
Abstract
Background:
The widespread use of neck sonography in recent years has led to a dramatic increase in the detection of thyroid cancer, accompanied by changes in the clinicopathologic features of the disease. However, small papillary carcinomas account for the bulk of this increase, while little is known about temporal changes in medullary thyroid carcinoma (MTC). The aim of this study was to evaluate trends in the presentation, treatment, and outcome of MTC.
Methods:
Patients treated for MTC at four medical centers in Israel were divided into three groups by year of diagnosis: 19811995 (period A), 1996–2005 (period B), and 2006–2016 (period C). Clinicopathologic and survival data were collected retrospectively from the medical files and compared between the groups.
Results:
The cohort included 182 patients (54.9% female) with a mean age of 49.2 ± 18.7 years: 43 (23.6%) diagnosed in period A, 54 (29.7%) in period B, and 85 (46.7%) in period C. No significant differences were found between the groups in primary tumor size (25.7 ± 18.9 mm, 26.6 ± 18 mm, and 23.7 ± 17.6 mm, respectively), proportion of micro-MTC (30.8%, 20.0%, and 25.3%, respectively), or TNM staging. Age at diagnosis significantly increased over time (38.7 ± 17.2 years, 51.7 ± 18.4 years, and 53.7 ± 17.7 years, respectively; p < 0.001), and the rate of familial MTC significantly decreased (41.9%, 14.8%, and 8.2%, respectively; p = 0.002). Although the implementation of cervical lymph node dissection increased (62.1%, 78.4%, and 85%, respectively; p = 0.01), detection of metastatic lymph nodes decreased from 88.9% in period A to 65.0% in periods B and C (p = 0.06). There was no difference between the groups in disease-specific survival or disease-free state at one year from diagnosis (37.5%, 43.1%, and 50%, respectively) and last follow-up (27%, 41.2%, and 48%, respectively). Similar findings on MTC presentation and outcomes were obtained when only patients with non-familial MTC were analyzed.
Conclusions:
Unlike differentiated thyroid cancer, most of the presenting features of MTC have not changed over time. The most significant temporal change is a decreased rate of familial MTC. Despite more extensive surgery and the use of new treatment modalities in recent years, significant improvement in disease-related outcomes were not found.
Introduction
T
Medullary thyroid carcinoma (MTC) is a rare but more aggressive malignancy than PTC, accounting for 1–5% of all cases of thyroid cancer (7). Most patients present with a thyroid nodule, similar to patients with DTC. However, unlike PTC, changes in the clinical features and prognosis of MTC over time remain unclear. Some authors have suggested that disease stage and patient survival have remained stable (8,9), whereas more recent studies have reported significant shifts in disease presentation and outcomes (10,11).
The aim of the present multicenter study was to evaluate and compare temporal trends in the clinicopathologic characteristics and outcomes of a large cohort of patients with MTC.
Methods
The study cohort included 182 consecutive patients diagnosed with MTC between 1981 and 2016 and followed at four tertiary medical centers in Israel. In all four institutions, patients with MTC are managed by a multidisciplinary team, including experienced ENT surgeons and experts in endocrinology and oncology, all with a specific interest in thyroid cancer. For the purposes of this study, patients were divided into three groups by year of diagnosis: 1981–1995 (period A), 1996–2005 (period B), and 2006–2016 (period C). Their medical files were reviewed for the following demographic, pathological, clinical, and outcome variables: sex and age at MTC diagnosis, mode of presentation, diagnosis of familial MTC, type of initial operation (hemi/total thyroidectomy with/without lymph node dissection [LND]), greatest dimension of the primary tumor, extension of the disease (intrathyroidal or extrathyroidal), number of lymph nodes removed at surgery, proportion of metastatic lymph nodes, presence and site(s) of distant metastasis, additional treatment modalities, duration of follow-up, disease state at last follow-up (complete remission or residual biochemical and/or structural disease), and survival. Patients were categorized as having familial MTC if a known pathogenic mutation was found in the RET proto-oncogene and/or at least one first-degree relative was diagnosed with MTC. The remaining patients were categorized as having probable sporadic MTC, as genetic analysis for RET mutations was not always performed.
MTC stage was classified according to the American Joint Committee of Cancer (AJCC) tumor-node-metastasis (TNM) system (12). Micro-MTC was defined as a primary tumor measuring ≤1.0 cm. The ratio of metastatic lymph nodes was calculated as the number of all metastatic lymph nodes identified divided by the number of all lymph nodes removed. Any patient in whom lymph nodes were detected at the initial surgery was considered to have undergone LND. Although this definition might incorporate patients with nodes that were removed unintentionally, it most reliably excludes patients who were not treated with LND.
Complete remission was defined as the absence of any biochemical or structural evidence of MTC. Residual disease was defined as structural in the presence of imaging findings compatible with loco-regional or distant metastatic lesions or as biochemical-only disease when elevated calcitonin level was detected without suspicious structural findings.
For patients who died during follow-up, the cause and time of death and the association of death to the presence of MTC were specified. Disease-specific survival (DSS) was determined from the date of diagnosis to the date of death from MTC. Overall survival (OS) was determined from date of diagnosis to the date of death from any cause. Because of the study design, the duration of follow-up was longest for patients diagnosed in the earlier periods. To account for this difference in the comparison of the groups for disease outcome, OS and DSS were also analyzed at five years after diagnosis. Similarly, the rate of disease-free state was compared in all three groups at both one year from diagnosis and at the last follow-up.
Statistical analysis
Categorical variables are presented as number and percentage, and continuous variables as mean and standard deviation (SD). The groups were compared for categorical variables with the chi-square test, and for continuous variables with Student's t-test or one-way analysis of variance, as appropriate. Fisher's exact test was used to analyze correlations of categorical variables when frequencies were too low for the performance of the chi-square test. The Kaplan–Meier method was used for univariate survival analysis, and the log-rank test was used to determine whether differences were statistically significant. The data were analyzed for the whole cohort and, additionally, after exclusion of patients with familial MTC.
All analyses were performed using IBM SPSS Statistics for Windows v24.0.1 (IBM Corp., Armonk, NY). A p-value of <0.05 was considered statistically significant. The study protocol was approved by the Institutional Ethics Board of all four medical centers.
Results
Patient demographics and clinical and pathological features
The cohort included 182 patients, of whom 100 (54.9%) were female. The mean age at diagnosis was 49.2 ± 18.7 years. MTC was diagnosed in 43 (23.6%) patients in 1981–1995 (period A), 54 (29.7%) patients in 1996–2005 (period B), and 85 (46.7%) patients in 2006–2016 (period C; Fig. 1).
Time of diagnosis in 182 patients with medullary thyroid carcinoma (MTC).
The baseline clinical, demographic, and pathological features of the patients at time of diagnosis are presented in Table 1. In periods B and C, the diagnosis of MTC in most cases was made after the detection of thyroid nodules or neck metastases. Notably, none of the patients was diagnosed on the basis of elevated calcitonin level, as patients with incidentally discovered thyroid nodules are not screened for serum calcitonin in Israel.
MTC, medullary thyroid carcinoma; SD, standard deviation; TNM, tumor-node-metastasis; NS, not significant.
The mean age at diagnosis increased significantly from 38.7 ± 17.2 years in period A to 51.7 ± 18.4 years in period B and 53.7 ± 17.7 years in period C (p < 0.001), with no change in sex distribution. Familial screening at any time during follow-up was performed in 103/182 (56.6%) patients: 25/43 (58.1%) patients in period A, 32/54 (59.3%) patients in period B, and 46/85 (54.1%) in period C patients. The rate of detected familial MTC decreased significantly from 41.9% in period A to 14.8% in period B and 8.2% in period C (p = 0.002).
There were no statistically significant differences between the groups in the pathological features of the primary tumor, including tumor size, proportion of micro-MTC, and rate of extrathyroidal extension. The TNM stage remained stable over periods A–C. Overall, of the 158 patients with sufficient data to define the TNM stage, 87 (55.1%) had N1disease at presentation and 33 (20.9%) had M1 disease. Most patients (101/158; 63.9%) had stage 3–4 disease: 68 diagnosed with stage 4, 25 diagnosed with stage 3, and eight in whom stages 3 and 4 could not be distinguished, usually because data were insufficient to determine the extent of locoregional lymph node metastases and to differentiate between N1a/N1b categories.
Baseline features were also analyzed in the 149 patients with apparently non-familial MTC (Table 2). As in the whole cohort, the single statistically significant temporal change was older age at diagnosis in periods B and C compared to period A (p = 0.016). Documented negative results of genetic screening for RET mutations was available in 70/149 (47%) patients: 7/25 (28%) patients diagnosed in period A, 24/46 (52.2%) diagnosed in period B, and 39/78 (50%) diagnosed in period C. In 7/70 (10%) patients, foci of MTC were found in both thyroid lobes.
Extent of surgery and treatment modalities
Data on the extent of surgery are shown in Table 3. In all three periods, >90% of the patients were treated with total thyroidectomy. The percentage of patients who underwent LND significantly increased from 62.1% in period A to 78.4% in period B and 85.0% in period C (p = 0.01). However, among the patients treated with LND, the detection rate of metastatic lymph nodes decreased from 88.9% in period A to 65.0% in periods B and C (p = 0.06).
Data on lymph node number and ratio in period A are not presented, as they were not specified in the pathological reports of most patients.
The indications for external beam radiation therapy (EBRT) were identical in all four medical centers and in all study periods. The indications for treatment with tyrosine kinase inhibitors (TKIs) were identical in all four institutions since the introduction of this therapy; these drugs were not available in the earlier years of the study. EBRT was used for loco-regional control in patients with incompletely resected MTC or at high risk of local recurrence. It was also used in patients with distant metastases to provide local control and improve quality of life. The proportion of patients who received EBRT at some point during surveillance was similar in periods A and B (23.2% and 24.1%, respectively) and significantly lower in period C (11%; p = 0.04). Twenty-three (12.6%) patients received treatment with TKIs at some point during follow-up, of whom 14 (60.9%) were diagnosed in period C compared to 4 in period A and 5 in period B. The indications for TKI treatment included advanced progressive and/or symptomatic disease.
Disease outcomes
Data on disease outcomes appear in Tables 4 and 5 and Figures 2 and 3. Overall, 23 patients died of the disease at a mean of 8 ± 7.3 years after diagnosis (median 4.5 years). They included 22 patients with stage 3–4 disease at presentation (18 stage 4, three stage 3, and one with insufficient data to differentiate between stage 3 and stage 4). The remaining patient underwent surgery in 1988, and the disease stage at presentation could not be retrospectively determined on the basis of the available data. However, the presence of distant metastases in the lungs and bones was documented in his file during follow-up.
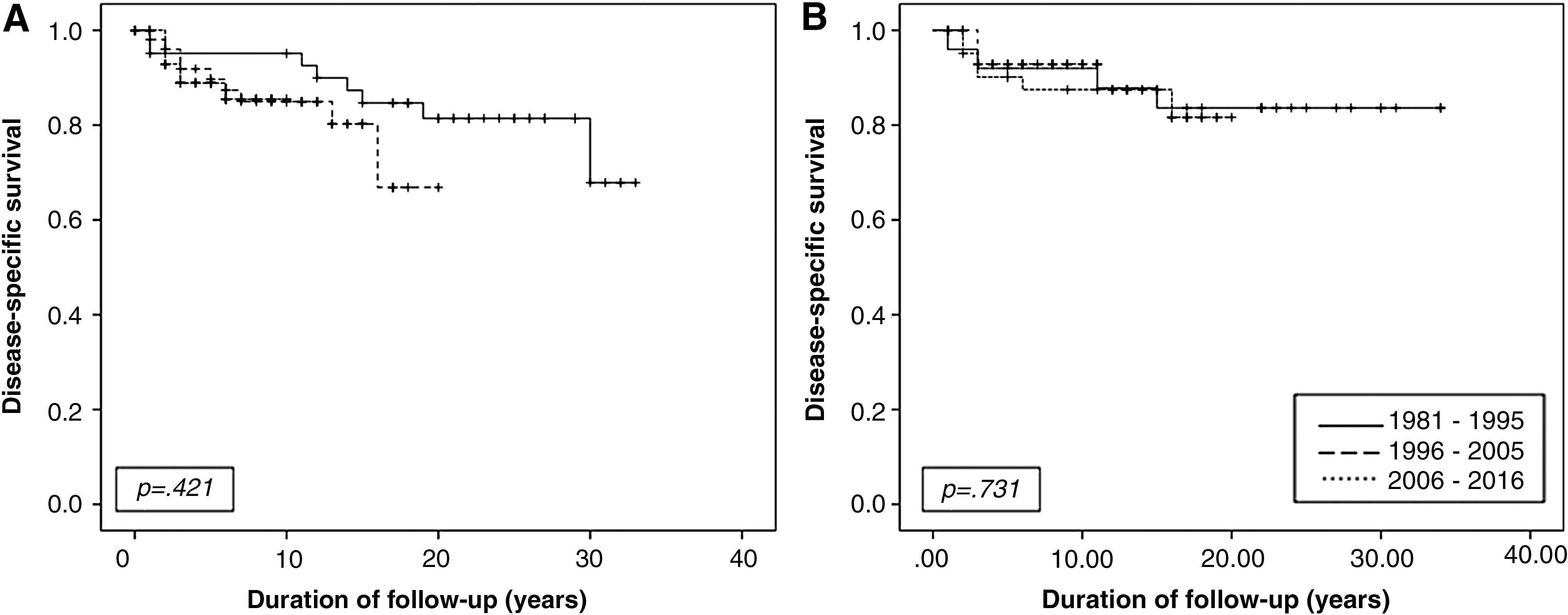
Kaplan–Meier analysis of disease-specific survival in the whole cohort of 182 patients with MTC (
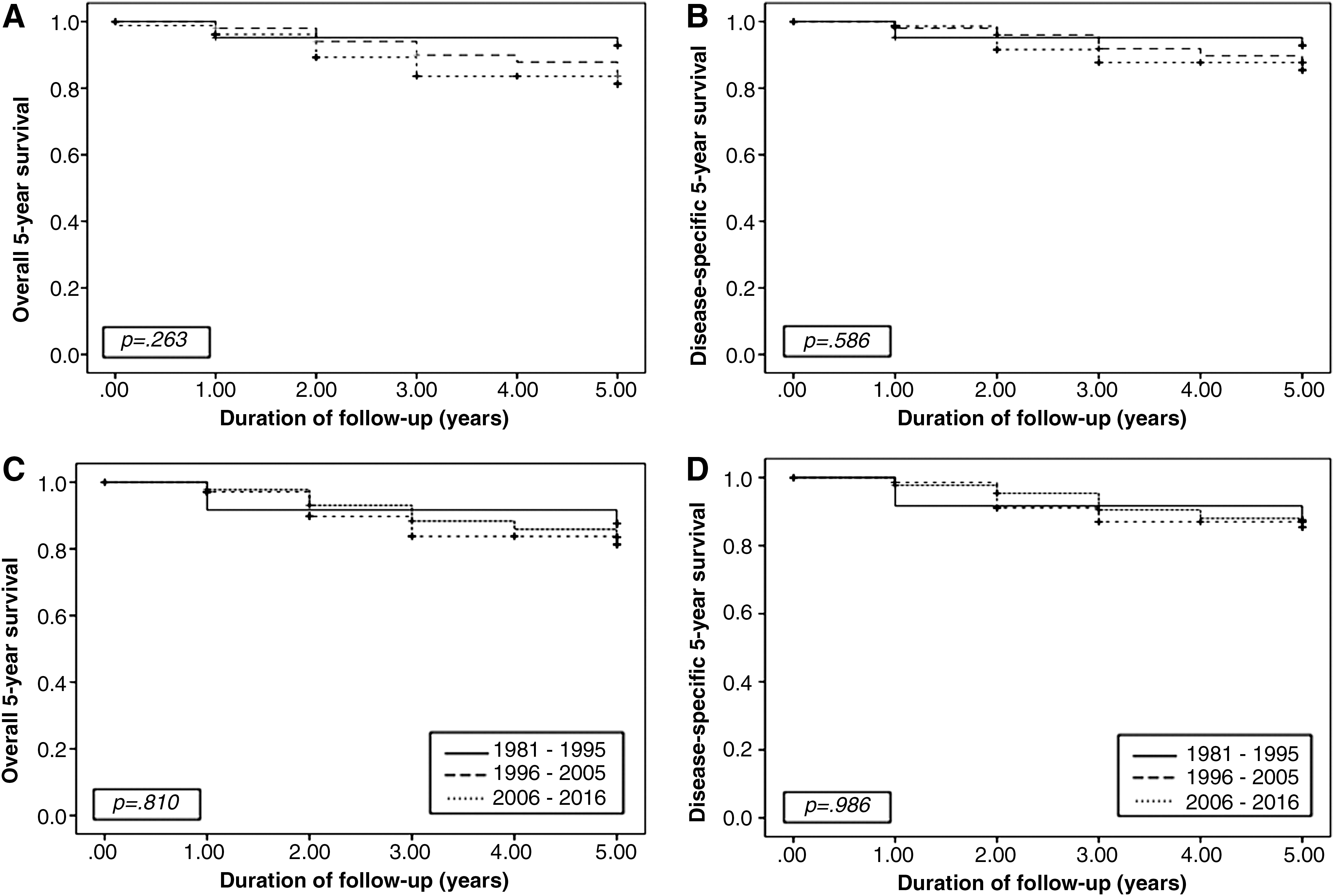
Kaplan–Meier analysis of five-year overall survival (
Persistent/recurrent disease was documented but not specified.
NED, no evidence of disease.
Persistence/recurrence is documented but not specified.
There were no statistically significant changes in DSS between the study periods. Additionally, no statistically significant changes were found for OS and DSS at five years from diagnosis in both the whole cohort (Table 4) and on separate analysis of patients with sporadic MTC (Table 5). Similarly, no differences were found in the rate of disease-free state at 1 year after diagnosis or at the last follow-up visit (Tables 4 and 5).
Figure 2A depicts the Kaplan–Meier curves for DSS in the whole cohort, and Figure 2B shows the patients with sporadic MTC during the study. Figure 3 depicts the Kaplan–Meier curves for OS and DSS at five years after diagnosis in the whole cohort (A and B, respectively) and in the patients with sporadic MTC (panel C and D, respectively).
Discussion
The present multicenter study evaluated the presentation, treatment, and outcome of patients who were diagnosed with MTC in the last 35 years in Israel. Comparison of the findings by time of diagnosis (1981–1995, 1996–2005, and 2006–2016) revealed that in recent years, an increasing proportion of cases of MTC were diagnosed after the detection of thyroid nodules or neck metastases. This is probably related to the rising use of neck ultrasonography. However, unlike PTC, most of the disease variables in the cohort remained stable over time. The most substantial temporal changes in the features of MTC at diagnosis were an increasing patient age and a significant decrease in the proportion of familial MTC.
Analysis of the pathological data of the patients included in this study revealed that most of the characteristics of MTC at presentation were similar over the three study periods. There was no difference in tumor size at diagnosis or in the proportion of micro-MTC. By contrast, a South Korean study of 109 patients with MTC diagnosed in 1996–2011 showed a gradual and significant chronological decrease in mean tumor size accompanied by an increase in the percentage of micro-MTC to up to 45% (10). The increase in the incidence of very small tumors may be associated with the South Korean practice of thyroid cancer screening followed by investigation and surgical intervention even for sub-centimeter lesions (3). In a single-institute study from the same country, the proportion of patients undergoing surgery for DTC measuring <1 cm in diameter rose from 14% in 1995 to 56% 10 years later (13). However, the lack of change in mean tumor size at diagnosis in the present study is in agreement with the results of Surveillance, Epidemiology, and End Results (SEER) program-based studies from 2005 (14) and 2017 (11). Additionally, although the more recent SEER study reported a significant increase in the proportion of micro-MTC over time (11), the 25.1% rate in the latest period of that study (2003–2012) is similar to the mean rate of 24.7% in all time periods in the present study.
The extent of disease at diagnosis also remained unchanged over the three periods evaluated in this study. This finding is in accordance with the SEER-based studies, which showed no significant trend toward an earlier stage of disease at diagnosis (11,14), even in the presence of a temporal rise in the proportion of micro-MTC (11). Furthermore, in another analysis of the SEER database including 310 patients with micro-MTC diagnosed in 1988–2007, the authors detected significant rates of poor prognostic features such as multifocality, extrathyroidal extension, lymph node metastases, and distant metastases (15). Thus, as opposed to PTC, while an increase in the incidence of micro-MTC suggests a trend toward earlier detection, it does not always equate to diagnosis at an earlier stage.
The percentage of familial MTC decreased steadily and significantly over time. This finding might partially explain the older patient age at MTC diagnosis in recent years. The discovery of the critical role of RET proto-oncogene mutations in hereditary MTC in 1993 facilitates genetic screening of the at-risk population (16). Thus, it might be assumed that in periods B and C of this study, patients with known familial MTC and a positive RET mutation underwent prophylactic thyroidectomy at a young age. However, other factors are probably involved as well, given that an increasing age at diagnosis was also found on separate analysis of the patients with sporadic MTC. An increase in age at diagnosis has also been demonstrated in previous studies (10,11).
The 2009 and 2015 guidelines of the American Thyroid Association for the management of MTC recommend total thyroidectomy with cervical lymph node dissection as the standard of care (17,18). Yet, Japanese investigators have proposed that given the very low frequency of bilateral disease in sporadic MTC, patients with negative family history and no germline RET mutations may be managed by hemithyroidectomy with neck dissection (19). In the present cohort, bilateral foci of MTC were detected in 10% of the patients with sporadic disease and negative genetic analysis. This finding, in accordance with previous reports of bilateral disease in up to 9% of patients with sporadic MTC (20 –22), demonstrates the advantage of total thyroidectomy as initial surgery in these circumstances.
The SEER-based studies reported a significant increase over time in the proportion of patients undergoing total thyroidectomy (11,14), from 43% in 1983–1992 to 81% in 2003–2012 (11). The corresponding increase in the rate of LND was from 53% to 68% (11). In the present study, total thyroidectomy was performed in >90% of the patients with MTC in all three periods, while the rate of cervical LND gradually and significantly increased from 62.1% in 1981–1995 to 85.0% in the last decade. However, the rate of patients with positive metastatic lymph nodes decreased from 88.9% in period A to 65.0% in periods B and C. This finding is compatible with previous reports (10,11), and it implies that the more extensive LND was done prophylactically and not for known cervical metastatic lesions.
The analysis of disease outcome in patients with MTC revealed no change over the three periods in rates of DSS or disease-free state at one year and at the last follow-up. Similar results were observed when the five-year OS and DSS were calculated. A possible explanation is the similarity in the clinicopathologic characteristics of the patients at presentation in all three periods. These results are in concordance with some previous studies (8,14) but disagree with two more recent studies that reported improved outcomes over time in MTC (10,11). Given the association of tumor recurrence with larger tumor size and more advanced nodal disease, Kwon et al. (10) attributed their finding of a higher disease-free survival rate in recent years to earlier diagnosis of the disease. However, they did not provide data on OS or DSS. The latest SEER-based study is the only one to demonstrate a significant improvement in DSS over time (11), probably because the large sample size afforded sufficient power to detect small but significant differences in disease outcomes. The improvement was noted in all patients with MTC, and it was greatest in those with regional or distant metastases (11). The authors suggested that the improved outcome over time in patients with regional disease may be explained by the use of more extensive neck surgery and, in patients with distant metastatic disease, by the introduction of novel systemic agents for this indication (23 –25). Targeted therapy with TKIs, including cabozantinib and vandetanib, has been found to improve progression-free survival in patients with MTC (24,25). In the present cohort, only 23 patients were treated with TKIs, mostly in period C, as expected. They were not analyzed separately because of their small number and the unequal distribution and circumstances of TKI treatment in the three periods. The proportion of patients receiving ERBT was significantly lower in period C than in the preceding periods. However, as ERBT may be administered at any point during the course of patient surveillance, this finding might reflect the inherently shorter follow-up of the group C patients.
Strengths and limitations
An important strength of this study is the rather large number of patients with MTC, although the cohort is probably still underpowered to detect small but clinically important differences. It is reasonable to assume that the differences observed in some of the variables would have reached statistical significance had a larger cohort been attainable. Another major advantage of this study is the availability of detailed demographic, clinical, and pathological data at presentation and throughout the surveillance years. In contrast to the much larger SEER-based study, this study was able to identify cases of hereditary MTC, detect disease states, and include different treatment modalities applied over the duration. This made it possible to specifically evaluate temporal trends in disease presentation and outcomes in patients with sporadic MTC. Using the recorded data, this study was also able to adjust pathological variables in the earlier study years to the recent AJCC TNM staging system for MTC in most patients.
This study is limited by the retrospective design, which has the inherent disadvantages of missing data and possible reporting bias. Additionally, being non-population based, the study is not appropriate for analyzing changes in MTC incidence. Finally, genetic screening for the RET mutation was only performed in some of the patients with presumed sporadic MTC. Recent studies have reported that 1–7% of the patients with apparently sporadic MTC may have hereditary disease (26,27). Therefore, the rate of familial MTC may have been underestimated in the cohort. This could also have hampered the accuracy of the data analysis of patients with apparently sporadic disease.
In conclusion, this study shows that the size and the pathological stage of MTC at presentation have not significantly changed in recent years. The extent of initial surgery has increased, as reflected in the higher rate of patients undergoing cervical lymph node dissection, probably prophylactically. At the same time, a statistically significant chronological improvement in disease outcomes was not detected. Although the rate of familial MTC has significantly decreased over time, the study still found no change in most of the presenting features of the disease and no change in outcomes on separate analysis of the patients with non-familial MTC. Further studies are needed to assess the short- and long-term impact of the new medical treatments on the outcome of MTC.
Footnotes
Author Disclosure Statement
No competing financial interests exist.