
Abstract
Background:
Gene fusions are known in many cancers as driver or passenger mutations. They play an important role in both the etiology and pathogenesis of cancer and are considered as potential diagnostic and prognostic markers and possible therapeutic targets. The spectrum and prevalence of gene fusions in thyroid cancer ranges from single cases up to 80%, depending on the specific type of cancer. During last three years, massive parallel sequencing technologies have revealed new fusions and allowed detailed characteristics of fusions in different types of thyroid cancer.
Summary:
This article reviews all known fusions and their prevalence in papillary, poorly differentiated and anaplastic, follicular, and medullary carcinomas. The mechanisms of fusion formation are described. In addition, the mechanisms of oncogenic transformation, such as altered gene expression, forced oligomerization, and subcellular localization, are given.
Conclusion:
The prognostic value and perspectives of the utilization of gene fusions as therapeutic targets are discussed.
Introduction
T
Effective and appropriate treatment management requires differentiating benign from malignant nodules, thyroid lymphomas, and metastases to the thyroid. In contrast to thyroid carcinomas, thyroid lymphomas do not require surgery. Conventional treatment strategies used for the treatment for DTC, such as radioactive iodine (RAI), is unnecessary and ineffective in patients with ATC or MTC (8 –10). The noninvasive encapsulated follicular variant (FV) of papillary thyroid carcinoma (PTC), recently reclassified as noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP), has a very low risk of adverse outcome and is unlikely to benefit from immediate completion thyroidectomy and RAI therapy (11). The use of ultrasound-guided fine-needle aspiration (FNA) biopsies enables a preoperative diagnosis of thyroid lesions to be established. However, in 20–30% of nodule aspirates, the cytological examination yields an “indeterminate” result, with the risk of malignancy ranging from 5% to 75% (12).
To address the diagnostic shortcomings and improve treatments, new approaches characterizing molecular markers such as gene mutations, miRNA, and gene expression profiles are being developed (13,14). Gene fusions have been recognized as important driver events in different types of cancer and are considered as potential diagnostic markers or therapeutic targets in anticancer treatment (15,16). Oncogenic fusions are generated via balanced and unbalanced chromosome rearrangements such as translocations, insertions, inversions, and deletions of chromosomal segments. Chromothripsis is another possible mechanism of fusion generation characterized by multiple simultaneous rearrangements (17,18). Rearrangements in intronic regions result in intact exon type fusion transcripts characterized by transcript breakpoints located exactly at the boundary of the exons. In contrast, in broken exon type transcripts, the breakpoint can be in the middle of the exon (19). Additionally, fusion transcripts can be formed at the transcriptional level via trans- or cis-splicing (20,21). The consequences of gene fusions are novel chimeric proteins with altered expression, function, subcellular localization, or forced oligomerization (22,23). Until 2010, fusions were difficult to detect, and many of the findings were serendipitous and not due to systematic analyses. Gene fusions in thyroid cancer were thought to be predominantly associated with exposure to radioactivity. However, new high-throughput massive parallel sequencing (MPS) technologies now permit a rapid and systematic search for new and known gene fusions in thyroid cancer. The spectrum of gene fusions varies between different types of tumors, and knowledge of their frequencies and types may help both diagnosis and the development of targeted therapies. Here, current data on gene fusions in thyroid cancer are summarized and classified.
Landscape of Gene Fusions in Thyroid Cancer
The landscape of gene fusions correlates with the histological subtypes of thyroid carcinomas. Fusions of tyrosine kinases activating the MAPK pathway can be found in PTC. In contrast, follicular thyroid carcinomas (FTC), follicular adenomas, and FVPTC tend to harbor PPARG and THADA gene fusions.
PTC
Oncogenic fusions can be found in 6–46% of sporadic PTC cases (24 –27). In the TCGA study, fusions were found in 15.3% of 484 PTCs (24). Genes described to be rearranged in PTC include RET, BRAF, NTRK1, NTRK3, ALK, PPARG, and THADA (Table 1).
Bold indicates novel fusions uncovered since 2014 using massive parallel sequencing.
Found predominantly in encapsulated FVPTC.
PTC, papillary thyroid carcinoma; PDTC, poorly differentiated thyroid carcinoma; ATC, anaplastic thyroid carcinoma; FTC, follicular thyroid carcinoma; MTC, medullary thyroid carcinoma; FVPTC, follicular variant of PTC.
RET fusions
RET fusions (known as RET/PTC rearrangements) are the most common rearrangement in PTC. In sporadic papillary carcinomas, RET/PTC prevalence ranges from 10% to 30%, while in child and adolescent sporadic PTC, the frequency is higher, up to 45–60% (28 –32). Radiation-induced PTC is also characterized by the high frequency of RET/PTC fusions, ranging from 35% up to 50–80% of cases (32 –34). To date, at least 19 RET/PTC fusions have been described (Table 1).
The major RET/PTC fusions are CCDC6-RET (RET/PTC1) and NCOA4-RET (RET/PTC3), which comprise in total up to 90% of all RET/PTC rearrangements. In sporadic thyroid cancer, the frequency of CCDC6-RET rearrangements is more than two times higher than the frequency of NCOA4-RET fusions. In contrast, in radiation-induced PTC, NCOA4-RET has an equal or even higher prevalence compared to CCDC6-RET fusions (35,36). Leeman-Neill et al. studied the RET/PTC and PAX8/PPARγ chromosomal rearrangements in post-Chernobyl thyroid cancers (37). They showed that the frequency of cases harboring CCDC6-RET fusions exceeded that of NCOA4-RET fusions, but the average 131I dose was higher in NCOA4-RET cases, and the presence of NCOA4-RET was negatively associated with the time between exposure and surgery (37). A meta-analysis of the NCOA4-RET distribution performed by Su et al. included 2395 radiation-induced and sporadic PTC cases. They demonstrated that radiation exposure contributed to an increased RET/PTC risk, and this association was restricted to the NCOA4-RET subtype in the Western population (38). PRKAR1A-RET (RET/PTC2) is less prevalent and is found in <10% of RET/PTC cases (28,39,40).
Rare RET fusions include RET/PTC4 (unlike RET/PTC3, it has an unconventional intra-exonic breakpoint in exon 11 of NCOA4) (41), GOLGA5 (RET/PTC5), TRIM24 (RET/PTC6), TRIM33 (RET/PTC7) (36,42), KTN1 (RET/PTC8) (43,44), RFG9 (RET/PTC9), RET-ERC1 (29,45), RET-PCM1 (46), RET-TRIM27 (47), RET-HOOK3 (34), and many others discovered recently with high-throughput MPS (24 –27,48). These fusions have been reported in one or two cases each, with no history of prior radiation exposure. With an explosive increase in the discovery of novel fusions, RET/PTC acronyms are no longer used. The current list of known RET fusions is summarized in Table 1.
NTRK fusions
NTRK fusions can be found in up to 2–3% of sporadic PTC cases (24,26,27). The major NTRK fusion is ETV6-NTRK3, which was found in 14.5% of post-Chernobyl PTC cases and is thought to have a strong association with radiation exposure (49,50). Despite the association of NTRK3 fusions with radiation, Prasad et al. identified ETV6-NTRK3 fusions in 22% of tumors from a pediatric cohort with no significant exposure to radiation (25). NTRK1 rearrangements were also described in PTCs but with lower frequency. The prevalent NTRK1 fusions are TPM3-NTRK1 (also known as TRK), TPR-NTRK1 (TRK-T1 and TRK-T2), and TFG-NTRK1 (TRK-T3) (25,51). Novel NTRK fusions uncovered in PTC using MPS include RBPMS-NTRK3, SQSTM1-NTRK3, IRF2BP2-NTRK1, SQSTM1-NTRK1, and SSBP2-NTRK1 (Table 1) (24,26).
BRAF fusions
A BRAF fusion was found for the first time by Ciampi et al. in 11% of early radiation–associated tumors and in 1% of children and adolescents with sporadic tumors, and the identified partner gene was AKAP (52). Since then, at least 13 novel BRAF fusions have been described in PTC (24,26,27).
ALK fusions
ALK fusions do not exceed 1–3% of papillary carcinomas (53 –55). The best characterized fusions include STRN-ALK and EML4-ALK, among which STRN-ALK is the most prevalent. Novel ALK fusions (GTF2IRD1-ALK and MALAT1-ALK) were discovered in the TCGA study (24).
The TCGA study demonstrated the following fusion prevalence in PTC: RET in 6.8%, BRAF in 2.7%, NTRK3 in 1.2%, NTRK1 in 0.8%, and ALK in 0.8% of tumors. Additionally, PPARG and THADA fusions were found; these fusions were more prevalent in FVPTC, while rare cases were discovered in classical PTC (24).
FVPTC
The fusion profile of FVPTC is dependent on the histologic subtype, that is, infiltrative (non-encapsulated) or encapsulated FVPTC, which are associated with distinct clinical outcomes. Fusions in infiltrative FVPTC include RET/PTC and NTRK1/3 fusions. In contrast, PAX8-PPARG predominates in encapsulated FVPTC (56,57). Recently, noninvasive encapsulated FVPTC was reclassified as NIFTP. Nikiforov et al. found PPARG and THADA fusions in 22% of NIFTP cases, whereas these fusions were absent in non-encapsulated FVPTC (11). It is interesting to note that the non-encapsulated FVPTC has the same fusion and mutation profile (BRAF mutations) as classical PTC, whereas the encapsulated FVPTC has similar fusions and RAS mutations as follicular adenomas and FTC.
Currently, there is insufficient and controversial data on the association of gene fusions and clinicopathologic outcomes of PTC. Several studies claim that some fusions are associated with more extensive disease and aggressive pathology (large size, solid and diffuse variants, tumor stage, lymphovascular invasion, metastases) (25,53). In contrast, others suggest the absence of differences in clinicopathologic features of gene fusion–driven cases (24,58,59). In the TCGA study, no association was found between gene fusions and cancer recurrence (24). Based on the overall low prevalence of fusions in a cohort with metastatic thyroid carcinomas (6.6% of 90 PTC cases) described by Zehir et al., gene fusions may in general be associated with a low risk for metastasis (27). However, in a PTC cohort studied by Lu et al., gene fusions were found in 18% of cases with lymphatic metastasis and in 17% of cases with extra-glandular invasion, whereas only 1.4% and 4.6% without lymphatic metastasis and without extra-glandular invasion were found to have fusions, respectively (26). Thus, the latter data do not support the concept of a more indolent behavior of gene fusion–driven papillary carcinomas.
PDTC and ATC
PDTC and ATC are rare types of thyroid cancer, and gene fusions have been found in few cases, mainly using MPS (Table 1). In PDTC, rearrangements were found in 10–14% of cases and include RET/PTC, ALK, BRAF, NTRK3, and PAX8-PPARG fusions (Table 1) (60,61). No correlation of gene fusions and clinicopathologic features was observed in PDTC (60). Fusions described in ATC included RET/PTC3, STRN-ALK, NUT-BRD4, and KIAA1549-BRAF. In ATC, fusions were identified in about 3–5% of cases (54,61,62). The relatively low prevalence of gene fusions in PDTC and ATC contradicts the concept that gene fusion–driven carcinomas have more potential to undergo dedifferentiation.
FTC
PAX8-PPARG rearrangements are almost exclusively found in FTC (30–60% in FTC) (63 –67). Occasional DERL-COX6C and CREB3L2-PPARG fusions have also been described (Table 1) (68).
MTC
The landscape of oncogenic events in MTC is less well characterized. Hereditary MTC is strongly associated with germline point mutations occurring in the RET gene. Sporadic MTC harbor somatic RET point mutations in up to 40%, and RAS mutations can be found in 10–15% of cases (69,70). Recently, three cases of MTC harboring gene fusions (MYH13-RET, GFPT1-ALK, and EML4-ALK) have been reported (Table 1) (70,71).
Adenomas and benign nodules
In follicular adenomas, PAX8/PPARG fusions were found with varying frequency. The highest was 55% (64,65,72). Several studies provide evidence that RET/PTC1 and RET/PTC3 rearrangements can be found in benign nodules, with the highest frequency of about 13% in sporadic nodules (30). RET/PTC positive nodules were found to grow faster compared to nodules without fusions (73,74).
It can be concluded that fusions including tyrosine kinases activating the MAPK pathway are more likely to be associated with classic PTC. In contrast, PPARG and THADA fusions are more common in follicular neoplasms with a more indolent behavior. Consistent with this observation, PPARG and THADA fusions may be considered as possible markers of more favorable outcomes.
Mechanisms of Oncogenic Activation
Known oncogenic fusions in thyroid cancer derive from intrachromosomal paracentric inversions (CCD6C-RET, NCOA4-RET, TPM3-NTRK1, TPR-NTRK1, and AKAP9-BRAF) or reciprocal balanced translocations (rare RET fusions, ETV6-NTRK3, TFG-NTRK1, and PAX8-PPARG). The STRN-ALK fusion is supposed to result from a deletion of a chromosome 2 fragment or from chromothripsis (53,54). It is proposed that proximity of the involved loci in the interphase nuclei provides the structural basis for the chromosomal aberrations. Thus, reduced distance between CCD6C and RET, TPR, and NTRK1 has been shown in thyroid interphase nuclei (75 –77).
Receptor tyrosine kinase fusions
The most prevalent fusions in thyroid cancer involve receptor tyrosine kinases (RTK), that is, RET, NTRK1, NTRK3, and ALK. The general structure of these kinases includes three domains: an extracellular ligand-binding domain, a hydrophobic transmembrane domain, and a cytoplasmic portion with the TK domain. Binding of specific ligands (growth factors such as TGF-beta, NGF-beta, or the pleiotrophin family) leads to homodimerization and autophosphorylation of the tyrosine residues in the tyrosine kinase domains. Activated RTK trigger intracellular signaling through MAPK/ERK and PI3K/Akt pathways, regulating cell growth, proliferation, and survival (78,79).
Oncogenic RTK fusions are comprised of the 3′ portion coding tyrosine kinase domain of the RTK gene (acceptor) and the 5′ portion of a partner gene (donor). The RTK portions of the fusions start with the following exons of the genes: 12 for RET, 15 (rarely 14) for NTRK3, 10 (rarely 9) for NTRK1, and 20 for ALK (Fig. 1).
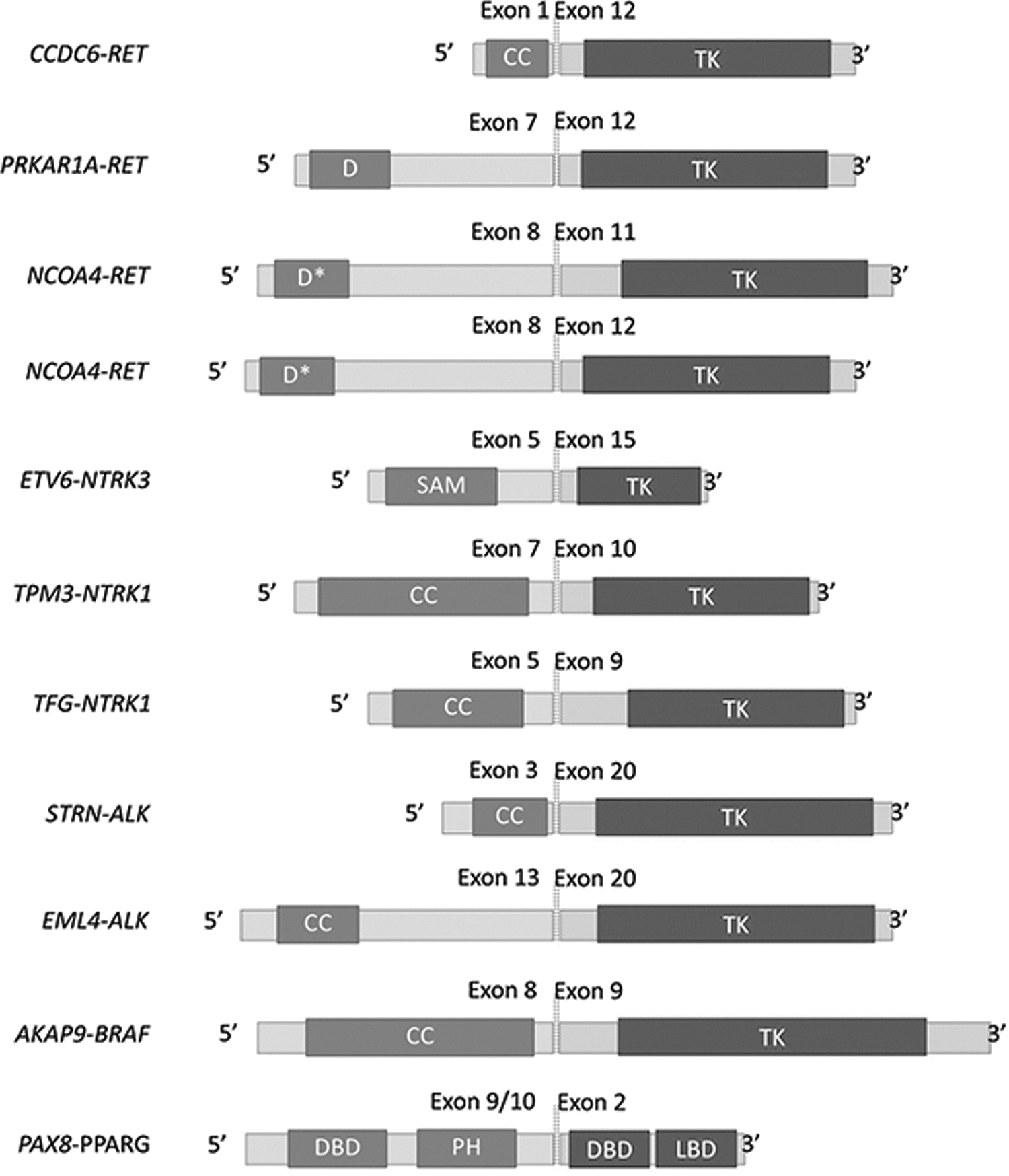
Structure of fusions major in thyroid cancer. CC, coiled coil domain; TK, tyrosine kinase domain; D, dimerization domain; SAM, sterile alpha motif; DBD, DNA binding domain; PH, partial homeobox. *Putative.
Several mechanisms can be implicated in the activation of the RTK transforming potential by rearrangements. First, transcriptional promoters of RTK fusions are substituted with those of the donor partners, which are often ubiquitously expressed. This enables expression of RTK in epithelial follicular thyroid cells, where it is normally transcriptionally silent. Second, all known partner genes encode dimerization domains, such as coiled coil, SAM domain, leucine zipper, or helix–loop–helix domains that drive ligand-independent activation of the chimeric protein (23). Finally, the chimeric oncoproteins are distributed in the cytosolic compartment of the cell. In addition, disruption of the normal function of the fusion partner gene might also have an important role. Thus, oncogenic rearrangements can result in loss of tumor-suppressor function of PRKAR1A in RET/PTC2, or proapoptotic activity of CCDC6 in RET/PTC1 (80,81).
BRAF fusions
BRAF encodes a serine-threonine protein kinase that phosphorylates MAPK/ERK kinase (MEK) within the MAPK cascade. The kinase domain of BRAF is inhibited by its RAS-GTP-binding domain (RBD) located in the amino-terminal regulatory region. Binding of RAS-GTP to the RBD domain triggers conformational changes through which the kinase domain becomes active (82,83). The AKAP9-BRAF fusion is an in-frame fusion of the 5′ portion (exons 1–8) of the A-kinase anchor protein 9 (AKAP9) gene, with the 3′ portion (exons 9–18) consisting of the catalytic domain of BRAF (Fig. 1). The loss of the regulatory CR1 domain of BRAF subsequent to the rearrangement results in constitutive kinase activity of the chimeric protein, and mitogenic signaling through the MAPK pathway. Additionally, deregulation of AKAP9 function might contribute to the pathogenic effect of AKAP9-BRAF (52).
PAX8/PPARG fusions
PAX8 is a transcription factor of the paired box family, which is necessary for normal thyroid development. In mature thyrocytes, it drives the expression of many thyroid-specific or -restricted genes such as those encoding thyroglobulin, thyroid peroxidase, and the sodium–iodide symporter. PPARγ is a transcription factor of the nuclear receptor family expressed at extremely low levels in the normal thyroid, and as of yet, it has no identified function in thyroid follicular cells (84).
The translocation fuses a truncated 3′ portion of PAX8 with the full-length PPARG (Fig. 1). Typically, the resulting transcript contains exon 10 of PAX8. However, shorter isoforms might be detected. The shorter fused transcripts can be explained by either breakpoints in other introns (introns 8 or 9) or alternative splicing that physiologically takes place while generating the PAX8 mRNA (84).
The PAX8 promoter, which is highly active in thyroid follicular cells, drives the expression of the chimeric PAX8-PPARG fusion protein (PPFP) containing the full length of PPARγ1. Microarray data from human thyroid carcinomas strongly suggest that PPFP has PPARγ-like activity in these tumors: two of the most highly expressed genes in PPFP-positive carcinomas are AQP7 and ANGPTL induced by PPARγ in adipocytes (85,86).
Oncogenic Fusions as Targets in the Management of Thyroid Malignancy
Standard therapy for thyroid cancer includes surgery followed by RAI ablation and thyrotropin suppression. Although DTC tend to respond well to this therapy, recurrent DTC are often resistant to RAI, and ATC and MTC cannot be treated with RAI (9,10). During recent years, numerous tyrosine kinase inhibitors, including multikinase and selective inhibitors, have been developed and tested in clinical trials (15,87). For patients with RAI-refractory cancer, several tyrosine kinase inhibitors have shown efficacy in improving progression-free survival and have received Food and Drug Administration approval (including sorafenib and lenvatinib for progressive DTC, and vandentanib and cabozantinib for MTC).
Identification of gene fusions in clinical practice is possible, for example, by comparative genomic hybridization (CGH) or fluorescent in situ hybridization (FISH). However, MPS has the advantage of large-scale and high-throughput fusion detection. Various next-generation sequencing approaches, such as whole-genome sequencing (WGS), whole-transcriptome (RNA-Seq) sequencing, and targeted sequencing may be used for fusion detection (22,88,89). The fusion detection capacity of the main methods is summarized in Table 2.
Asterisks indicate cost, with five being the most expensive, and one being the least.
FFPE, formalin-fixed, paraffin-embedded tissue; CGH, comparative genome hybridization; FNA, fine-needle aspiration biopsy.
WGS and RNA-seq approaches are robust instruments for the identification of novel fusions and characterization of the role of fusions in molecular pathogenesis of different types of cancers. WGS-based approaches provide comprehensive and integrative characterization of fusions. However, the significance of a fusion gene depends on the generation of a fusion transcript that is translated (88). In contrast, RNA-seq focuses only on the expressed regions of the genome, making the discovered fusions more relevant. A RNA-Seq based approach was used by Kelly et al. to identify oncogenic events in thyroid cancers with no known driver mutations and allowed a novel STRN-ALK gene fusion to be discovered (53). The drawbacks of RNA-seq include transcription-induced chimeras resulting from intergenic trans- or cis- splicing of adjacent genes, the inability to identify fusion events involving nontranscribed sequences, sensitivity to tissue specificity, and the broad dynamic range of expression in human transcriptome (20,22,88 –93). Integrative employment of WGS and RNA-seq data increases the sensitivity and specificity of fusion detection (94,95). The combination of WGS and RNA-Seq employed in the TCGA project allowed several new RET/PTC fusions to be discovered (24).
The cancer exome panel MSK-IMPACT enables most of the previously reported fusions in thyroid tumors to be detected, except NTRK1 and NTRK3. This panel is based on massively parallel exon capture approach and targets all exons and selected introns of 341 genes frequently altered in human cancer. Using MSK-IMPACT, Landa et al. characterized the genomic landscape of PDTC and ATC and identified oncogenic rearrangements, which is challenging in these tumors because of extensive tumor infiltration by macrophages, particularly in ATC (61).
Wide application of WGS and RNA-seq approaches in clinical practice is limited due to their high cost. Targeted sequencing is suitable for clinical purposes, since it combines high sensitivity, throughput, and cost effectiveness. As an example, the ThyroSeq v2 panel, which utilizes Ion AmpliSeq™ technology (Thermo Fisher Scientific) and semiconductor-based sequencing, includes 42 types of gene fusions reported in thyroid cancer, in addition to select point mutations in 14 genes (96). Another cancer panel ThyGenCap™, based on hybridization capture, targets 20 potential fusion genes in addition to somatic mutations (26).
Fusion proteins arising from oncogenic rearrangements are potential targets for the treatment of patients with advanced thyroid cancer, especially in cases of RAI resistance and metastatic disease (3,9). Patients with ATC and MTC positive for ALK fusions showed pronounced response to the crizotinib, an inhibitor of ALK (70,97). RET fusions provide a plausible target for RET tyrosine kinase inhibitor therapies, which was confirmed in the case of MTC harboring a RET rearrangement (71). However, adaptive resistance to inhibitors due to kinase domain mutations and over-activation of bypass pathways is possible (98,99). Despite these promising results, the number of successful examples of targeted therapy is very limited. This can be explained in part by the fact that MPS is not yet widely available for fusion detection in clinical practice. It is hoped that new sequencing technologies will arm clinicians with valuable tools to find targeted therapies based on individual mutation profiles of thyroid cancer.
In conclusion, gene fusions have been well characterized in different types of thyroid cancer. Some of them are cancer type specific and may be used as diagnostic and prognostic tools. Some fusions can be inhibited by targeted therapies. MPS allows efficient detection of fusions and other mutations in thyroid cancer, providing a quick and reliable instrument in clinical practice that permits better characterization of the malignancy at the molecular level.
Footnotes
Author Disclosure Statement
No competing financial interests exist.