
Abstract
Background:
Hypoparathyroidism (hypoPT) is the most common complication following bilateral thyroid operations. Thyroid surgeons must employ strategies for minimizing and preventing post-thyroidectomy hypoPT. The objective of this American Thyroid Association Surgical Affairs Committee Statement is to provide an overview of its diagnosis, prevention, and treatment.
Summary:
HypoPT occurs when a low intact parathyroid hormone (PTH) level is accompanied by hypocalcemia. Risk factors for post-thyroidectomy hypoPT include bilateral thyroid operations, autoimmune thyroid disease, central neck dissection, substernal goiter, surgeon inexperience, and malabsorptive conditions. Medical and surgical strategies to minimize perioperative hypoPT include optimizing vitamin D levels, preserving parathyroid blood supply, and autotransplanting ischemic parathyroid glands. Measurement of intraoperative or early postoperative intact PTH levels following thyroidectomy can help guide patient management. In general, a postoperative PTH level <15 pg/mL indicates increased risk for acute hypoPT. Effective management of mild to moderate potential or actual postoperative hypoPT can be achieved by administering either empiric/prophylactic oral calcium and vitamin D, selective oral calcium, and vitamin D based on rapid postoperative PTH level(s), or serial serum calcium levels as a guide. Monitoring for rebound hypercalcemia is necessary to avoid metabolic and renal complications. For more severe hypocalcemia, inpatient management may be necessary. Permanent hypoPT has long-term consequences for both objective and subjective well-being, and should be prevented whenever possible.
Introduction
H
Background
The short half-life of PTH (3–5 minutes), along with the fragile nature of the parathyroid glands, sets the stage for their functional derangement following manipulation. The etiology of hypoPT is related to dissection or removal of the vulnerable parathyroid glands during central neck operations, resulting in a decline in circulating PTH.
Definitions
Biochemical hypoPT is defined as a low intact PTH level, below the lower limit of the laboratory standard (usually 12 pg/mL), accompanied by hypocalcemia. Ranges of normal PTH values vary, depending upon the laboratory.
Hypocalcemia is a total serum calcium level that is less than the lower limit of the center-specific reference range (5). Transient serum calcium values outside the normal reference range may reflect dynamic changes in electrolytes and state of hydration rather than true hypocalcemia. Hypocalcemia may occur independent of hypoPT, but untreated hypoPT always leads to hypocalcemia, even though time lag can range from hours to days.
Clinical hypoPT is defined as biochemical hypoPT that is accompanied by symptoms and/or signs of hypocalcemia.
Parathyroid insufficiency, or relative hypoPT, may occur after central neck surgery and typically is manifested by clinical symptoms of hypoPT that require medical treatment, despite measured laboratory values within normal ranges.
Transient or temporary hypoPT is defined as occurring for less than six months after surgery, while permanent hypoPT continues beyond six months after surgery (9).
Mechanisms
The mechanisms that underlie hypoPT are related to disruption of parathyroid arterial supply or venous drainage, mechanical injury, thermal or electrical injury, and either intentional or inadvertent partial or complete removal (10). Normal parathyroid function requires a rich blood supply; a normal parathyroid gland is composed of up to 30% capillary cells (11). Parathyroid blood supply is both delicate and complex, and requires close attention during thyroidectomy to ensure its preservation. While the inferior thyroid artery is typically the dominant blood vessel that supplies the parathyroid glands, laser Doppler flowmetry has shown that the superior thyroid artery and vessels within the thymo-thyroid cord (ligament) can dominate in some individuals (12).
Impaired PTH secretion results in postoperative hypocalcemia through inhibition of bone resorption, reduction of 1,25-dihyroxyvitamin D synthesis by the kidneys, and reduced intestinal absorption of calcium (13).
Symptoms and signs
Hypocalcemia causes neuromuscular excitability and cardiac electrical instability due to a reduced nerve and muscle cell depolarization threshold. Its most common early symptoms are paresthesias, or numbness and tingling, of the perioral region and the fingertips. Muscle stiffness, cramps, and spasms are also common. Neuropsychiatric symptoms include confusion, anger, depression, lightheadedness, and irritability. More sustained muscle contraction may lead to laryngospasm, and more severe neural excitability may lead to seizures.
Signs of hypocalcemia include observed or elicited tetany. Classic bedside findings are a positive Chvostek sign (facial muscle twitching upon tapping the preauricular region over the facial nerve; present at baseline in up to 25% of people), or a positive Trousseau sign (flexion of the wrist, thumb, and metacarpophalangeal joints and hyperextension of the fingers, upon brachial artery occlusion by inflation of a blood pressure cuff above systolic blood pressure). Cardiovascular signs observed with progressive hypocalcemia include prolongation of the QT interval that can result in torsades de pointes, a form of ventricular tachycardia that may degenerate into ventricular fibrillation.
Risk factors
HypoPT may follow any simultaneous or staged bilateral central neck operation. Risk factors for both temporary and permanent hypoPT are presented in Table 1 (2,14 –35). A prior partial thyroid operation creates a potentially increased risk of hypoPT during completion thyroidectomy, due to unknown status (presence or viability) of the parathyroid glands in the previously operated neck.
The most straightforward way to avoid hypoPT is to limit the extent of thyroidectomy to a unilateral approach. Though the historical rationale for a near-total or subtotal thyroidectomy, instead of a total thyroidectomy, is in part preservation of the parathyroid glands, it has never been adequately studied whether this actually reduces the risk of hypoPT (15).
Parathyroid autotransplantation (PA) at the time of thyroidectomy has been associated with an increased risk of temporary hypoPT. Paradoxically, routine PA may be associated with a reduced risk of permanent hypoPT. While data supporting propyhylactic PA are not definitive, the risk of permanent hypoPT is very low in patients who have undergone autotransplantation of at least one parathyroid gland (29).
Preoperative Vitamin D Deficiency
When the planned thyroid operation is bilateral, preoperative testing of baseline serum calcium, PTH, and 25-hydroxy vitamin D blood levels can be helpful. If the baseline calcium is low normal, or below normal, the risk of hypoPT is increased (36), and it may be appropriate to initiate scheduled oral calcium supplementation preoperatively. If the baseline calcium level is elevated, then the PTH level should be measured in order to evaluate for occult primary hyperparathyroidism, which could be definitively treated during thyroidectomy. A preoperatively elevated PTH level is commonly due to secondary hyperparathyroidism from vitamin D deficiency. Vitamin D increases the absorption of calcium from the intestinal tract, and supplementation may be helpful to patients with hypoPT, assuming no underlying malabsorptive condition is present. Vitamin D also increases bone resorption and decreases renal excretion of calcium and phosphate. Vitamin D deficiency can be severe (below the lowest recordable level, <10 ng/mL), moderate (10 to <20 ng/mL), or mild (20–30 ng/mL). To optimize postoperative oral calcium absorption, it is prudent to treat vitamin D deficiency preoperatively. The Food and Drug Administration (FDA) approved regimen is 50,000 IU of vitamin D3 (cholecalciferol) weekly or 6000 IU daily for eight weeks; more aggressive regimens and other vitamin D supplements are available, but their utilization should be considered off-label. Not all studies have substantiated improved postoperative calcium levels with higher preoperative vitamin D levels (37,38). Lang et al. found the rate of clinically significant hypocalcemia after total thyroidectomy to be similar in patients with severe, moderate, and mild vitamin D deficiency (39), whereas Al-Khatib et al. found that severe 25-hydroxyvitamin D deficiency was an independent predictor of hypoPT in patients undergoing total thyroidectomy (40). However, a large meta-analysis reported that the perioperative PTH level, the preoperative vitamin D level, and postoperative changes of calcium were biochemical predictors of post-thyroidectomy hypocalcemia (8).
Given the present evidence, it would appear preferable to diagnose vitamin D deficiency and initiate appropriate corrective supplementation prior to surgery (41). In cases of elective bilateral thyroid surgery, it may be prudent to delay surgery in order to correct severe vitamin D deficiency.
Surgical Techniques and Tools
Preservation of all four parathyroid glands during total thyroidectomy is a critically important operative goal, but this objective is not always attainable due to the extent of thyroid disease, plus variations in the anatomical locations and blood supply of the parathyroid glands. Avoiding parathyroid damage first requires that the surgeon is able to recognize parathyroid tissue accurately. The parathyroid glands are difficult to distinguish from other cervical tissues because of their small size and similar coloration compared to thyroid, fat, and lymph nodes. The time-honored key to parathyroid identification has been a proactive anticipatory visual approach and use of surgical landmarks. Recent promise for improved parathyroid identification has arisen through the intraoperative stimulation of parathyroid tissue fluorescence in the presence of a contrast agent or photosensitizer (indocyanine green, amino levulinic acid hydrochloride [5-ALA], methylene blue) and detection with near-infrared fluorescence imaging (42 –44). More recent still has been the successful detection of label-free parathyroid autofluorescence with near-infrared fluorescence spectroscopy (45,46).
A gentle capsular dissection that reflects the perithyroidal fatty tissues off the surface of the thyroid allows for preservation of the parathyroid blood supply. This technique requires dissection immediately on the surface of the thyroid gland medial or anterior to the parathyroids (Fig. 1). The importance of staying as distal to the parathyroid gland(s) as possible when dissecting cannot be overstated. Utilization of loupe magnification (2.5 × ) has been found to reduce significantly the rate of inadvertent parathyroid gland removal (3.8% vs. 7.8%), and both postoperative biochemical (20.6% vs. 33.9%; p = 0.028) and clinical (12.7% vs. 33%; p < 0.001) hypocalcemia (47).
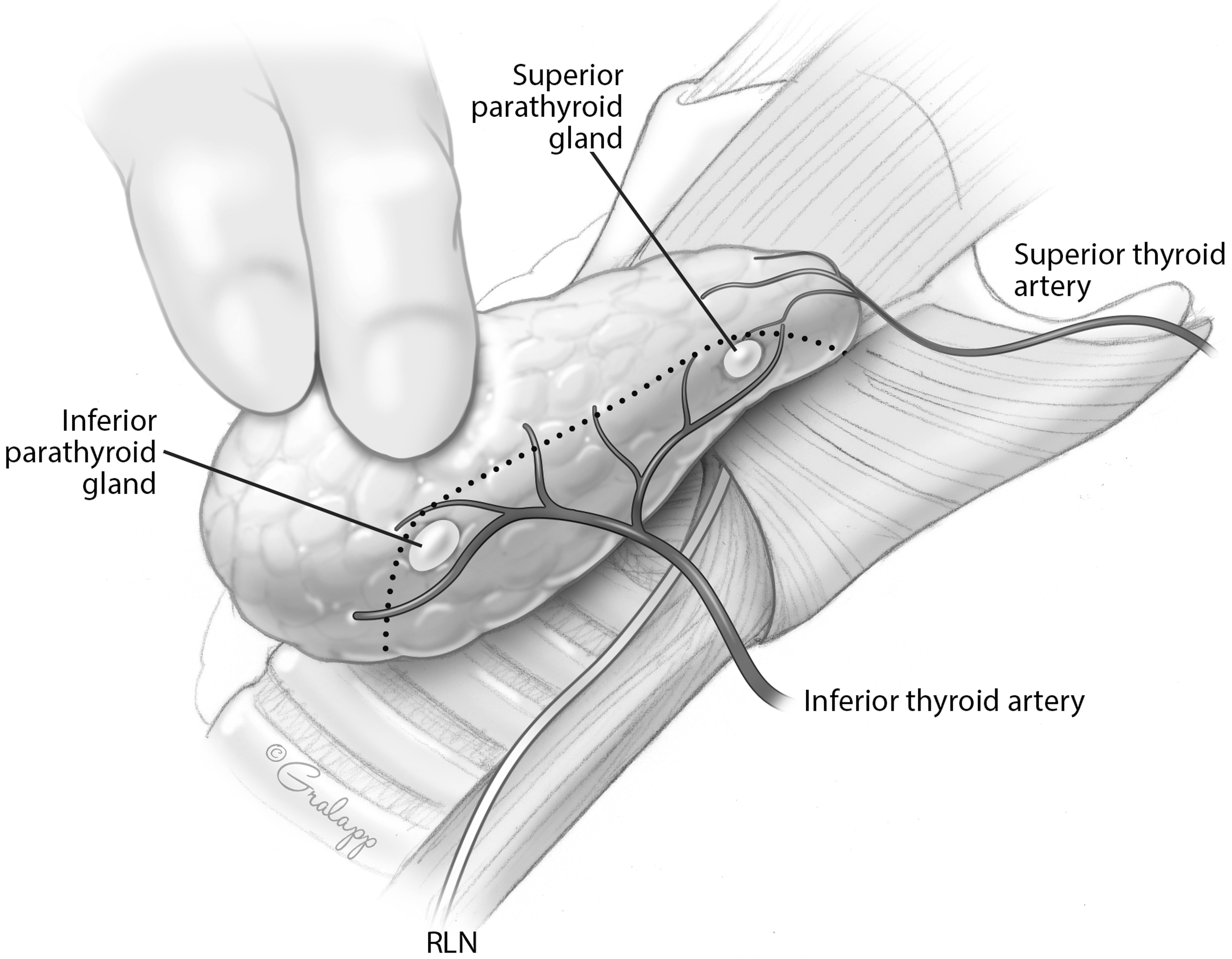
Plane of capsular dissection (dotted line) during thyroidectomy, dividing vasculature medial (distal) to the parathyroid glands in order to allow preservation of the parathyroid blood supply.
The use of energy devices for vessel sealing during thyroidectomy is another relevant surgical technical factor. These energy devices generate a zone of collateral thermal spread within the tissues, and necessitate an optimal 3–5 mm distance of separation between the instrument and the parathyroid gland in order to avoid thermal injury (48).
Interestingly, it is not essential to visualize all four parathyroid glands during thyroidectomy to reduce the incidence of postoperative hypocalcemia. Sheahan et al. reported that patients with zero to two parathyroid glands identified during thyroidectomy had a significantly lower incidence of clinical hypocalcemia compared to patients who had three to four parathyroid glands visualized (3.2% vs. 17.1%; p = 0.02) (49). In this study, the observed differences in biochemical hypocalcemia were not significant (16.1% vs. 28.1%; p = 0.13), and the incidence of inadvertent parathyroidectomy was similar (9.7% vs. 9.4%; p = 1.0). In contrast, Thomusch et al. demonstrated that during thyroidectomy, at least two parathyroid glands should be identified and preserved in order to avoid permanent hypoPT (50). The inferior parathyroid glands embryologically develop along with the thymus, and as such may be separated enough from the inferior pole of the thyroid to make their visual identification without dissection more difficult yet their preservation more likely during thyroidectomy.
Thyroid cancer surgery has an increased risk of hypoPT when a central lymph node dissection is performed. The superior parathyroid glands are at lower risk of injury or inadvertent removal than the inferior parathyroid glands, since most of the central neck lymph node metastases are generally located in the more inferior paratracheal and pretracheal areas. Sometimes, a small inferior parathyroid vein may be seen to course lateral and anterior to the carotid artery. When identified, it is important to preserve this vein, which can also be followed to facilitate identification of the inferior parathyroid gland. The blood supply to an ectopic intrathymic parathyroid gland is more difficult to preserve. Central neck lymph node dissection that is ipsilateral to the primary thyroid cancer should usually be performed first. Then, the risk of contralateral central neck lymph node metastasis must be weighed against the risk of hypoPT when deciding whether to proceed with further nodal dissection.
Parathyroid Autotransplantation
The identified parathyroid glands should be assessed for devascularization, and a decision made whether to perform PA, in order to maximize the amount of retained functional parathyroid tissue. Venous congestion may be alleviated by sharp scoring of the parathyroid gland capsule, which may result in prompt normalization or improvement in color. However, ischemia (arterial insufficiency) of a parathyroid gland may be subtle and difficult to detect, as the gland may appear only slightly pale to normal in color. A common surgical dilemma is whether autotransplantation of persistently or progressively discolored parathyroid glands is appropriate. Promberger et al. found that patients with discolored parathyroids only had transiently impaired function (51). They recommended PA only if there was clear evidence of ischemia or an inadequate blood supply.
PA is accomplished by first storing the excised parathyroid in iced saline while a sliver of the parathyroid tissue is submitted for frozen section confirmation. The parathyroid gland is then minced into 1 mm fragments that are autotransplanted by direct implantation or injection into either intramuscular or subcutaneous pockets, within the sternocleidomastoid muscle or elsewhere. The aim of PA is to reduce the risk of permanent hypoPT. Of note, much of the literature reporting on PA is focused on glands from patients with underlying hyperparathyroidism, and their observations may not extrapolate to the transplantation of devascularized parathyroids when preoperative parathyroid function was normal. Lo and Lam reported a higher incidence of postoperative hypocalcemia in patients who underwent PA during thyroidectomy compared to those who did not (21.4% vs. 8.1%; p < 0.01), but permanent hypoPT only occurred in the patients who did not undergo PA (1.8%) (52). However, in a different study, the same investigators found that routine PA was associated with a higher incidence of postoperative hypocalcemia, and did not lead to a significant reduction in the incidence of permanent hypoPT when compared to a policy of selective PA (53). A large Australian study examined the clinical outcomes after autotransplantation of zero, one, two, or three parathyroid glands (54). As the number of autotransplanted parathyroid glands increased, the incidence of temporary hypoPT increased respectively (p < 0.05), but the incidence of permanent hypoPT was similar at <1% (p = NS), respectively.
BIochemical testing: perioperative Calcium and PTH
The ability to predict the occurrence of transient hypoPT, by subjective surgeon assessment during operation, is highly variable (55). Objective serial measurement of serum calcium levels has traditionally been used to stratify for risk of symptomatic hypocalcemia development during the postoperative period, and to determine the need for oral calcium and calcitriol administration. After thyroidectomy, the absolute value of serum calcium levels, as well as the trend and slope or rate of change of these values, have also been employed to predict hypoPT (56 –59), but this approach requires sufficient time to observe such a trend. In one study, serum calcium levels were measured at 6 and 12 hours after total thyroidectomy, and patients with a positive serum calcium slope (rise in level) were deemed safe for hospital discharge with or without calcium supplementation (56). For patients with a non-positive slope but with serum calcium levels ≥8 mg/dL, discharge with calcium supplementation was also found to be safe.
Because trending calcium often requires sampling over a 12- to 24-hour or longer time period, and because postoperative calcium levels may be confounded by prophylactic calcium and calcitriol administration or by low preoperative vitamin D levels, many groups have examined the utility of measuring intraoperative or postoperative intact PTH levels drawn at various time points in the early post-thyroidectomy period (Table 2) (60 –77). Intraoperative PTH (IOPTH) refers to rapid processing of blood specimens drawn during or shortly after thyroid or central neck surgery to determine PTH levels that will influence surgical or postoperative management. At many institutions, the IOPTH assay provides a rapid, actionable result, whereas the routine intact PTH assay may not have a turnaround time that is fast enough for perioperative decision making. It is the normal short half-life of PTH (3–5 minutes) that enables decisions based on early postoperative PTH levels. The timing of PTH measurements in published studies has ranged from 10 minutes to 24 hours post thyroidectomy. McLeod et al. found that a low recovery room-drawn postoperative PTH level (<12 pg/mL) predicted the development of hypocalcemia, with a sensitivity of 100% and a specificity of 92% (61). Sywak et al. reported that a low four-hour postoperative PTH level (3–10 pg/mL) had a sensitivity of 90% and a specificity of 84% for predicting postoperative hypocalcemia (65), and Asari et al. reported that an intact PTH level of ≤15 pg/mL on postoperative day 1 predicted hypoPT, with a sensitivity of 97.7% and a specificity of 82.6% (72). Thus, the earliest opportunity to predict hypoPT reliably is through measurement of serum PTH level either at the conclusion of or immediately following surgery.
PTH, parathyroid hormone.
A PTH level <15 pg/mL is usually predictive of impending hypocalcemia (61,62,64,65,69 –73,76,77). IOPTH levels measured alone or combined with serum calcium level measurements may guide the decision to discharge versus monitor patients in the hospital setting, to prescribe prophylactic oral calcium, or to take more aggressive measures to prevent or treat hypocalcemia.
Based on the available evidence, and acknowledging that reference ranges differ based on assay and institution, it is the opinion of the ATA Surgical Affairs Committee that a PTH value ≥15 pg/mL measured in adults at ≥20 minutes following thyroidectomy would obviate the need for intensive serum calcium monitoring and/or calcium supplementation. A postoperative PTH value of <15 pg/mL would suggest an increased risk for acute hypoPT that might prompt preemptive prescribing of oral calcium and calcitriol and/or serial serum calcium measurements until calcium stability has been confirmed.
The ability to predict transient as opposed to permanent hypoPT following thyroidectomy is uncertain. At least one study found that acute postoperative hypoPT specifically did not predict permanent hypoPT (78). Several parameters, including postoperative PTH values, decline in PTH values between preoperative and postoperative measurements, degree of decrease in magnesium levels, and whether PA was carried out, have been associated with the risk of permanent hypoPT (79 –82). However, the utilization of these parameters is not consistently established and requires further investigation.
Postoperative Management
The goal of managing hypoPT, potential or actual, is to avoid the symptoms and complications of hypocalcemia. Acute symptoms may range from subtle to profound, and fortunately recognizable symptoms of mild to moderate hypocalcemia usually precede more life-threatening complications of severe hypocalcemia. Development of acute hypocalcemia after thyroid surgery lags behind the decline in the serum PTH level, and the patient may have been discharged from the hospital prior to their serum calcium having reached a nadir, which may occur 24–72 hours after thyroidectomy. Therefore, it is important to anticipate the possibility of progressive hypocalcemia, to educate patients about its possible development and steps they should take to avoid and treat it, and to institute measures that both prevent and correct hypocalcemia in the postoperative period.
Individuals with normal parathyroid function who undergo thyroid or central neck operation are at risk for developing hypoPT with different kinetics and recovery than those who undergo parathyroidectomy for treatment of hyperparathyroidism. The distinction of normal preoperative parathyroid function may be confounded because many patients take calcium, vitamin D, and/or other supplements on a routine or intermittent basis. Postoperative measurement of absolute values and trends of calcium as total or ionized calcium blood levels are the mainstay of clinical monitoring. However, consideration of vitamin D and magnesium levels is also necessary.
The cost of measuring ionized calcium level can be significantly higher than the cost of measuring serum calcium (83). Despite the ionized calcium level having been shown to be a more sensitive indicator than serum calcium for the diagnosis of hyperparathyroidism (84), it is not necessarily more sensitive or useful to guide the management of hypoPT (83,85). However, at least one perioperative serum albumin level should be measured to allow for calculation of the corrected calcium level.
Prophylactic Postoperative Management
An empirical prophylactic approach for managing potential post-thyroidectomy hypocalcemia is to prescribe oral calcium routinely with or without oral calcitriol, without testing PTH or calcium levels (86,87). This approach is cost-effective, is not labor intensive, is expeditious, and can hasten hospital discharge after thyroidectomy (60,68,70,74,76,88 –93). Oral calcium carbonate is the most widely available and inexpensive preparation, and is given as 500–625 mg to 1000–1250 mg two to three times a day. Routine administration of oral calcium has been reported to reduce postoperative hypocalcemia to approximately 10% (94). Adding calcitriol (1,25-(OH)2-D3), usually in a dose of 0.5–1.0 μg per day, adds to the cost but increases the effectiveness of oral calcium. Calcitriol increases intestinal absorption of calcium and also mobilizes calcium from bone. The half-life of calcitriol is relatively short (5–8 hours), and toxicity from excessive calcitriol ingestion may be reversed quickly (within days), although in patients with renal failure its half-life may double. In contrast, the fat-soluble vitamin D3, cholecalciferol, has a half-life of weeks to months (95), and toxicity may lead to soft-tissue calcification, nephrolithiasis, nephrocalcinosis, or chronic renal failure. 25 OH-vitamin D also requires conversion to active 1,25 OH-vitamin D by 1-α-hydroxylase, which is a PTH- and magnesium- dependent enzyme. A prospective, randomized study of patients after total thyroidectomy found that 1500 mg of oral calcium salts and 1 μg of calcitriol administered twice a day was superior to 0.5 μg of calcitriol administered twice a day or no calcitriol (96). This aggressive prophylactic approach has an associated uncommon but serious risk of overshooting and causing hypercalcemia and potential renal injury. So, biochemical monitoring for medication tapering is mandatory. Prophylactic measures also depend upon patient compliance and tolerance of oral intake. Still, the cost of calcium carbonate and calcitriol tend to be less than the cost of PTH testing. On the other hand, even the cost of PTH testing is considerably lower than the cost of an emergency room visit or hospital admission.
While transient prophylactic calcium and calcitriol may bridge the recovery period for “stunned” or briefly dysfunctional parathyroid glands, it is unnecessary in a certain (unknown unless tested) proportion of patients. However, when acute hypoPT is known to be present, it has been found that the more aggressive the calcium and activated vitamin D replacement is, the better the chances of parathyroid recovery (97).
Treatment of early/Mild to Moderate Hypoparathyroidism
Patients whose PTH is <15 pg/mL, serum calcium is <8.5 mg/dL, or ionized Ca is <1.1 mmol/L should be considered for postoperative oral calcium supplementation. A regimen of 400–1200 mg per day of elemental calcium (1–3 g of calcium carbonate; i.e., 2–6 TUMS per day) or the equivalent in calcium citrate (2000–6000 mg per day) administered orally in divided doses is usually sufficient (5). Calcium carbonate (40% elemental calcium) and calcium citrate (21% elemental calcium) are the most common calcium salts and should be taken with meals. Calcium carbonate requires an acidic environment to dissolve. Patients on proton pump inhibitors, elderly patients with achlorhydria, and gastric bypass patients may be better treated with calcium citrate, which does not require an acidic environment for absorption (98). Some patients report fewer gastrointestinal side effects with calcium citrate, and calcium citrate tablets tend to be smaller and easier to swallow, although chewable and liquid options are available for both. Oral calcium dosing should be separated from oral thyroid hormone replacement, as calcium inhibits levothyroxine absorption. Levothyroxine should be taken one hour before or three hours after calcium salts are taken (99). The prolonged period of fasting that occurs during sleep may also contribute to early morning hypocalcemia if oral calcium is prescribed three times daily rather than every eight hours.
If the patient has symptomatic hypocalcemia and a serum calcium level that is declining on sequential measurements or remaining <7 mg/dL, then calcitriol, typically 0.25–0.5 μg twice daily, may be added to their regimen. Furthermore, magnesium depletion impairs PTH release and activity. So, if the serum magnesium is <1.6 mg/dL in a patient with normal renal function, magnesium supplementation with 400 mg of magnesium oxide once or twice daily can expedite calcium recovery and may also diminish the constipation commonly associated with high-dose calcium replacement.
Treatment of Progressive/Symptomatic Hypoparathyroidism
If symptoms or signs of hypocalcemia progress despite treatment, and serum calcium remains <7 mg/dL, not only calcium but also magnesium levels should be measured and supplemented as needed. If severe symptomatic hypocalcemia develops despite oral calcium and calcitriol therapy, then a 12-lead EKG should be performed, corrected QT interval (QTc) measured, and intravenous (i.v.) calcium administered. Calcium given by i.v. bolus (1–2 g of calcium gluconate [93 mg elemental calcium in one vial of calcium gluconate] in 50 mL of 5% dextrose infused over 20 min) is the most expeditious but also the least durable method for raising serum calcium rapidly. A calcium drip or slow i.v. infusion provides more consistent blood levels and, by employing serial measurements, may be adjusted to maintain the calcium level in the low normal range. Calcium gluconate (90 mg of elemental calcium per 10 mL) is the preferred salt for peripheral i.v. repletion. Calcium chloride (270 mg of elemental calcium per 10 mL) is prone to causing phlebitis and local tissue necrosis unless delivered through a central line, or diluted to approximately one-third concentration for peripheral administration (100). However, initiation of a calcium drip also necessitates electrocardiographic monitoring because of the risk associated with potential calcium overdose, and also because patients with severe hypocalcemia are prone to cardiac instability, QTc prolongation, or even development of torsades de pointes. The patient receiving a calcium drip should have their oral calcium and calcitriol doses increased as soon as feasible and their drip weaned as tolerated.
When calcium control remains difficult despite all of the above measures, thiazide diuretics may be considered. Thiazides enhance distal renal tubular calcium reabsorption, thereby enhancing retention of calcium that is being supplemented and reducing urinary calcium excretion. If no contraindications exist, hydrochlorothiazide 12.5–50 mg daily may be effective, but it must be titrated to avoid hypotension.
Once a patient is stable enough on oral therapy alone to be discharged, calcium levels must still be followed, and calcitriol dose should be gradually reduced once a steady state is achieved. Patients undergoing thyroidectomy for Graves' disease are especially at risk because demineralized bone becomes re-calcified through the “Hungry Bone Syndrome” after surgery (101). After several weeks of treatment for hypocalcemia, rebound hypercalcemia may result and will necessitate reduction in the dose of calcitriol.
These approaches to the postoperative management of hypoPT are summarized in Table 3.
Optimize 25 OH-vitamin D levels and serum magnesium.
Serum Ca <8.5 mg/dL, new-onset symptoms.
Serum Ca <7.0 mg/dL, persistent/severe symptoms despite therapy; check EKG for QTc prolongation.
Calcium carbonate, or equivalent in calcium citrate.
i.v., intravenous; N/A, not applicable.
Long-Term Management of Hypoparathyroidism
The long-term management of hypoPT aims to maintain serum calcium within the asymptomatic range, avoid significant hypocalcemia or hypercalcemia and its associated complications, and preserve bone health. In order to minimize the risk of symptoms, serum calcium should be maintained in the low normal reference range, and serum phosphorus should be maintained no higher than the upper normal range. Recommendations for 24-hour urine calcium excretion <7.5 mmol/day and calcium-phosphorus product <55 mg2/dL2 have been advocated (102). A high calcium phosphorus product (typically only seen in patients with renal failure, but exacerbated by hypervitaminosis D) poses a risk for calciphylaxis, in which vascular calcification, thrombosis, and skin necrosis occur. The mortality of calciphylaxis is usually associated with sepsis and approaches 45–50% (103). Long-term management of hypoPT is usually best accomplished under the care of a medical professional with expertise in this area.
Calcium supplementation doses that range up to 3500 mg of elemental calcium per day have been reported, with most patients requiring 1500 mg daily. Therapy in two to three divided doses offers the best absorption. Calcitriol is usually recommended, with most patients requiring 0.25 μg of calcitriol daily (0.25–4.0 μg/day). Vitamin D2 (ergocalciferol) or vitamin D3 (cholecalciferol) are occasionally used for long-term management, given their much longer half-lives compared to the activated metabolite of vitamin D (calcitriol). Vitamin D therapy does increase intestinal phosphate absorption. So, when hyperphosphatemia is significant, intestinal phosphate binders may be necessary (102).
To prevent hypercalciuria (>150 mg/24 h), and to reduce the total amount of calcium supplementation needed to maintain adequate circulating levels of calcium effectively, hydrochlorothiazide 12.5–50 mg daily can be added to the regimen.
Even after a patient is stabilized on an oral calcium and vitamin D regimen, episodes of hypocalcemia or hypercalcemia may occur in the setting of acute illness, dehydration, or stress. Pregnancy and lactation also affect calcium and vitamin D requirements and metabolism, and special precautions should be taken when prescribing supplements under these conditions. There are no controlled data on the use of calcitriol in human pregnancy; it has been classified as U.S. FDA pregnancy category C, indicating that animal reproduction studies have shown an adverse effect on the fetus, and advising that it not be used during pregnancy unless the benefit outweighs the risk to the fetus. Calcitriol use is also not recommended during lactation because it is presumed to pass into breast milk. Thus, if it is used during breastfeeding, serum calcium levels of both mother and infant should be monitored (104).
Patients who have undergone prior Roux-en-Y gastric bypass surgery or other duodenal resection have an increased risk for postoperative hypocalcemia due to malabsorption issues. Gastric bypass patients may have elevated PTH levels following their bariatric surgery, even when their vitamin D levels are normal (32,33), but especially when vitamin D levels are deficient. This scenario can profoundly complicate management of both temporary and permanent postoperative hypoPT (34,35). Liquid calcium may improve absorption in these cases. In extreme circumstances, gastric bypass reversal could be considered.
Long-standing hypoPT may have a substantial impact on quality of life. The consequences of long-term loss of parathyroid regulation of calcium metabolism, even when treatment achieves normal blood calcium levels, include nephrolithiasis, nephrocalcinosis, basal ganglia calcification, ectopic soft tissue calcification, cataracts, and potential defects in bone metabolism. In rare instances, renal failure requiring hemodialysis or renal transplantion may occur. To avoid this complication, periodic renal ultrasound and 24-hour urine calcium measurement are important (105). Bone microarchitecture in hypoparathyroid patients is abnormal, and while mineral content tends to be increased, bone stiffness is also increased, and consequently bones may be predisposed to develop microfractures when loaded (102). Unfortunately, standard DXA testing is not effective in assessing this risk. Additionally, patients with hypoPT often report increased anxiety and a decreased sense of well-being when compared with controls (102).
The FDA approved recombinant human PTH (1 –84) (rhPTH[1–84]) in January 2015 for treatment of patients with refractory hypoPT. The double-blind, placebo-controlled, randomized, Phase III REPLACE trial demonstrated that when rhPTH(1 –84) 50–100 μg was injected subcutaneously once daily, 53% of adult hypoparathyroid patients were able to reduce their calcium and vitamin D requirements by >50%, and 43% were able to achieve independence from vitamin D and reduce calcium to <500 mg daily (106,107). Urinary calcium and serum phosphorus levels were also reduced, and quality-of-life indexes were improved compared to traditional management (106,107). rhPTH(1 –84) may also restore normal bone metabolism and improve bone microarchitecture. Due to the potential risk of osteosarcoma associated with rhPTH(1 –84) therapy, only certified healthcare providers may prescribe it and only certified pharmacies can dispense it under an FDA-mandated Risk Evaluation and Mitigation Strategy program.
Teriparatide acetate (recombinant human PTH 1–34; rhPTH[1–34]) is an approved treatment for osteoporosis, and it is currently being studied as a possible off-label treatment for postoperative hypoPT (108).
Summary
Knowledge of the causes and effects of hypoPT is essential for its prevention and optimal management. A summary of key recommendations is provided in Table 4. Individual surgeons should strive to recognize their own rates of hypoPT and minimize this complication through the measures reviewed. Thoughtful preoperative assessment, meticulous intraoperative surgical technique with potential use of technical adjuncts (especially PTH testing), and prompt diagnosis and judicious treatment should minimize or eliminate the risks and negative consequences of hypoPT.
Footnotes
Author Disclosure Statement
B.C.S. Jr. has the following disclosure: Speakers bureau, Shire (Natpara). He did not specifically recommend this product in the treatment of hypoparathyroidism for this paper. No competing financial interests exist for the remaining authors.