA for this patient. The details of this patient's case have been previously published (6). One patient presented with stridor and declined tracheostomy to preserve quality of life. Considering his symptoms, he received bridging chemotherapy with carboplatin and nab-paclitaxel to palliate his symptoms prior to starting lenvatinib.
End organ dysfunction was present in four (27%) patients: three had congestive heart failure (CHF), and one had grade 3b chronic kidney disease. One patient had a prolonged QTc interval, despite several treatments to try to correct this abnormality. Two patients had prior malignancies: gastric carcinoma and carcinoma of the ampulla in one patient, and lung cancer in another. The presence of these comorbidities disqualified them from participating in the clinical trials that were open at that time. Further details regarding comorbidities can be found in Table 1.
Targeted therapy
Median time from diagnosis of ATC to the start of targeted therapy was 3.4 months [confidence interval (CI) 1.4–8.5 months], during which time most of these patients were on other therapies for ATC (Supplementary Table S1). Six patients with BRAFV600E -mutated ATC were treated with a combination of dabrafenib and trametinib. Due to pre-existing history of CHF with an ejection fraction of 40%, one patient on dabrafenib and trametinib was started on 75 mg of dabrafenib b.i.d. (half dose) with 2 mg of trametinib daily. All other patients were started on a full dose of dabrafenib (150 mg b.i.d.) and trametinib (2 mg daily).
Ten patients were started on lenvatinib. Two of these patients had BRAFV600E -mutated tumors. Of these patients, one opted for lenvatinib, while the other patient could not be started on dabrafenib and trametinib due to insurance denial. Five patients were started on the full dose of lenvatinib (24 mg daily). Four patients on lenvatinib were started on a lower dose, which was gradually increased to the full dose, due to concerns for bleeding and/or fistula. One patient discontinued lenvatinib after six days of therapy due to inability to tolerate the adverse events. Median time on therapy was five months [CI 2.8, not reached (NR)].
Efficacy of targeted therapy
Of the 16 patients, 14 were evaluable for best response; the other two patients died prior to the first restaging scan due to progression. In the entire cohort, 6/16 (38%) had partial response, 6/16 (38%) had stable disease, and 2/16 (12%) had progressive disease. The BOR is shown in the waterfall plot in Figure 1. PR were observed in 3/6 (50%) patients on dabrafenib plus trametinib, and in 3/10 (30%) on lenvatinib. Median time to partial response was 12 weeks (range 3–20 weeks). SD was the BOR in 2/6 (33%) patients on dabrafenib plus trametinib, and in 4/10 (40%) patients on lenvatinib. All patients with SD had tumor regression. Overall, clinical benefit (PR + SD) was seen in 75% of patients. Median duration of clinical benefit was 8.3 weeks (range 1.5–34.5 weeks). Of the 16 patients, two (13%) had disease progression as the BOR: one was on full-dose lenvatinib, and one was on full-dose dabrafenib and trametinib. Both patients progressed within two months of starting their respective targeted therapies. The patient who progressed on dabrafenib plus trametinib was confirmed to have a BRAFV600E mutation on NGS of his previously resected tumor nine months prior to initiation of targeted therapy. Interestingly, on cell-free DNA (cfDNA) analysis from plasma, drawn at the time of locoregional recurrence, this patient was not found to have a BRAF mutation, suggesting that the recurrent tumor may not have responded to BRAF directed therapy because of the emergence of a clone lacking the BRAF mutation.
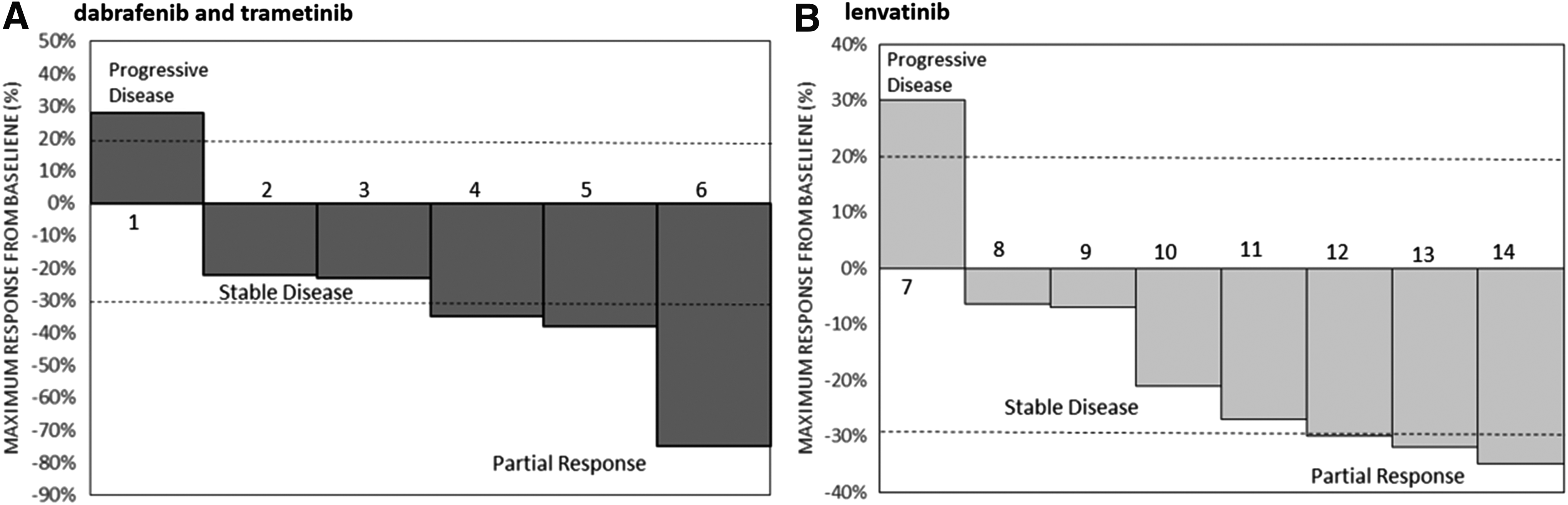
Response to targeted therapy with dabrafenib plus trametinib or single-agent lenvatinib. Waterfall plot of 14 evaluable patients. Of 16 patients, six (38%) had a partial response (PR). Stable disease (SD) was observed in 6/16 (38%) patients, and progressive disease (PD) in 2/16 (13%) patients. Two (13%) patients are not shown in this plot, as they were not restaged. (
The timeline of events for each patient from the initiation of targeted therapy to the date of treatment discontinuation and/or last follow-up are described in Figure 2.
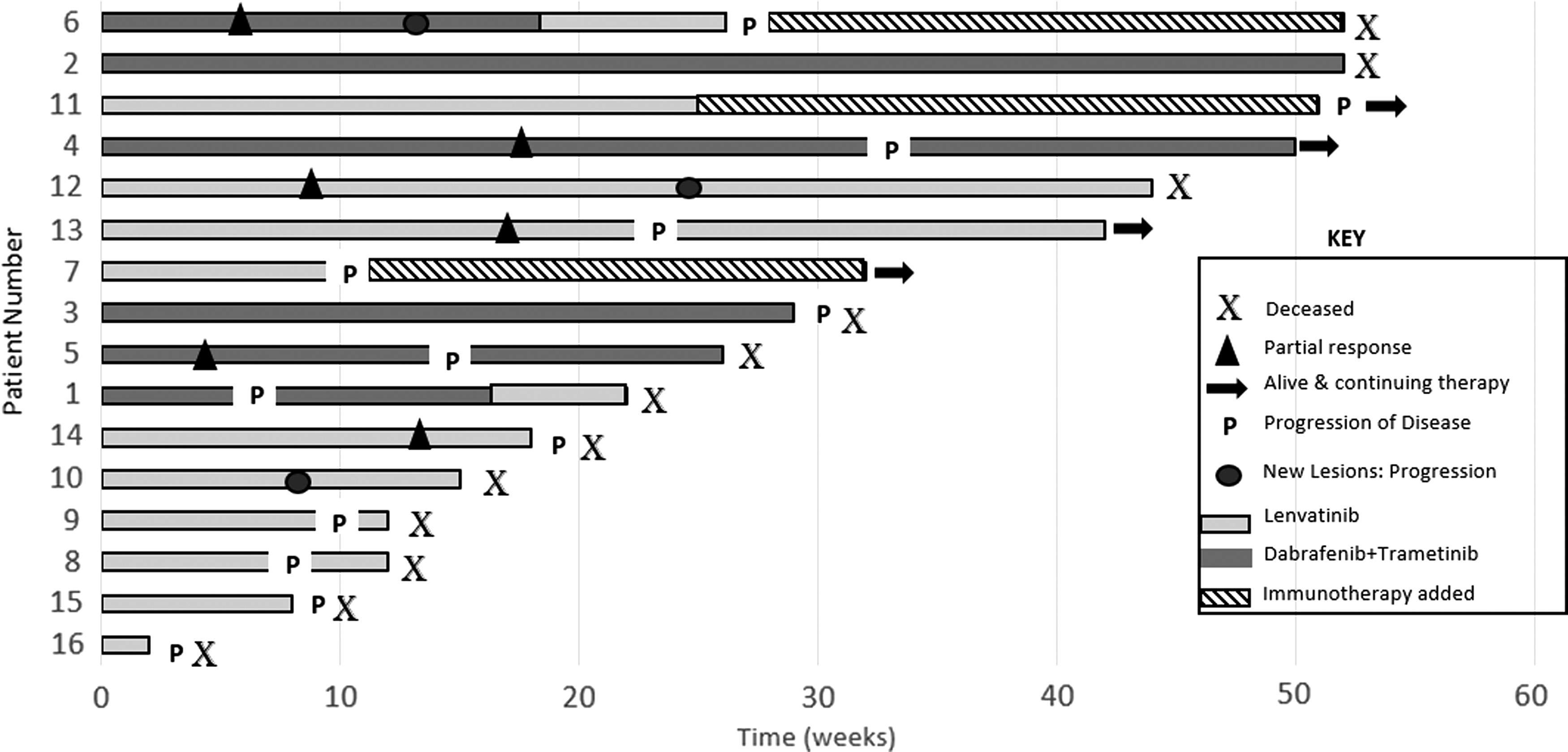
Timeline of events on targeted therapy: The graph depicts the events from the initiation of targeted therapy to the date of last follow-up or death. Patients are numbered according to the BOR, as shown in Figure 1. Patients 15 and 16 died prior to restaging and hence are not depicted in Figure 1. All patients are depicted here in decreasing order of time on targeted therapy. Six patients showed a partial response (depicted by black triangles). Patients 1 and 6 were switched to lenvatinib after they progressed on dabrafenib and trametinib. Three patients progressed on therapy, as evidenced by the development of new lesions (depicted by black circles). Three patients were started on immunotherapy with pembrolizumab, added to their existing targeted therapy. Two of these patients (patients 6 and 12) had shown a partial response prior to the development of new lesions. Patients who died due to progression of disease are depicted by “
Survival analysis
On targeted therapy, PFS and OS were calculated for all 16 patients. The median PFS was 3.7 months ([CI 1.8–7.6]; Fig. 3A). Median PFS for patients treated with dabrafenib plus trametinib was 5.2 months [CI 3.7–NR], and for lenvatinib-treated patients it was 2.6 months ([CI 1.8–NR]; Fig. 3B).
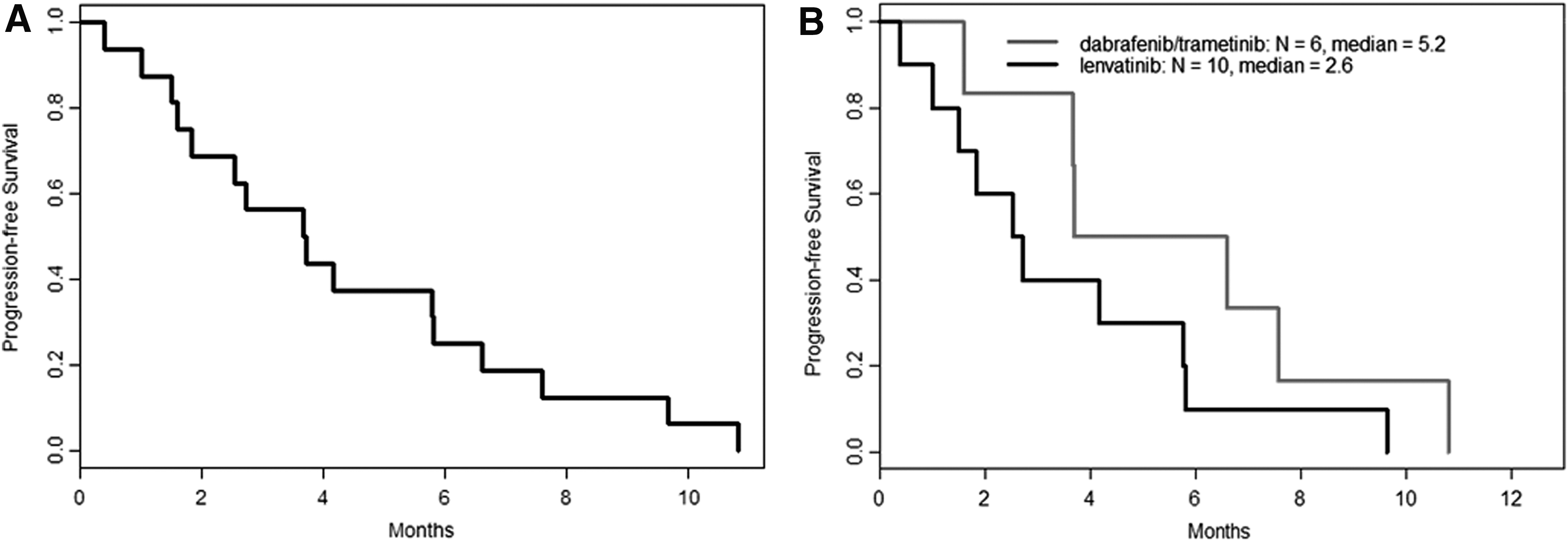
Progression-free survival (PFS) in anaplastic thyroid cancer (ATC) patients treated with targeted therapies. (
After a median follow-up of 11.8 months, four (25%) patients were alive. Median OS was 6.3 months [CI 1.8–7.6] for the entire cohort (Fig. 4A). The median OS was 9.3 months [CI 5.7–NR] for patients treated with dabrafenib plus trametinib and 3.9 months [CI 2.5–NR] for lenvatinib-treated patients (Fig. 4B).
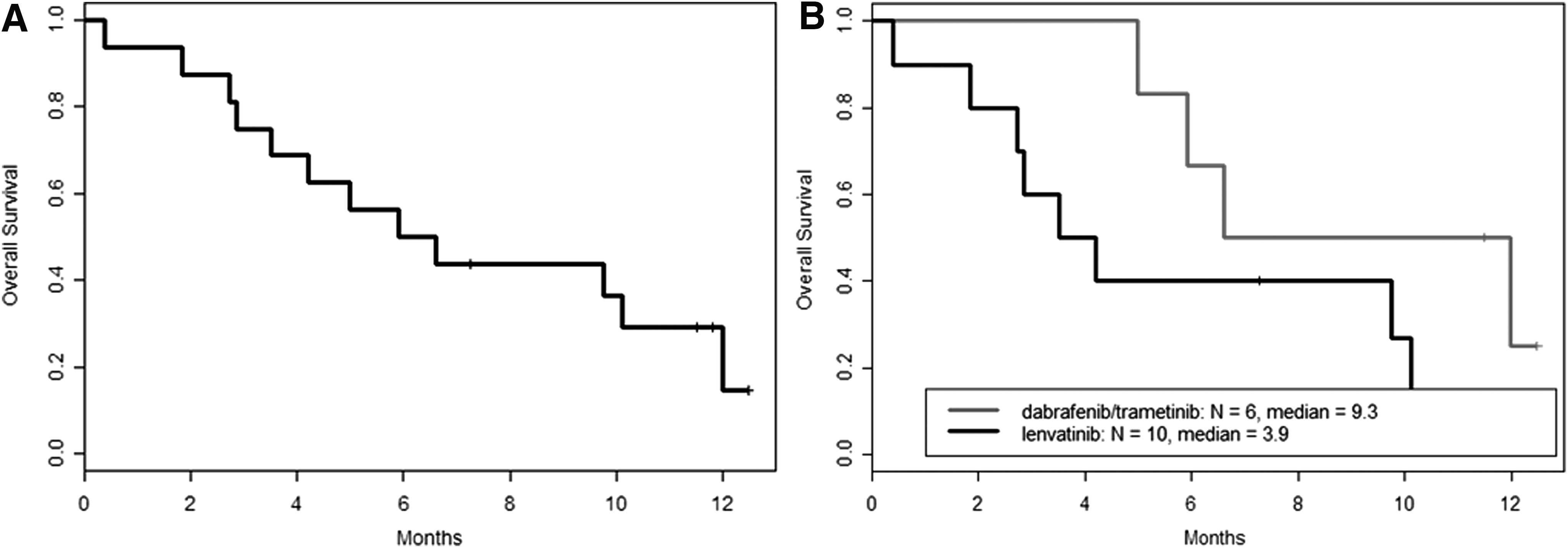
Overall survival (OS) on targeted therapy. (
Safety and tolerability
AEs were as expected and tolerable. One patient had not followed up since starting lenvatinib and hence was excluded from AE analysis due to missing information. All AEs reported are described in Table 2.
Adverse events reported in all 16 patients are listed.
Len, lenvatinib; D + T, dabrafenib plus trametinib; SCC, squamous cell carcinoma
In patients who received dabrafenib plus trametinib, nausea in 4/6 (67%), fatigue in 4/6 (67%), hand–foot skin reaction in 3/6 (50%), hyponatremia in 3/6 (50%), anemia in 3/6 (50%), and weight loss in 3/6 (50%) patients were the most commonly encountered AEs. No grade 4 or higher AEs were noted. One patient had grade 3 anemia requiring blood transfusion, and one with a history of chronic hyponatremia at baseline demonstrated worsening hyponatremia. Other biochemical abnormalities included hypercalcemia, transaminitis, elevated alkaline phosphatase, and lymphopenia.
Dose reduction was needed in two patients on dabrafenib and trametinib who developed lower extremity edema. One of them had CHF at baseline, with an ejection fraction (EF) of 40%. However, this patient did not have a significant change in the EF after treatment and therefore the edema was not attributed to CHF. The other patients with edema had a normal echocardiogram. Only one patient developed grade 1 fever on dabrafenib plus trametinib, which was attributed to drug therapy. Hypothyroidism was seen in two patients.
The most common AEs with lenvatinib were hypertension in 7/10 (70%), pain in 7/10 (70%), fatigue in 7/10 (70%), mucositis in 5/10 (50%), and hand–foot skin reaction in 3/10 (30%) patients. Four (40%) patients who had not undergone thyroidectomy developed grade 1 hypothyroidism. One patient developed grade 3 hyponatremia during treatment, but he also had hypothyroidism requiring an increase in his levothyroxine dose. Among the biochemical abnormalities, hyponatremia was most commonly encountered followed by proteinuria, transaminitis, elevated alkaline phosphatase, lymphopenia, hyperkalemia, thrombocytopenia, hyperuricemia, and anemia. One patient had hemoptysis followed by the development of a broncho-tumoral fistula while on lenvatinib, following which lenvatinib was discontinued. However, prior to this event, there was progression of disease. Thus, it was unclear if this event was attributable to lenvatinib. One patient discontinued therapy after six days due to grade 3 mucositis and grade 3 fatigue. One patient on lenvatinib experienced no clinical or biochemical AEs from lenvatinib. Interestingly, this patient's BOR was PD.
Discussion
A series of 16 ATC patients is described, who were treated outside of the context of a clinical trial with either the combination of dabrafenib plus trametinib or single-agent lenvatinib. Seventy-one percent of patients did not qualify for a clinical trial. This study shows that despite advanced disease and comorbidities that would have excluded patients from a clinical trial, these patients showed relevant responses to therapy, with 83% of patients treated with dabrafenib plus trametinib and 70% of patients treated with lenvatinib experiencing overall clinical benefit—a significant finding for patients with a highly aggressive cancer.
Comparatively, in the Phase II data from a trial with 17 patients treated with lenvatinib, a confirmed PR rate of 24% (4/17) was observed, with the majority of patients experiencing SD, mostly with regression of disease (15). These findings are consistent with the current observations. In the present series, patients treated with lenvatinib had a short median PFS and OS of 2.5 and 3.9 months, respectively. Tahara et al. reported a median PFS and OS of 7.4 and 10.6 months, respectively (15) with single-agent lenvatinib, which is significantly longer when compared to the findings in the present series. A shorter PFS and OS in the current series could be explained by different patient characteristics. Essentially, patients with excellent performance status and in fairly good health are usually enrolled in clinical trials, whereas almost all of the patients in this study had significant comorbidities that would have excluded them from participation in clinical studies.
Recently, results of a basket trial with 16 ATC patients treated with the combination of dabrafenib and trametinib were reported (14). More than 80% of the patients in this trial had received prior treatment with surgery and radiation therapy prior to starting targeted therapy. The response rate was 69%, with one patient experiencing a complete response (CR), 10 patients PR, three patients SD, and one patient PD (14). The median OS and PFS were not reached, but at one year, 80% of patients were still alive. In our series of six patients treated with dabrafenib plus trametinib, 50% of patients had prior treatment with surgery, and 33% of patients had been treated with radiation therapy. Half of the patients experienced a PR, and the median PFS and OS were 3.7 and 9.3 months, respectively. Compared to the OS of the patients treated with lenvatinib, this long OS could be attributed to the targeted treatment of tumors harboring an actionable mutation (BRAF), the ability to salvage those patients with lenvatinib (as was done in two cases), or a more indolent course of disease in these patients compared to non-BRAF-mutated tumors. The strikingly shorter PFS and OS in the patients treated outside of a trial likely reflects the fact that the patients had a worse performance status, comorbidities that excluded them from trial participation, and likely more advanced locoregional disease at the start of targeted therapy. In the basket trial, patients had to be able to swallow pills, suggesting that they possibly had less advanced locoregional disease. This brings to light a serious problem with clinical trials: they may not be generalizable because they include very select patients. Thus, entry criteria in ATC trials should be expanded to include more patients that reflect the true ATC population (21), and regulatory agencies should mandate that these drugs be studied in suspension and via gastrostomy tube so that these drugs can be safely delivered to ATC patients who commonly cannot swallow.
Interestingly, in the present series, the single patient who progressed on dabrafenib plus trametinib did not have a BRAF mutation on cfDNA testing collected at the time of recurrence. His primary tumor, resected and then treated with adjuvant chemoradiation a year prior to cfDNA testing, was found to harbor a BRAFV600E mutation, which was the rationale for starting dabrafenib plus trametinib. Emergence of a subpopulation of cells without the BRAF mutation could explain why he did not respond to BRAF-directed treatment. Circulating cfDNA has proven to be a useful tool in monitoring response in patients with BRAF-mutated melanoma (22). Recent work has demonstrated a strong correlation between the mutation status of the tumor in ATC and circulating cfDNA (23). This is an important consideration, and studies are needed to validate the use of cfDNA for use as a monitoring tool and should be included in prospective ATC clinical trials. Since it is possible that cfDNA testing simply failed to detect circulating BRAF in this patient, re-biopsy of the tumor should be considered at the time of progression to determine if there is emergence of new mutations.
In the current series, the median time from diagnosis of ATC to starting targeted therapy was 3.4 months. During this period, 13 patients received some form of treatment for their ATC. Six patients received bridging chemotherapy with nab-paclitaxel or paclitaxel, or these drugs in combination with carboplatin, while awaiting genomic analysis of the tumor and procurement of their targeted therapy. Paclitaxel has been shown to be useful in shrinking the size of tumors in ATC and slowing progression in prior studies (7,24). This beneficial effect of paclitaxel was also observed in the current series, where none of these six patients progressed while receiving bridging chemotherapy. This strategy should be considered for patients who are awaiting results of molecular testing or insurance clearance, preventing patients from deteriorating, since ATC progresses rapidly.
In terms of tolerability, both targeted therapy regimens were well tolerated in the current series patients, irrespective of the multiple comorbidities. AEs observed in both groups were as expected and manageable. No patients died from drug-related AEs.
In the dabrafenib and trametinib group, the frequency of fatigue and nausea was higher than that reported in the basket trial (14). This is likely due to the pre-existing comorbidities or lower performance status in the patients in the current study. However, similar to this trial, grade 3 anemia and grade 3 hyponatremia were seen in these patients as well.
One patient on lenvatinib experienced hemoptysis. This patient developed a broncho-tumoral fistula. However, this occurred in the setting of progressive disease, and therefore it is unclear whether it was related to lenvatinib. Despite the high incidence of tracheal and great vessel invasion by tumor in the current series, there were no bleeding events. This may have been by chance or because many of the ATC patients were started on low-dose lenvatinib due to concern for bleeding and fistula. Severe hemorrhage from great vessel invasion remains a concern with lenvatinib (25).
One patient on lenvatinib experienced no AEs from the drug, including hypertension. This patient's BOR was PD on lenvatinib, despite tolerating the full dose of 24 mg. A study looking retrospectively at the therapeutic efficacy of VEGFR-tyrosine kinase inhibitors (TKIs), particularly sunitinib and pazopanib in metastatic renal cell carcinoma (mRCC), showed that hypertension might be a predictive factor of efficacy of VEGFR-TKIs therapy (26). Thus, the lack of hypertension in the single patient who progressed on lenvatinib is in accordance with the findings reported in mRCC. However, prospective studies to investigate this correlation are needed.
Limitations of this study include the retrospective nature, small sample size, and a short follow-up time. The retrospective nature makes it particularly difficult to report AEs confidently, since some may not have been documented and/or graded.
Conclusions
This study brings to light three important management issues in ATC. First, although treatment guidelines recommend clinical trials, most ATC patients are not eligible. Therefore, a relaxation of entry criteria in order to reflect the true population of ATC may be warranted. Second, bridging chemotherapy (if necessary) followed by targeted therapy drugs could be a useful strategy to relieve airway symptoms and/or stop progression of localized and distant metastatic disease in some advanced ATC patients. Third, all ATC patients should be tested for the presence of a BRAF mutation, as BRAF-directed therapy appears to be associated with the best clinical outcomes in ATC.
In summary, ATC patients with a reasonable performance status can be safely and effectively treated with dabrafenib plus trametinib if they harbor a BRAFV600E mutation, or with lenvatinib irrespective of the genomic findings. Our “real-world” results are inferior to the published clinical trials with lenvatinib and combination dabrafenib/trametinib but still reflect a major advancement in the treatment of ATC. Building upon this progress and knowledge, a clinical trial with bridging chemotherapy and the combination of targeted therapy and immunotherapy is currently underway (NCT 03181100).
Footnotes
Acknowledgments
This study was supported in part through The University of Texas MD Anderson Cancer Center's Cancer Center Support Grant CA16672.
Author Disclosure Statement
M.E.C. has received research funding from Eisai, Kura, and Genentech. R.D. received consulting fees from Eisai and Bristol-Myers Squibb. N.L.B. has received research funding from GlaxoSmithKline and Bayer and consulting fees from Eisai. M.A.H. has received research funding and consulting fees from Eisai. The remaining authors have no competing financial interests.