
Abstract
Background:
Lymph node (LN) yield and ratio are considered important predictors of post-treatment outcomes for several human cancers. This study examined the association between nodal factors, including the LN yield and ratio, with recurrence after thyroidectomy plus central compartment neck dissection (ND) for papillary thyroid carcinoma (PTC).
Materials and Methods:
This retrospective study involved 2384 consecutive patients who underwent a thyroidectomy plus central compartment ND combined with (n = 440) or without lateral compartment ND at the authors' tertiary referral center between 2006 and 2012. The number of harvested LNs, as well as other tumor and nodal findings, were carefully reviewed. Univariable and multivariable Cox proportional hazards regression models were conducted to predict recurrence and its association with clinicopathologic variables.
Results:
All nodal factors, including the positive number of LNs, ratio, and extranodal extension, were significantly associated with nodal and any-site recurrence after thyroidectomy, as well as the tumor size and multifocality (p < 0.01). The multivariable analysis showed that tumor size, multifocality, LN ratio, and extranodal extension were independent factors predictive of post-treatment recurrence (p < 0.05). The LN yield was higher in patients with nodal recurrence but did not significantly affect the nodal recurrence. Patients with a LN ratio >0.3 exhibited a 1.7-fold higher risk of post-treatment nodal recurrence than their counterparts (p < 0.01).
Conclusions:
LN ratio is an independent determinant predictive of nodal and any-site recurrence following thyroidectomy for PTC.
Introduction
A
Nodal factors of clinical detection, metastatic LN size (>3 cm), and the number of metastatic LNs (>5) have been incorporated as modifiers of the N1 category to improve estimation of the risk of recurrence (7,8). Additionally, the size and number of metastatic LNs have been included in the risk-stratification system of structural disease recurrence recently proposed by the American Thyroid Association (ATA) (4). Furthermore, a recent study suggested that the risk estimates for PTC obtained by assessing the adequacy of the LN yield (the total number of harvested LNs) provide an excellent guide for determining the risk of occult metastasis, as well as the need for post-thyroidectomy adjuvants and close surveillance (9). The presence and number of cervical LN metastases are associated with reduced overall survival (OS) in PTC patients, even in patients <45 years of age (10). In addition, a higher neck LN yield is associated with lower rates of neck recurrence in PTC patients (11). Furthermore, the LN ratio is reportedly a strong indicator of recurrence following initial surgery (12). Indeed, one study reported that patients with a LN ratio >0.3 have a 3.4-fold increased risk of persistent or recurrent disease (13). However, neither the absolute number of metastatic LNs nor the percentage of metastatic LNs removed was found to be associated with OS among the N1 patients from the Surveillance, Epidemiology, and End Results (SEER) database, which analyzed 9926 patients with differentiated thyroid cancer (14).
Although the prognostic significance of nodal factors has been examined, further studies are required to elucidate the association between nodal factors and post-treatment recurrence, as well as survival in PTC patients. Therefore, this study examined the association of nodal factors, including LN yield and ratio, with recurrence after thyroidectomy plus central compartment ND for the treatment of PTC.
Materials and Methods
Study patients
This retrospective study involved 2384 consecutive patients who underwent thyroidectomy plus central compartment ND combined with or without lateral compartment ND in the authors' tertiary referral center between 2006 and 2012. Inclusion criteria were patients with pathologically confirmed therapy-naïve PTC and surgery with thyroidectomy and central compartment ND with or without lateral compartment ND. Exclusion criteria were a follow-up period of less than two years, a prior history of treatment for PTC, diagnosis with another type of cancer at the time of the diagnosis, and a previous history of radiation therapy. The patients with no ND or a ND that did not yield more than one LN were also excluded. Primary tumors and any suspicious metastatic LN were examined in all patients using preoperative high-resolution ultrasonography (US) and US-guided fine-needle aspiration biopsy. This study was approved by the Institutional Review Board, and informed consent from each patient was waived.
Treatment and follow-up
All patients underwent a complete resection of the tumor and central compartment LN dissection. Therapeutic central and lateral LN dissection was performed in all patients suspected of having metastatic LNs in the central and lateral neck compartments. Prophylactic central LN dissection was commonly performed in the central compartment (neck level VI) in accordance with institutional protocol, regardless of clinical evidence of LN metastasis. Lateral LN dissection was performed in the neck level Ib–V or II–IV of the patients with clinical evidence of LN metastasis in the lateral neck. Most patients with total thyroidectomy received postoperative radioactive iodine (RAI) ablation according to the individual characteristics of the patient indicated by the previous ATA guidelines (15).
All surgical thyroid and metastatic LN specimens were carefully reviewed by experienced surgeons and pathologists. The patients were followed up every three months during the first year and at yearly intervals thereafter. The patients received regular examinations for clinical, neck US, chest radiography, whole-body iodine scanning, and the measurement of serum-free thyroxine and thyrotropin, thyroglobulin (Tg), and anti-Tg antibody concentrations (16,17). Any lesion suspicious for recurrence was evaluated with fine-needle aspiration cytology and imaging modalities, regardless of whether the serum Tg levels were elevated. Structural recurrence was determined by imaging modalities using US, contrast-enhanced computed tomography (CT), and/or whole-body nuclear scanning with RAI and 18F-fluorodeoxyglucose positron emission tomography, followed by histological examinations of recurrent tumors (4,18).
Most patients with structural recurrence received the additional surgery and patients with unresectable or distant metastatic PTC received RAI therapy (15). A few patients with iodine-refractory recurrent PTC received therapy using tyrosine kinase inhibitors (e.g., sorafenib or vemurafenib) (19).
Statistical analysis
Descriptive statistics were used to summarize the study data. Continuous variables were expressed as the median and range, and categorical variables as a number and percentage. Recurrence was the primary endpoint because the index cancer-specific and all-causing mortality occurred in <1% of all study patients. Any-site and nodal recurrence-free survival (RFS) was defined as the time from surgery until the first evidence of any-site and nodal recurrences, respectively. A univariate Cox proportional hazards model was used to analyze the relationship between clinicopathologic variables and RFS. Multivariate Cox proportional hazards regression analyses were performed with backward elimination, including variables with p-values <0.05 in the univariate analyses. The estimated hazard ratios (HR) and confidence intervals (CI) were calculated. The survival curves for the LN ratio were depicted after adjusting for the significant clinicopathologic factors in the univariate analyses. A two-sided p-value of <0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics for Windows v23.0 (IBM Corp., Armonk, NY).
Results
Patient characteristics
The study population is shown in a flow chart (Supplementary Fig. S1; Supplementary Data are available online at
The study patients consisted of 495 men and 1889 women with a median age of 52 years (range 12 − 86 years). Table 1 presents the clinicopathologic characteristics of the study patients summarized with a comparison between patients with and without post-treatment nodal recurrence. A tumor size >2 cm was observed in 381 (16.0%) patients. Multifocality, bilaterality, extrathyroidal extension, and a positive resection margin were detected in 802 (33.6%), 558 (23.4%), 1268 (53.2%), and 376 (15.8%) patients, respectively. Prophylactic central LN dissection was performed in 1906 (79.9%) patients without evidence of metastatic LN on preoperative US or CT. A total of 478 (20.1%) patients with clinical evidence of metastatic central LN underwent therapeutic central LN dissection. Of 2384 study patients, 440 (18.4%) patients underwent thyroidectomy plus central and lateral compartment ND (LND): unilateral LND in 403 patients and bilateral LND in 37 patients. The overall rate of central LN metastases was 40.1%. The median (range) numbers of harvested and positive LNs were 10 (2–168) and 1 (0–50), respectively: in central LN dissection alone, 8 (2–48) and 1 (0–21), respectively; and in central plus lateral LN dissection, 43 (6–168) and 8 (2–50), respectively. A total number of more than five harvested LNs was achieved in 1783/1944 (91.7%) patients in central LN dissection alone, and >18 LN were removed in 406/440 (92.3%) patients with central plus lateral LN dissection. A LN ratio >0.3 and extranodal extension were observed in 564 (23.7%) and 370 (15.5%) patients, respectively. Postoperatively, temporary and permanent vocal fold paralysis were observed in 19 (0.8%) and 3 (0.1%) patients (without preoperative paralysis), respectively; temporary and permanent hypoparathyroidism were observed in 394 (16.5%) and 33 (1.4%), respectively.
Microscopic findings.
Of 83 patients with lateral neck recurrence, 41 (49.4%) underwent lateral compartment LN dissection at initial surgery.
LN, lymph node; MACIS score, distant metastasis, patient age, completeness of resection, local invasion, and tumor size score; ND, neck dissection; RAI, radioactive iodine.
Of the total 2384 patients included in this study, 116 (4.9%) experienced any-site recurrence, and 95 (4.0%) developed nodal recurrences in central or lateral compartments. During the median follow-up of 94 months (range 24–131 years), cancer-related death occurred in only nine (0.4%) patients, and 19 (0.8%) cases involved deaths due to other causes. The nine patients with index cancer-related death are summarized in Supplementary Table S1.
Risk factors for nodal and any-site recurrence following thyroidectomy
The univariate analyses showed that male sex, tumor size >2 cm, multifocality, extrathyroidal extension, positive resection margin, therapeutic central and lateral ND, pathological central and lateral neck LN metastasis (pN1a and pN1b), number of LNs harvested, number of involved LNs, LN ratio, extranodal extension, and an MACIS score >6 were significantly associated with nodal or any-site RFS outcome (Table 2). For nodal recurrence, the multivariate analyses revealed that tumor size >2 cm (HR = 1.70 [CI 1.08–2.68]; p = 0.022), tumor multifocality (HR = 1.89 [CI 1.24–2.87]; p = 0.003), a LN ratio >0.3 (HR = 1.76 [CI 1.10–2.82]; p = 0.019), and extranodal extension (HR = 1.90 [CI 1.17–3.11]; p = 0.010) were the independent variables for nodal RFS outcomes (Table 3). For any-site recurrence, the multivariate analyses showed that a tumor size >2 cm (HR = 1.70 [CI 1.15–2.52]; p = 0.008), tumor multifocality (HR = 1.55 [CI 1.08–2.23]; p = 0.018), pN1b (HR = 3.78 [CI 1.68–8.47]; p = 0.001), LN ratio >0.3 (HR = 1.70 [CI 1.12–2.58]; p = 0.012), and extranodal extension (HR = 2.21 [CI 1.45–3.38]; p < 0.001), and MACIS >6 (HR = 1.63 [CI 1.08–2.43]; p = 0.019) were independent variables for any-site RFS outcomes. Figure 1 presents the adjusted nodal and any-site RFS probabilities for PTC patients stratified by LN ratio.
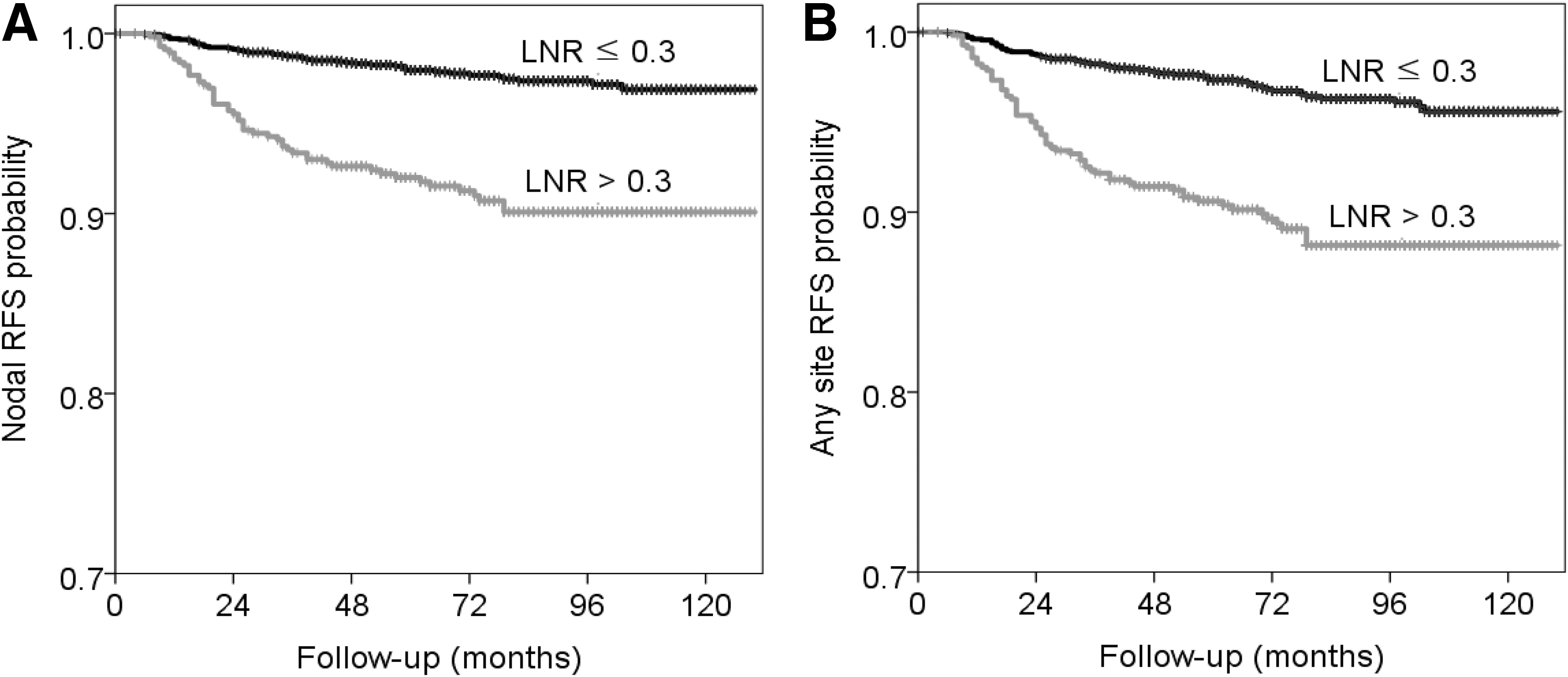
Adjusted recurrence-free survival (RFS) probability for papillary thyroid cancer patients stratified according to the lymph node ratio (LNR). Survival curve adjusted for age, sex, tumor multifocality and extension, margins, lymph node metastasis, and extranodal extension. (
Cox proportional regression analyses, p-values <0.05.
Microscopic findings.
CI, confidence interval; HR, hazard ratio.
Cox proportional hazard regression analyses were performed using a backward elimination of variables with p-values <0.05 according to the univariate analyses.
pN1b, pathological lateral neck LN metastasis.
The LN yield and number of positive LNs were further analyzed in a fashion of increasing categorization of their values (Supplementary Table S2). A LN yield >18 was significantly associated with poor nodal and any-site RFS outcomes (p < 0.001), but the LN yields 0–6, 7–12, and 13–18 did not significantly differ (p > 0.05). The number of positive LNs were significantly associated with poorer nodal and any-site RFS outcomes than no positive LNs in an increasing trend of their HRs and CIs when the numbers were categorized as 0, 1–5, 6–10, and >10 (p < 0.005). The 10-year any-site recurrence rates of 0, 1–5, 6–10, and >10 positive LNs were 1.2%, 5.4%, 12.9%, and 27.7%, respectively (p < 0.001). There was a significant correlation between the LN yield and number of positive LNs (Pearson's correlation coefficient = 0.735; p < 0.001). Because the LN yield was significantly higher in the central plus lateral LN dissection than the central LN dissection alone (t-test; p < 0.001), the LN yield and number of positive LN were stratified with central LN dissection alone versus central plus lateral LN dissection. After adjustment with the presence of lateral compartment LN dissection, the LN yield and number of positive LNs were significantly associated with poor nodal and any-site RFS outcomes (p < 0.05). However, after adjustment of all variables significant on univariate analyses, only LN ratio >0.3 but not the LN yield or number of positive LNs remained the independent variable of nodal and any-site recurrence. The 10-year nodal recurrence rates of the categories were 0.8%, 3.6%, 11.7%, and 22.8%, respectively (p < 0.001). Figure 2 shows the adjusted nodal and any-site RFS probabilities for the categorized LN yield and number of positive LNs. The distribution of the LN yield according to the performance of lateral neck compartment dissection is shown in Supplementary Figure S2.
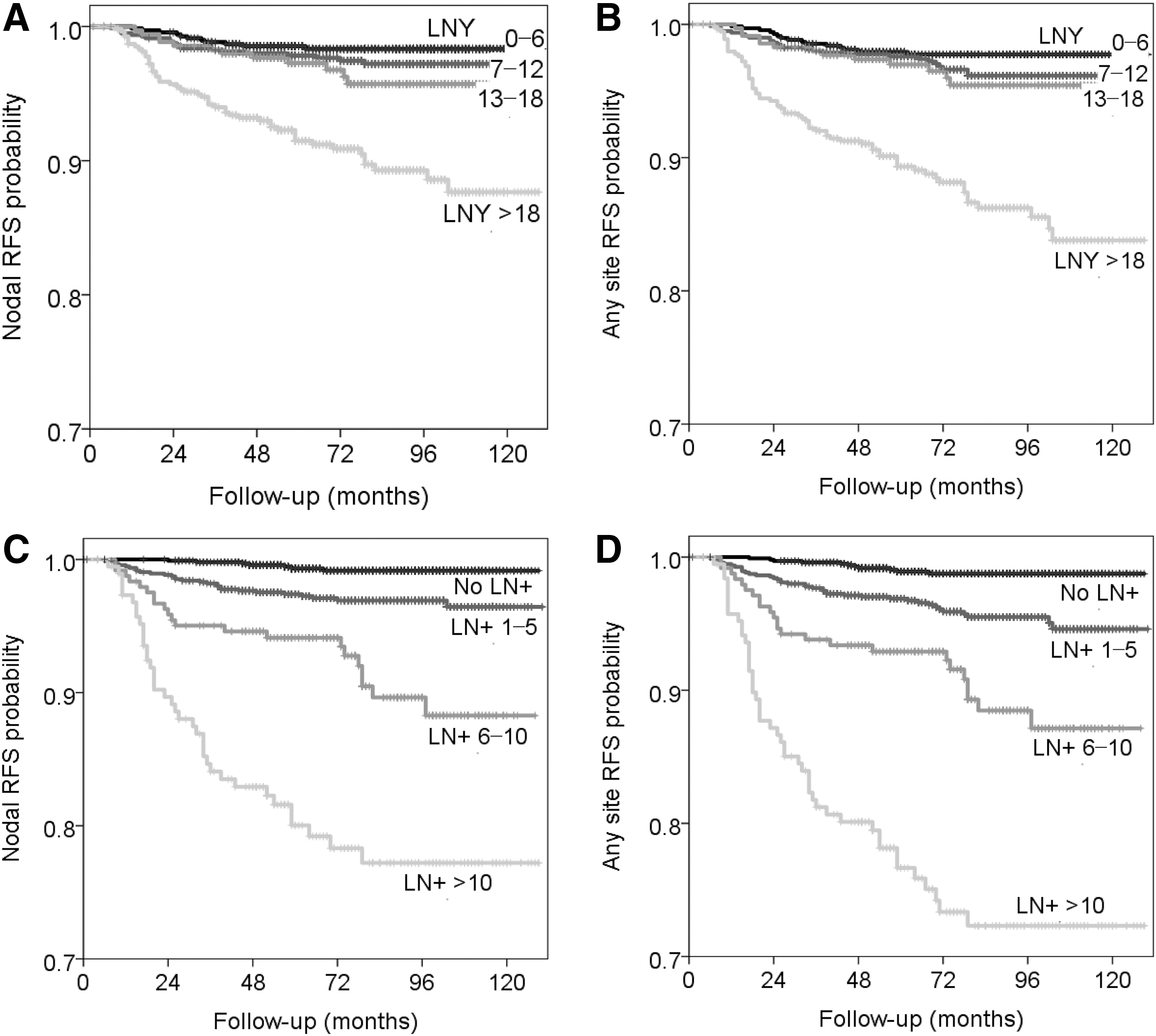
Adjusted probability of RFS for papillary thyroid cancer patients stratified by lymph node yield (LNY;
Discussion
The present study demonstrates the association between nodal factors and recurrence after thyroidectomy plus central compartment ND with/without lateral compartment ND for the treatment of PTC. All nodal factors, including the positive number of LNs, ratio, and extranodal extension, were significantly associated with nodal and any-site recurrence after thyroidectomy, as well as tumor size and multifocality. Among the nodal factors, LN ratio and extranodal extension remained the independent factors predictive of post-treatment recurrence. The study suggests that the LN ratio is an effective prognostic indicator. Therefore, the study may help to guide the management and prognostic prediction for PTC patients.
Nodal status is well recognized as an important factor predictive of disease-free and disease-specific survivals in patients with well-differentiated thyroid cancer (DTC) (20 –22). In a population-based study comprised of 29,255 DTC patients, the overall 5- and 10-year cumulative incidence of cancer-specific mortality were 1.9% and 3.0%, respectively, which increased up to 4.8% and 6.9% when associated with regional LN involvement and to 15.0% and 21.7% with distant LN involvement (20). The presence of clinical LN metastasis from PTC also increases the post-treatment recurrence to as high as 22% (range 10–42%) (7). In the present study, the 10-year cancer-specific and overall mortality rates were 0.5% and 1.6%, respectively. Moreover, the 10-year nodal and any-site recurrence rates were 4.6% and 6.0%, respectively. Clinical LN metastasis increases the 10-year cancer-specific mortality rate from 0.1% to 2% and the 10-year recurrence rate from 2.4% to 16.8%. Studies by both the authors and another group (7,20) have emphasized the prognostic value of nodal status in addition to age and tumor factors in relation to the recurrence and survival of PTC patients. Therefore, the present study focused on nodal factors, including LN yield, positive number, and ratio, and their association with post-treatment nodal and any-site recurrence in a large cohort of 2384 patients who underwent a thyroidectomy and central compartment LN dissection for PTC.
Among the nodal factors, the present study suggests a prognostic role of the LN ratio and extranodal extension for predicting any-site and nodal recurrences. In addition, previous studies have examined the prognostic implications of the LN yield and ratio in PTC patients. A LN ratio >0.3 was associated with a 3.4-fold higher risk of persistent or recurrent disease in 198 PTC patients who underwent a total thyroidectomy and ND (13). Moreover, a LN ratio ≥0.7 was associated with a significantly worse disease-free survival and higher disease recurrence (OR = 19.5 [CI 4.1–22.9]) in a study of 217 patients who underwent a total thyroidectomy plus ND (12). Similarly, the central and total LN ratios were also independent predictors of recurrence in a study of 253 PTC patients (23). Another study reported that a LN ratio ≥0.3 represented the strongest independent predictive factor for lateral LN recurrence in 760 patients who received a total thyroidectomy and prophylactic central LN dissection (24). A LN ratio (>0.44) in the central neck compartment was also an increased risk factor for locoregional recurrence in papillary microcarcinomas (25). Although there is growing evidence of the prognostic value of the LN ratio, further multicenter studies are required to elucidate the optimal cutoff value of the LN ratio, and to standardize the number and extent of dissected LNs.
There are several controversial reports on the clinical value of the LN yield and positive LNs in predicting recurrence and survival following a thyroidectomy with a concomitant ND. The LN yield was defined as the total number of harvested LNs and was not significantly associated with disease-free survival. However, an optimal LN yield was not determined (13). A recent retrospective study involving 125 PTC patients found that higher rates of recurrence were significantly associated with a lower LN yield in patients who underwent both central compartment ND and ipsilateral lateral ND (11). That study suggested the necessity of thorough, compartment-oriented, central and lateral compartment ND to minimize the risk of recurrence. In contrast, another study using the SEER database demonstrated that an increased LN yield was associated with poor survival in DTC patients, even in node-negative patients. This indicates that nodal understaging is inconsequential for the survival of DTC patients (14). Furthermore, an adequate LN yield remains undefined with a wide variation among surgeons. A recent study using the National Cancer Database (1998–2012) suggested that 6, 9, and 18 nodes need to be examined in PTC patients with T1b, T2, and T3 disease, respectively (9). The present study also demonstrates that a LN yield >18 is associated with increased rates of any-site and nodal recurrences, which were not independent factors.
Growing evidence indicates that the number of metastatic LNs is positively associated with the risk of recurrence. An increasing number of positive LNs is related to a significantly higher 10-year risk of recurrence: 3% for <5 LN metastases, 7% for 6–10 LN metastases, and 21% for >10 LN metastases (26). Similar findings were observed in the present study regarding the association between recurrence and the categories for the increased number of positive LNs. Another study showed that the presence of ≥10 metastatic LNs was significantly associated with a lower disease-free survival (27). Another Japanese group reported that the risk of recurrence was significantly higher in patients with more than five LN metastases (19%) compared to those with five or fewer LN metastases (8%) (28). Another study emphasized that the number of metastatic LNs in the central compartment is a significant predictor of recurrence (29). In accordance with the abovementioned findings, the recent management guidelines for differentiated thyroid cancer incorporate more than five positive LNs as a risk factor of structural recurrence (4,8). However, this criterion may need further refinement.
Extranodal extension is well recognized as an important prognostic factor for PTC; the more nodes present with extranodal extension, the greater the risk of recurrence. A previous study showed that an extranodal extension was indicative of a higher risk of recurrence: a risk of 1% in N1 stage patients without extranodal extension rose to 4% and 32% patients with one to three metastatic LNs and more than three metastatic LNs with extranodal extension, respectively (26). The presence of an extranodal extension is also less likely to exhibit a complete biochemical response, and these patients have an increased probability of tumor persistence following a thyroidectomy (30). Similar findings were also observed in the 1743 papillary microcarcinoma cases exhibiting a 14.5% recurrence rate for extranodal extension compared to a rate of 2.4% and 1.5% in patients with N0 and N1 diseases without extranodal extension, respectively (31). In the present study, nodal and any-site recurrence was significantly higher for patients with extranodal extension than those without extranodal extension: 10-year recurrence rates were 16.7% versus 2.5% for nodal recurrence and 20.0% versus 3.6% for any-site recurrence. Although several studies have reported that extranodal extension predicts a high risk of recurrence and impaired cancer-specific survival (26,30 –32), the present study confirms an association between extranodal extension and nodal recurrence in a large cohort study.
This study has several limitations, including a retrospective design and the inclusion of a high proportion of patients with small-sized tumors. Various pathological subtypes (e.g., follicular, tall-cell, and columnar-cell variants) were not considered in the analyses due to their extremely rare incidence. Most of our cases consisted of small-sized tumors ≤2 cm that were surgically treated without a clinical observational trial (1). In addition, most of the study patients (79.9%) underwent prophylactic central compartment LN dissection that is not routinely undertaken in most developed countries and is not recommended in the current management guidelines for PTC (4). Therefore, these may lead to a limited generalizability of the findings. Nonetheless, extrathyroidal extension (61.5%), LN metastasis (57.4%), and extranodal extension (15.5%) were frequently seen among the cases, despite the high prevalence of small tumors. In demonstrating the association of recurrence and nodal factors, this study may be clinically useful for the management and prediction of PTC patient prognosis.
In conclusion, this study further characterizes the risk factors of nodal and any-site recurrence after thyroidectomy and central compartment LN dissection with or without lateral compartment LN dissection. Among the nodal factors, the LN ratio was found to be an independent determinant predictive of nodal and any-site recurrence following a thyroidectomy for patients with PTC. Although the LN yield was higher among the patients with recurrences, it did not significantly affect nodal recurrence. While the number of metastatic LNs appeared to be a significant predictor of post-treatment recurrence, it exhibited borderline significance in the multivariate analysis. Therefore, these findings indicate that high-risk patients should receive close surveillance for potential recurrence after thyroidectomy.
Footnotes
Acknowledgments
This study was supported by a grant (no. 2015R1A2A1A15054540) from the Basic Science Research Program through the National Research Foundation of Korea, Ministry of Science, ICT, and Future Planning, and a grant (no. HI15C2920) from the Korean Health Technology R&D Project through the Korea Health Industry Development Institute, Ministry of Health & Welfare, Seoul, Republic of Korea (J.-L.R.).
Author Disclosure Statement
No competing financial interests exist.