
Abstract
Background:
BRAFV600E is the most common mutation in papillary thyroid carcinoma (PTC) and can be associated with aggressive disease. Previously, a highly sensitive blood RNA-based BRAFV600E assay was reported. The objective of this study was to assess the correlation of BRAFV600E circulating tumor RNA levels with surgical and medical treatment.
Methods:
Circulating BRAFV600E levels were assessed in (i) a murine model of undifferentiated (anaplastic) thyroid carcinoma with known BRAFV600E mutation undergoing BRAFV600E -inhibitor (BRAFi) treatment, and (ii) in 111 patients enrolled prior to thyroidectomy (n = 86) or treatment of advanced recurrent or metastatic PTC (n = 25). Blood samples were drawn for BRAFV600E analysis before and after treatment. Testing characteristics were assessed and positivity criteria optimized. Changes in blood BRAFV600E values were assessed and compared to clinical characteristics and response to therapy.
Results:
In a murine model of anaplastic thyroid carcinoma with BRAFV600E mutation, blood BRAFV600E RNA correlated with tumor volume in animals treated with BRAFi. In tissue BRAFV600E -positive (n = 36) patients undergoing initial surgery for PTC, blood BRAFV600E levels declined postoperatively (median 370.0–178.5 fg/ng; p = 0.002). In four patients with metastatic or poorly differentiated thyroid carcinoma receiving targeted therapies, blood BRAFV600E declined following therapy and corresponded with radiographic evidence of partial response or stable disease.
Conclusions:
This study shows the correlation of blood BRAFV600E levels in response to treatment in both an established animal model of thyroid cancer and in patients with BRAFV600E -positive tumors with all stages of disease. This assay represents an alternative biomarker in patients with positive thyroglobulin antibodies, and tumors, which do not express thyroglobulin.
Introduction
T
Most risk-stratification algorithms were designed to predict mortality and do not integrate mutational status. The 2009 American Thyroid Association (ATA) guidelines for the management of differentiated thyroid cancer introduced a three-tiered risk of persistent/recurrent disease following initial treatment, which was validated in a number of countries (7). In the 2015 revision of the ATA guidelines, the authors include BRAFV600E as a potential additional prognostic variable (5). BRAFV600E causes constitutive activation of the MAPK pathway and is present in more than one half of PTCs and in 5–20% of patients with poorly differentiated and anaplastic thyroid carcinomas (ATC) (8,9). The proportion of BRAFV600E -positive PTC is reportedly increasing (10). In thyroid cancer patients, this mutation is highly specific for PTC. Commercial DNA and gene expression profile assays performed on thyroid fine-needle aspirates (FNA) are highly predictive of malignancy when the BRAFV600E DNA mutation is present (11 –13). Currently, assessment of the thyroid tumor tissue for this mutation requires obtaining genetic material for mutational profiling through FNA or tissue for immunohistochemical staining with specific anti-BRAFV600E antibodies (14). Traditional tissue assays are considered less sensitive because of the potential for background tissue contamination and sampling error (i.e., testing an adjacent BRAFwt nodule) (5).
Knowing the mutation status of each tumor is important, since the mutation is associated with aggressive pathological features, local tumor recurrence, loss of radioactive iodine avidity (RAI), and increased disease-specific mortality (15 –21). Even in papillary thyroid microcarcinomas (<1 cm), aggressive features and a higher risk of recurrence are observed in patients with BRAFV600E tumors (22,23). While prophylactic central cervical lymph node dissection in patients with cytological BRAFV600E tumors is controversial, some experts recommend using BRAFV600E status to guide extent of initial surgery and use of RAI (24 –27).
Recently, the development and feasibility of a highly sensitive blood RNA-based BRAFV600E assay in patients with thyroid disease was reported (28). Circulating BRAFV600E was able to be detected in the blood of thyroid cancer patients, and a good correlation was found with conventional tissue methods. The correlation of response to treatment in patients with melanoma undergoing BRAFV600E -inhibitor (BRAFi) therapy has also been reported (5,29 –32). In patients with thyroid cancer, a liquid biopsy that can accurately measure circulating BRAFV600E levels would be beneficial at multiple levels: (i) in patients with tumor recurrences, where tissue is not easily accessible; (ii) an alternative biomarker for surveillance of those patients with thyroglobulin antibodies (TgAb); (iii) a biomarker for advanced thyroid cancer patients undergoing BRAFV600E -targeted therapies; and (iv) an alternative to Tg in patients undergoing thyroid lobectomy alone for lower-risk PTC, since the remnant gland is left in situ (5,30 –32). Compared to FNA, a routine blood draw is less expensive and less invasive. In addition, the FNA can only be done on one lesion at a time.
This work further characterized the RNA-based blood assay to see if it would allow for serial, quantitative analysis correlating with effects of treatments such as surgery or targeted therapies. In addition, BRAFV600E levels were analyzed in a murine model of undifferentiated (anaplastic) thyroid carcinoma harboring the BRAFV600E mutation during treatment with BRAFV600E inhibitors. It was hypothesized that blood BRAFV600E levels would correlate with response to treatment. Serial blood BRAFV600E levels could provide an inexpensive, safe, and simple mechanism for risk stratification and surveillance in the 50% of patients with PTC with BRAFV600E mutation, offer an alternative biomarker in in patients where Tg levels are not informative, and provide longitudinal assessment of treatment response.
Materials and Methods
Orthotopic murine model of human ATC
All animal work was done in the animal facility at Massachusetts General Hospital (Boston, MA) in accordance with federal, local, and institutional guidelines. Human ATC cells (8505c; BRAFV600E /–, TP53R248G/–; Deutsche Sammlung von Mikroorganismen und Zellkulturen) were cultured in Dulbecco's modified Eagle's medium (DMEM) supplemented with 10% fetal bovine serum and 1% penicillin/streptomycin in a 37°C 5% CO2 incubator. An orthotopic murine model of BRAFV600E -mutant ATC was chosen in order to provide proof-of-principle of the feasibility of detecting plasma BRAFV600E RNA and the ability to correlate plasma levels with tumor volume. The 8505c human ATC orthotopic severe combined immunodeficiency (SCID) model progresses at a much faster rate compared to PTC models, which lends to improved ease of use. Human ATC cells were injected into the thyroid of 33 ten-week-old female SCID mice, as previously described (33). Briefly, the mice were anesthetized, the thyroid gland exposed, and 106 8505c cells were injected into the left thyroid lobe with a 27-gauge needle. The right thyroid lobe was not manipulated to serve as an internal control. Mice were randomized to either a control diet (Research Diets, Inc.) or 418 mg/kg BRAFi (PLX4720)-embedded chow (Research Diets, Inc.) ad libitum, starting two weeks after injection (34). Three mice were euthanized weekly for assessment of tumor volume (volume = [length × width × depth]/2), and blood was obtained by cardiopuncture and pooled to yield sufficient quantity. The blood BRAFV600E level was quantified, as previously described and below (29).
Patient selection
Under approval by the Partners Human Research Committee Institutional Review Board at the Massachusetts General Hospital, patients with benign and malignant thyroid disorders undergoing initial curative surgery or treatment of recurrent disease were enrolled between September 2013 and September 2015. After informed consent, a 5 mL sample of peripheral blood was obtained from each patient before and after surgery or, in the cases of iodine-refractory metastatic disease, during treatment with targeted chemotherapies. The post-treatment blood was drawn at the time of the subsequent clinic visit, the vast majority being at the postoperative visit (median 17.5 days; interquartile range (IQR) 13.0 to 30.3 days).
Blood BRAFV600E assay protocol
The assay was previously described in detail (28,29). Briefly, peripheral blood lymphocytes were isolated by Ficoll density centrifugation from each blood sample and stored in freezing medium. RNA was isolated by the Trizol method (Invitrogen, Grand Island, NY) and (50–100 ng) reverse transcribed to cDNA by standard methods, normalized in quantity with 18S RNA, and amplified. After DNA cleanup, wild-type BRAF (BRAFwt ) was digested with TSPR1 (restriction site = NNCASTGNN; New England Biolabs, Beverly, MA) to reduce contamination by normal BRAFV600E from surrounding normal tissue in the blood samples. The product was then subjected to a second round of polymerase chain reaction (PCR) and BRAFwt digestion. To favor the mutant further over the wild-type product, a 33-fold excess of the reverse (common sequence in mutant and wild-type) to forward (exact match for mutant and one base mismatch for wild-type sequences) primers were used in the final real-time PCR assay for BRAFV600E . Oligonucleotides were custom synthesized from Invitrogen (Carlsbad, CA) and Sigma–Aldrich (St. Louis, MO). Purified BRAFV600E first-round PCR product with a known concentration was also run through the assay and was used to create a standard curve.
It was previously established that the assay can detect as low as 1 pg of BRAFV600E and has a 1000-fold increased sensitivity compared to the BRAFwt (28). This assay was used for the orthotopic murine model (discussed above), reported in pictograms, with a positivity criterion of 4.8 pg. The 18S reverse transcription PCR assay is now run in the presence of known amounts of purified RNA in order to generate a standard curve (input RNA in nanograms). Going forward, all new data generated by this assay will be reported as femtograms of BRAFV600E /nanogram of RNA.
Tissue-based BRAFV600E analysis
Tissue-based BRAFV600E analysis has been previously described (28). Briefly, patients meeting inclusion criteria and with tissue available had BRAFV600E mutational analysis as part of standard clinical care either via SNaPshot (Massachusetts General Hospital Cancer Center Translational Research Laboratory) or immunohistochemistry was done using a BRAFV600E monoclonal antibody with 97% correlation with SNaPshot molecular testing (98% sensitivity and 97% specificity) (35). For PTC cases in which mutational status was not obtained clinically, BRAFV600E mutation was sequenced from formalin-fixed, paraffin-embedded (FFPE) tissue blocks, as previously described.
Tg assay
A commercial assay (Mayo Medical Laboratories New England, MA) was used to determine Tg levels in all patients, as per standard clinical practice.
Statistical analysis
Clinical variables were chosen based on established demographic and pathological risk factors for decreased thyroid cancer-free survival. The American Joint Committee on Cancer TNM (AJCC TNM) stage was determined for each patient. For comparisons between BRAFV600E and wild-type groups, pathological variables were only considered present if they were specifically described in the final pathology report (as per convention). Univariate comparisons of categorical variables were analyzed using Fisher's exact test, and continuous variables were assessed by Student's t-test or Wilcoxon's rank-sum test for nonparametric data. Correlations of postsurgical blood BRAFV600E expression levels according to mutational status and demographic and pathological characteristics were based on linear regression models. A p-value of <0.05 was considered statistically significant. Using tissue results as the gold standard, likelihood ratios (sensitivity/1 – specificity) were calculated, and a receiver operating characteristic curve was produced. An a priori decision was made to maximize specificity for determining the positivity criterion. Blood BRAFV600E levels before and after surgery were compared, and Wilcoxon's signed rank test was carried out to assess the non-normal blood BRAFV600E level change before and after surgery for tissue BRAFV600E -positive and tissue BRAFwt patients, respectively.
Results
Circulating BRAFV600E levels correlate with tumor response after treatment with BRAFi in an orthotopic murine model of ATC
The previously described immunocompromised orthotopic mouse model of ATC was utilized to study the correlation between BRAFV600E tumor growth and BRAFV600E levels both before and following treatment with the selective BRAFi (PLX4720) (33). This model results in tumor growth with extrathyroidal extension over several weeks and cervical lymph node and pulmonary metastases; control animals have a life expectancy of up to five weeks.
A total of 33 mice had orthotopic injection of 8505c cells (Fig. 1). Three mice were euthanized weekly to evaluate mean tumor volumes, and their blood was pooled to obtain sufficient peripheral blood leukocytes for RNA-based BRAFV600E analysis. Two days after implantation of tumor, mouse blood BRAFV600E levels were 16.17 pg and steadily rose such that at two weeks post implantation, mice had a peak BRAFV600E RNA level of 40.8 pg in the pooled blood and a mean tumor volume of 12.0 ± 0.6 mm3. Subsequently, mice were randomized to either control chow or treatment with BRAFi embedded chow at a standard dose (418 mg/kg BRAFi). Over the next set of measurements, tumor volume rose steadily to a peak of 118.6 ± 26.1 mm3 at four weeks in the control group, consistent with previously reported data. Blood BRAFV600E levels remained elevated at each weekly time point (34). During the third week post implantation, the BRAFV600E blood level dipped slightly to 22.01 pg and remained stable at four weeks. The control mice had to be euthanized at the beginning of week 5 post implantation in order to meet humane endpoints. In the BRAFi-treated group, tumor volume declined to 7.11 ± 1.0 mm3 and 2.53 ± 2.7 mm3 at weeks 3 and 4, respectively. Tumors subsequently became and remained undetectable. Mean blood BRAFV600E RNA declined in tandem with tumor volume to 2.1 pg and 4.0 pg at weeks 3 and 4, respectively, and remained between 1.5 pg and 2.8 pg through week 8 of the study.

BRAFV600E -mutated thyroid tumors grow in the first two weeks after orthotopic tumor implantation. Blood BRAFV600E levels also increase. Treatment with BRAFi (PLX4720) prevents tumor progression and dramatically reduces blood BRAFV600E levels.
Patient cohort characteristics
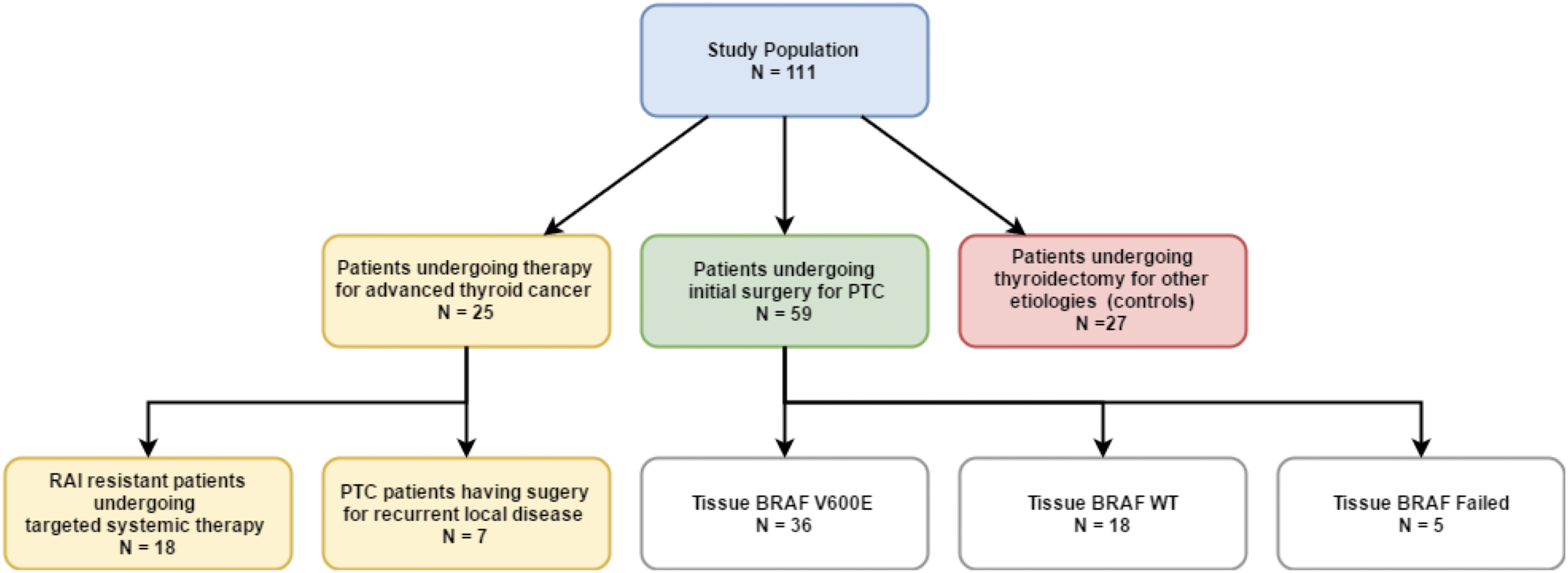
The goal was to analyze this assay in a variety of thyroid cancer patients to understand assay utility fully. The study population included 111 patients who had their blood BRAFV600E level measured before and after surgery or adjuvant therapy (Fig. 2). Of the 111 patients, 25 were undergoing advanced thyroid cancer therapy, including seven PTC patients who had surgery for recurrent local disease and 18 patients with RAI-resistant differentiated, poorly differentiated, or ATC undergoing active surveillance, or systemic therapy with small molecule inhibitors or, in the case of ATC, cytotoxic chemotherapy and radiotherapy. Fifty-nine patients underwent initial surgical treatment with curative intent for PTC, 51 (94.4%) of whom underwent at least total thyroidectomy. In this group, 36 patients had tumor tissue harboring the BRAFV600E mutation, whereas 18 patients had tumor tissue with BRAFwt . In five patients, the assay failed (n = 1) or BRAFV600E testing was not performed. An additional 27 patients were recruited as controls, and their surgical pathology diagnoses were multinodular goiter (n = 23) and follicular adenoma (n = 4). None of the patients had known melanoma or colorectal adenocarcinoma. Patients with cancer had AJCC TNM stages I–IV (Table 1).
Patient cohort and associated therapy.
PTC, papillary thyroid carcinoma; wt, wild type; SD, standard deviation; AJCC TNM, American Joint Committee of Cancer Tumor, Node, Metastasis; IQR, interquartile range.
Testing characteristics
To compare the blood BRAFV600E assay results with the conventional tissue testing, the results of the optimized blood assay were compared to conventional tissue mutational testing using the group of patients undergoing initial surgery for curative intent in which tissue genotyping was available. Using the tissue BRAFV600E result as the gold standard, likelihood ratios were calculated and a receiver operating characteristic curve for the blood assay predicting tissue BRAFV600E mutational status was constructed (Fig. 3). The area under the curve (AUC) was 0.68, indicating moderate correlation of tests assuming the tissue results are true. Using maximum likelihood ratio for a positive test (LR+) as the optimal cutoff, the threshold for blood BRAFV600E level is 140–145 fg/ng RNA.

Receiver operating characteristic curve based on 54 patients receiving initial papillary thyroid carcinoma therapy who have tissue BRAFV600E status.
Blood BRAFV600E levels decline following initial surgical treatment for PTC
Preoperative blood BRAFV600E levels were assessed for association with clinical and pathological characteristics. On multivariable linear regression, adjusting for sex, age, and tumor volume, only extrathyroidal extension was correlated with the preoperative blood BRAFV600E level (p = 0.03). The blood BRAFV600E levels were compared before and after initial surgical treatment for PTC patients stratified by their tissue BRAFV600E status (Fig. 4). For tissue BRAFV600E -positive patients (n = 36), the median blood BRAFV600E level dropped from 370.0 fg/ng RNA to 178.5 fg/ng RNA (p = 0.002). For tissue BRAFwt (n = 18) and for non-PTC controls with tissue BRAFwt (n = 15), the median blood BRAFV600E level did not change significantly with surgery (p = 0.70 and p = 0.69, respectively). Three of these patients for whom blood BRAFV600E levels were available before and after initial surgery for curative intent had a structural recurrence requiring surgery during the study period, all of whom were tissue BRAFV600E positive. Blood BRAFV600E levels correlated with clinical disease status in the two patients with high preoperative levels. In one patient, the preoperative BRAFV600E level of 3567 fg/ng RNA fell to139 fg/ng (Tg 8.8 ng/mL), below the established threshold, at six months postoperatively. With the development of recurrent clinical nodal disease six months later, the BRAFV600E level had increased to 316 fg/ng RNA and correlated with an increase in the Tg level, indicating recurrence (Tg level 54 ng/mL). To see whether serum thyrotropin (TSH) levels influenced blood BRAFV600E levels, the length of the time lapse between collection of the blood BRAFV600E levels, tissue BRAFV600E levels, and the recorded TSH were adjusted, and no significant association was found between blood BRAFV600E levels and TSH levels following surgery (data not shown). The effect between postoperational serum BRAFV600E level and the time between surgery and measurement was also tested (median 17.5 days; IQR 13.0 to 30.3 days), adjusting for preoperative blood BRAFV600E levels and tissue BRAF status in a linear regression model, and there was no significant association (p = 0.328).

Comparison of blood BRAFV600E level (log10 scale) before and after initial surgical treatment among tissue BRAFV600E-positive and BRAFwt patients. The box plots measure 1st quartile −1.5 interquartile range (IQR), 1st quartile, median, 3rd quartile, 3rd quartile +1.5 IQR from bottom to top.
Blood BRAFV600E levels before and after surgical treatment for locally recurrent PTC
Seven patients in the cohort had remote thyroidectomy with or without cervical lymph node dissection. Five of the patients had tumor tissue positive for BRAFV600E , one in the index tumor and four in the recurrent tumors. Blood BRAFV600E was obtained before and after surgery to characterize recurrent local disease. Median blood BRAFV600E before and after salvage surgery was 319.0 fg/ng RNA (IQR 192.5–562.6 fg/ng) and 260 fg/ng RNA (IQR 109.0–491.0fg/ng). In one patient, clinical recurrence occurred one year following initial total thyroidectomy with central lymph node dissection for a tall-cell variant PTC with a small focus of ATC. The preoperative BRAFV600E level was 1193 fg/ng. While two weeks following salvage surgery this level failed to decline (2163 fg/ng), after external beam radiation, the level decreased to 598 fg/ng RNA. Six months following this, the level returned to 2104 fg/ng RNA, which was concerning for worsening disease. The patient has a new thyroid bed mass that is being observed (based on the patient's age and choice), which is consistent with the observed elevation in BRAFV600E levels. Throughout the clinical course, Tg levels have been very low to undetectable (0.1–0.3 ng/mL). Two other patients in this group had elevated TgAb.
Blood BRAFV600E levels before and after initiation of targeted therapies
Blood BRAFV600E samples were obtained from 18 patients with metastatic RAI-resistant papillary (n = 11) poorly-differentiated/anaplastic (n = 5), and Hürthle cell (n = 2) thyroid carcinomas undergoing active surveillance, or receiving chemotherapy, radiotherapy, multikinase inhibitors, and/or MAP-kinase pathway-specific inhibitors. Fourteen of the patients had BRAFV600E -mutant tumors, and all 18 had detectable levels of BRAFV600E in their blood (median 615 fg/ng; range 41–6552 fg/ng). Six patients (five BRAFV600E -positive PTC and one with poorly differentiated thyroid carcinoma [BRAFV600E positive]) did not have an alternative means of biochemical monitoring due to lack of Tg production (Tg <1 ng/mL; n = 4) or because of elevated TgAb (n = 2). Five of these six patients without other means of biochemical monitoring had gross elevations in pretreatment blood BRAFV600E levels (range 552–6552 fg/ng) that dropped following systemic therapy initiation (range of log2 [fold change] of 0.76–4.91). Correlation between blood BRAFV600E and treatment response per RECIST v 1.1 was most notable in patients receiving BRAFV600E inhibitors alone or in combination with MEK inhibitors (Fig. 5). In this subset of four patients, blood BRAFV600E levels declined dramatically following initiation of therapy and corresponded with radiographic evidence of partial response or stable disease. In three of these patients, blood BRAFV600E increased from the nadir, one of whom developed progressive disease 13 months after this increase, while the two other patients continued to have stable disease.

Circulating levels of BRAFV600E in four patients with radioiodine-refractory metastatic BRAFV600E -positive thyroid cancer undergoing targeted therapy. BRAFi, dabrafenib or vemurafenib; MEKi, trametinib.
Discussion
Thyroid cancer has been increasing in incidence more than any other cancer in the past few decades. While the majority of the increase is attributed to small, seemingly indolent cancers, a recent report also shows an increase in higher-staged tumors and disease-specific mortality (3). With recent changes in guidelines toward less aggressive treatment, improved risk stratification for thyroid cancer patients is essential (5). Additionally, the standard circulating biomarker, Tg, is unreliable in the subset of patients who progress to aggressive disease and whose tumors no longer make Tg, as well as in patients with TgAb that interfere with measurement of Tg. Thus, alternative biomarkers are needed.
Approximately half of patients with PTC harbor a BRAFV600E mutation, a proportion that may be growing, at least in North America, with the reclassification of RAS-mutant (BRAFwt ) noninvasive encapsulated follicular-variant PTC to noninvasive follicular thyroid neoplasm with papillary-like nuclear features (36). Large controlled studies have shown a correlation between this mutation and aggressive tumor characteristics, tumor recurrence, and overall survival particularly in the presence of other mutations such as TERT (15,17,18,37). Knowledge of BRAFV600E status may be helpful in diagnosis (nearly 100% positive predictive value for PTC); determining extent of surgery (lobectomy vs. total thyroidectomy ± level VI cervical lymph node dissection), use of RAI, and frequency and intensity of follow-up; as an alternative to Tg in Tg-negative or TgAb-positive patients; and to assess response to BRAFi therapy in patients with advanced disease. Conventionally, cytology or surgical pathology specimens have been utilized to ascertain BRAFV600E mutational status. The feasibility of a sensitive RNA-based blood assay to detect and serially monitor BRAFV600E levels in patients with PTC has been published previously (28).
A key potential advantage of the assay is to serve as an alternative biomarker in patients with anti-TgAb, present in a significant proportion of PTC patients, and in the subset of patients whose tumors stop producing Tg because of disease dedifferentiation (38). Indeed, 12/59 (20%) patients undergoing initial surgery for PTC in this study had TgAb noted postoperatively, making Tg levels useless. Of these 12, nine were positive for BRAFV600E on tissue testing. Indeed, in 6/18 patients with advanced thyroid cancer, the BRAFV600E levels were elevated in the setting of very low or absent Tg <1.0 ng/mL and/or anti-TgAb (n = 2). Moreover, in the small but substantial group of patients destined to do poorly, there is an enrichment of BRAFV600E mutations. Thus, the ability to detect and follow BRAFV600E levels accurately over time as a biomarker for recurrence and response to BRAFi would be of great clinical value.
This work shows the correlation of blood BRAFV600E levels in response to treatment both in an established animal model of thyroid cancer and in BRAFV600E patients with all stages of disease undergoing treatment. In both the orthotopic murine model and in the patients, blood BRAFV600E levels were not associated with tumor size, TSH level, Tg levels, or time of blood draw. In fact, the only clinical or pathological factor correlating with BRAFV600E levels in the patient cohort was extrathyroidal extension. It was found in general that blood BRAFV600E levels were detectable in all stages of disease and responded to both surgical therapy and treatment with systemic targeted therapy.
It was observed that plasma BRAFV600E RNA levels spontaneously dropped in control mice that did not receive PLX4720 at week 3, albeit to a much lesser extent compared to mice that received treatment. The reasons for this decline (and subsequent rise) are unclear but may be due to the complex dynamic relationship between circulating tumor cells/nucleic acids and the originating tumor volume. In the 8505C orthotopic SCID ATC model, weeks 2–3 coincide with the exponential growth of thyroid tumor volume (in this experiment, mean tumor volume increased from 12.0 mm3 to 68.9 mm3) and the emergence of pulmonary micrometastases. In a review of the primary data, the subsequent rise in BRAF-mutant RNA at week 4 is largely driven by higher levels of the fourth mouse with a small tumor whose blood was analyzed separately. This was included at the four-week time point by taking a mean with a weighted mean of the pooled mice (n = 3). If this mouse is excluded from the analysis, the decline continues to occur. The outlier was included for completeness. Although not specifically shown for circulating tumor RNA, a spontaneous decrease in circulating tumor cells has been reported in the literature, especially during a period of rapid tumor growth following a period of slower growth (39 –41). A spontaneous decline and then subsequent rise has also been reported, especially for larger tumors. There are several postulated mechanisms for this phenomenon that remain unproven. One such mechanism includes the activation of host immunity by increasing single or clustered circulating tumor cells and subsequent enhanced clearance, although this immune activation is not enough to penetrate and/or clear the primary solid tumor or metastases, which are associated with an immunosuppressive microenvironment. While one might expect this phenomenon to be dampened in SCID mice, they do retain functional phagocytes such as neutrophils and monocytes/macrophages, which may be contributory to clearance. Additionally, rapid tumor growth may be associated with changes in tumor vessel morphology and function and tumor cell apoptosis/necroptosis; it is conceivable that these variables might decrease the efflux of circulating tumor cells.
Limitations of our study are acknowledged. There is some baseline signal in both BRAFwt patients and patients undergoing thyroidectomy for benign disease. Using tissue BRAFV600E status of the dominant tumor as the reference may be a source of potential error, given that PTC is commonly multifocal, with some carcinomas harboring BRAFV600E mutations and others that do not. It is possible that the larger, dominant nodule undergoing tissue testing may be BRAFwt while other, potentially smaller, carcinomas (which may shed BRAFV600E into the blood) may not have been tested. Another possible explanation is that there is a small volume of BRAF-mutant cells in the thyroid neoplasm that was not identified, since it was below the level of detection of the BRAF tissue testing. The blood test may be more sensitive than tissue testing. However, this is impossible to prove without testing at the tissue level (although testing at the tissue level may be limited by heterogeneity between different lesions, as discussed above). Additionally, the possibility cannot be entirely excluded that detectable circulating levels of BRAFV600E are from an undiagnosed BRAFV600E mutant malignancy (e.g., melanoma or colorectal adenocarcinoma), although there was no clinical documentation of such in the cohort. None of these patients has declared themselves with a secondary malignancy thus far, although small PTC can be indolent. Lastly, it is also possible that there is a false-positivity rate or noise with the assay at low or absent BRAFV600E concentrations that will not be overcome until technical and analytical validation is formally completed, which is the subject of ongoing work. As with other biochemical assays, a functional sensitivity threshold will need to be established. The change from before to after treatment will likely be the most useful metric to follow.
Recently, several commercial BRAFV600E assays, originally designed for and validated on FFPE samples, have been investigated for use with circulating tumor DNA isolated from the blood of patients with melanoma, including the PrimePCR™ ddPCR™ BRAFV600E pV600E Mutation Assay (Bio-Rad, Hercules, CA), the therascreen CRGQ PCR Kit (Qiagen, Hilden, Germany), the Idylla™ BRAFV600E mutation test (Biocartis, Mechelen, Belgium), the PNA Clamp™ BRAFV600E Mutation Detection Kit (Panagene, Daejeon, Korea), and the ctBRAFV600E Mutation Detection Kit (Entrogen, Woodland Hills, CA) (42 –48). Kim et al. (45) were the first to adopt the use of the TaqMan® (castPCR™) BRAFV600E Mutation Detection Assay (Life Technologies, Carlsbad, CA) in the plasma of patients with PTC. The present assay detects BRAFV600E amid excess wild-type BRAF with high sensitivity (28,29). The use of RNA with exponentially higher copy numbers of BRAFV600E mRNA as well as digestion of BRAFwt enhances the sensitivity of the assay, which is a potential advantage over the DNA-based techniques described above.
Blood-based BRAFV600E detection has several clinical applications. Unlike tissue mutational testing, in which results are qualitative and binary, this assay allows quantitative, serial measurements of circulating BRAFV600E , and levels are responsive to treatment. The ability to test circulating BRAFV600E levels during treatment with BRAFi and other targeted therapies to assess response to treatment and prediction of re-differentiation would be of great value in guiding therapy. Recent work has shown the BRAFi (dabrafenib) treatment in RAI-refractory patients can lead to re-differentiation and subsequent RAI uptake in some tumor lesions (32). Partial response was also seen in a Phase II trial with the BRAFi vemurafenib in 10/26 patients with metastatic or unresectable RAI-refractory PTC (49). More recent work in two other Phase II trials using combinations of BRAFi and MEKi has shown high response rates in BRAFV600E RAI refractory PTC and BRAFV600E ATC patients (50,51), and one Phase I trial of dabrafenib and LAP was well tolerated in BRAFV600E thyroid cancer patients (52). The ability to test circulating BRAFV600E levels during treatment with BRAFi to assess response to treatment (surgical, RAI, and systemic therapy) and as an early marker of recurrence could be of great value.
In summary, this study reports the correlation of RNA blood BRAFV600E levels with surgical and medical management of patients with PTC. This builds on prior work showing that the assay has good correlation (AUC 0.71) with tissue BRAFV600E testing (28). In a murine model of BRAFV600E -mutant ATC, blood BRAFV600E levels correlate with tumor volume in animals and correlate with clinical response to BRAFi. The study also reports a significant decline in levels following initial surgery for curative intent. While it is challenging to make conclusions in the heterogeneous population of patients with metastatic or poorly differentiated thyroid carcinomas receiving targeted therapies, a subset of patients was found who showed a decline in blood BRAFV600E levels following therapy that corresponded with radiographic evidence of partial response or stable disease. It is possible that this blood assay may work best for patients with BRAFV600E -mutated tumors who have high baseline levels and are undergoing specific targeted therapies that work on reducing MAPK signaling. This assay represents an alternative biomarker in patients with anti-TgAb, and tumors, which do not express Tg. This is important, since no other biomarker exists for this group of patients and standard radiologic means of measuring tumor responses such as RECIST are less reliable in thyroid cancer. Finding a reliable assay that can provide early information into the therapeutic effect at the tumor cell level by measuring the RNA expression of the tumor cells in the blood can be an important tool that the medical oncologists can use to gauge a response to a targeted therapy.
Footnotes
Acknowledgments
This work was supported by the following: National Institutes of Health/National Cancer Institute Grant CA177900, The Claflin Foundation at Massachusetts General Hospital, and American Thyroid Association/ThyCa Research Grant (C.L.); The NIH National Cancer Institute (R01CA149738-01A1), Ruane Fund for Thyroid Cancer Research (S.P.); Conquer Cancer Foundation and the Clinical Investigator Training Program, Harvard Medical School and Massachusetts Institute of Technology (R.S). National Institutes of Health—Training Program in Endocrinology (5T32DK00702842; B.G.).
Author Disclosure Statement
The authors declare no potential conflicts of interest.