
Abstract
Background:
Noninvasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) is an indolent thyroid tumor previously known as noninvasive subtype of encapsulated follicular variant of papillary thyroid carcinoma (EFVPTC). The absence of BRAFV600E mutations has been considered characteristic of NIFTPs. However, a recent study from Korea found that 28.6% of NIFTPs harbored a BRAF mutation. This study evaluated BRAF and RAS mutations in NIFTPs and invasive subtype of EFVPTCs.
Methods:
This study enrolled 32 patients with NIFTP and 48 with invasive EFVPTC. BRAF, NRAS, HRAS, and KRAS mutations were evaluated by direct sequencing using DNA from fresh-frozen tissues and formalin-fixed, paraffin-embedded tissue samples.
Results:
The primary tumor size of NIFTP was smaller than that of invasive EFVPTC (median 2.8 cm vs. 3.2 cm; p = 0.03). Cervical lymph node metastases were found in only four (8%) patients with invasive EFVPTC. There was no BRAF mutation in NIFTPs, whereas invasive EFVPTCs had three (6%) BRAFV600E mutations and one (2%) BRAFK601E mutation. RAS mutations were detected in 15 (47%) NIFTPs and 22 (46%) invasive EFVPTCs. NRAS mutations in codon 61 were the most common mutations in NIFTPs (34%) and invasive EFVPTCs (27%). There was no significant difference in the frequency of RAS mutations between the two groups.
Conclusions:
There was no BRAF mutation in any of the NIFTPs. RAS mutations, particularly mutations in codon 61 of NRAS, were the most common mutations in both NIFTPs and invasive EFVPTCs. The presence of a RAS mutation is not helpful for preoperative differentiation between NIFTPs and invasive EFVPTCs.
Introduction
T
Molecular testing for genetic mutations has been shown to enhance the diagnostic accuracy of thyroid fine-needle aspiration cytology (FNAC), particularly in cases with an indeterminate category cytology (9). The most common genetic alterations in thyroid cancer are BRAF and RAS point mutations, and these mutations are mutually exclusive (9,10). Several studies have reported that EFVPTC has a high frequency of RAS mutations (30–40%), and that most RAS mutations in PTCs were associated with EFVPTC (3,6,11 –13). The absence of the BRAFV600E mutation is regarded as one of characteristic features of NIFTPs (6,14), whereas 0–30% of invasive EFVPTC harbor BRAFV600E mutations (15 –17). However, a recent study from Korea reported that 28.6% of NIFTPs harbored BRAF mutations (18). It was proposed in that study that the differences in the prevalence of BRAF mutations in NIFTPs may be attributed to ethnic differences. However, there has been no further evidence to support this.
This study evaluated BRAF and RAS mutations in NIFTPs and invasive EFVPTCs in Koreans. The study also compared the frequency of these mutations as potential diagnostic markers to distinguish these two entities.
Materials and Methods
Patients and sample collection
This study enrolled 32 patients with NIFTP and 48 patients with invasive EFVPTC who underwent initial thyroid surgery between 2013 and 2016 at the Asan Medical Center (Seoul, Korea). Genomic DNA from fresh-frozen tissues (n = 62) and formalin-fixed, paraffin-embedded (FFPE) samples (n = 18) were used for direct sequencing. For mutational analysis, all tissue specimens were reviewed by an experienced pathologist (D.E.S.). The pathologist selected adequate tissue blocks for the isolation of DNA from EFVPTC tissues. In all, 62 fresh-frozen EFVPTC tissues from surgically removed thyroid samples were collected at the Asan Bio-Resource Center and used to isolate genomic DNA following Institutional Review Board approval (2013-0539). The clinicopathologic features of EFVPTCs were reviewed after approval by the Institutional Review Board of Asan Medical Center (2016-0635).
DNA extraction methods
Genomic DNA was isolated from 10 mg of fresh-frozen tissue using the DNeasy Blood & Tissue Kit (Qiagen, Hilden, Germany) according to the manufacturer's instructions, as previously described (19). For FFPE samples, genomic DNA was extracted from two and eight 10-μm-thick FFPE tissue sections containing a representative portion of each archival tissue block using the QIAamp DNA Mini Kit (Qiagen) (20).
Mutational analysis of the BRAF and RAS genes
Genomic DNA from fresh-frozen tissues and FFPE samples was used for polymerase chain reaction (PCR) amplification and direct sequencing to evaluate the presence of BRAF and RAS mutations. Exon 15 on the BRAF gene and exons 2 and 3 of the NRAS, HRAS, and KRAS genes were amplified using PCR, with appropriate primers. The status of the BRAF and RAS mutations was analyzed, as reported previously (20,21). Briefly, the amplification protocol consisted of initial denaturation at 95°C for 15 min, followed by 45 cycles of denaturation at 95°C for 30 s, annealing of the primer to the template at 55–65°C for 30 s, primer extension at 72°C for 30 s, and a final extension at 72°C for 5 min. Then, the PCR was cooled to 4°C. The amplified PCR was purified using a gel extraction kit (Qiagen, Valencia, CA) and submitted to direct sequencing. The DNA sequences were read using a DNA analyzer (Bioedit v7.2.0; Ibis Biosciences, Carlsbad, CA). Each DNA sample was analyzed at least twice to confirm the status of the BRAF and RAS mutations.
Pathological evaluation and definition
All thyroid specimens were reviewed and diagnosed by an experienced pathologist (D.E.S). The preoperative FNAC results were categorized using the Bethesda System (22). Surgical specimens were reviewed and diagnosed based on the World Health Organization classification criteria (23). For effective gross examination of encapsulated thyroid nodules, a modified form of parallel transverse sectioning was used (4). Additional vertical sectioning of the tumor capsule was performed to examine the entire tumor capsule and adjacent thyroid parenchyma interface completely at both ends of the encapsulated thyroid nodules. The entire tumor capsule and the majority of the tumor parenchyma were reviewed microscopically. When the tumor size was >4 cm, about 80% of the parenchyma was examined microscopically.
EFVPTCs were categorized into two groups. Diagnostic criteria for the noninvasive subtype of EFVPTCs (i.e., NIFTPs) included a microscopic follicular growth pattern, complete or partial encapsulation with clear demarcation from adjacent normal thyroid parenchyma, and the presence of nuclear features of papillary thyroid cancer similar to the consensus inclusion criteria by Nikiforov et al. (1). These tumors showed no capsular or vascular invasion (1). The invasive subtype of EFVPTCs was defined by being fully encapsulated/well circumscribed in combination with any capsular or vascular invasion in the tumor capsule (1,8,24). Criteria for capsular invasion included tumor buds penetrating the outer contour of the capsule or the separate satellite tumor nest with identical tumor cells outside the capsule. Criteria for vascular invasion included a polypoid tumor nest covered by endothelium, attached to the walls of blood vessels located within or outside the capsule, rarely associated with a thrombus, and excluded free floating tumor nests in vascular lumens. Strict criteria for the percentage of classic papillae were applied to the cases of EFVPTCs, and a diagnostic cutoff of 0% papillae was used in this study. The original diagnosis of NIFTPs was noninvasive subtype of EFVPTCs. However, two patients with noninvasive EFVPTCs were reclassified as invasive subtype of EFVPTC after pathological review.
The main follicular growth pattern of tumor cells in EFVPTCs were subclassified into five types: microfollicular, macrofollicular, mixed micro- and macrofollicular, minor solid (<50%), and minor solid with clear cytoplasm (<50%). The status of the tumor capsule was separately classified into two types: totally encapsulated and partially encapsulated/well demarcated.
Statistical analyses
All statistical analyses were conducted using R v.3.1.0 (R Foundation for Statistical Computing, Vienna, Austria;
Results
Baseline characteristics of study subjects
The clinicopathologic characteristics of the 32 patients with NIFTP and 48 patients with invasive EFVPTC are presented in Table 1. The median age of the patients was 51.7 years (IQR 40.8–61.2 years), and 60 (75%) patients were female. The median primary tumor size was 3.0 cm (IQR 2.4–4.5 cm). The median primary tumor size of NIFTPs was significantly smaller than that of invasive EFVPTCs (2.8 vs. 3.2 cm; p = 0.03). Cervical lymph node (LN) metastases were found only in four (8%) patients with invasive EFVPTCs, and these were confined to the level VI area. Minimal extrathyroidal extension (ETE) and lymphovascular invasion (LVI) were only present in three (6%) and five (10%) patients with invasive EFVPTCs, respectively. No patient had distant metastasis at the time of initial surgery. A total of 51 (64%) patients underwent total thyroidectomy, and 26 (33%) received radioactive iodine (RAI) remnant ablation therapy based on the tumor size, ETE, or cervical LN metastases. There were no significant differences in age, sex, ETE, LVI, initial surgical extent, or RAI therapy between the two groups. There was no recurrent disease in patients with NIFTP and invasive EFVPTC during a median of 29.8 months (IQR 24.5–36.1 months) of follow-up.
Values are expressed as median (interquartile range) or number (%). Statistically significant values are shown in bold.
Minor solid defined as the proportion of solid areas occupying the tumor <50%.
NIFTP, noninvasive follicular thyroid neoplasm with papillary-like nuclear features; EFVPTC, encapsulated follicular variant of papillary thyroid carcinoma; I-EFVPTC, invasive subtype of EFVPTC; LN, lymph node; RAI, radioactive iodine; AUS, atypia of undetermined significance; FN, follicular neoplasm; SFN, suspicious for follicular neoplasm.
On the basis of the preoperative FNAC results, atypia of undetermined significance (n = 49; 61%) was the most common preoperative FNAC diagnosis. There were no significant differences in preoperative FNAC results between the two groups. On pathological examination, the most common growth pattern of tumor cells was mixed micro- and macrofollicular growth in both NIFTPs (50%) and invasive EFVPTCs (48%). Macrofollicular growth involving >50% of tumor cells was identified in six (19%) patients with NIFTPs and five (10%) patients with invasive EFVPTCs. Minor solid or cytoplasmic clear features (<50% of tumor cells) were identified in only three (6%) patients with invasive EFVPTCs (from 30% to 45%). Encapsulation was predominant in both NIFTPs (72%) and invasive EFVPTCs (69%). There were no significant differences in growth pattern of tumor cells or the tumor capsule (aside from invasion) between the two groups.
Prevalence of BRAF and RAS mutations in NIFTPs and invasive EFVPTCs
The frequency of BRAF and RAS mutations were compared in NIFTPs and the invasive subtype of EFVPTC (Table 2). There were four (8%) BRAF mutations in invasive EFVPTCs, including three BRAFV600E mutations and one BRAFK601E mutation. No BRAF mutation was found in NIFTPs. There were no significant differences in the frequency of BRAF mutations between the two groups (p = 0.15).
RAS mutations were detected in 15 (47%) NIFTPs and 22 (46%) invasive EFVPTCs. NRAS mutations in codon 61 were the most common mutation in both NIFTPs (34%) and invasive EFVPTCs (27%). HRAS codon 61, HRAS codon 12/13, and KRAS codon 61 mutations were detected in two (6%), one (3%), and one (3%) NIFTPs, respectively. HRAS codon 61 and KRAS codon 61 mutations were detected in eight (17%), and one (2%) invasive EFVPTCs, respectively. There were no NRAS codon 12/13 or KRAS codon 12/13 mutations in the two groups. There were no significant differences in the frequency of RAS mutations or NRAS codon 61 mutations between the two groups (p = 0.99 and p = 0.62, respectively).
Clinicopathologic features of patients with invasive EFVPTC harboring BRAF mutations
The clinicopathologic features of the four patients with BRAF mutations are listed in Supplementary Table S1. Two invasive EFVPTCs harboring BRAFV600E had microscopically minor solid growth and cytoplasmic clear features (35% and 45%, respectively), as shown in Figure 1. The other invasive EFVPTC harboring a BRAFV600E mutation had a microscopically mixed micro- and macrofollicular growth pattern. There was no cervical LN metastasis and no vascular invasion in these patients.
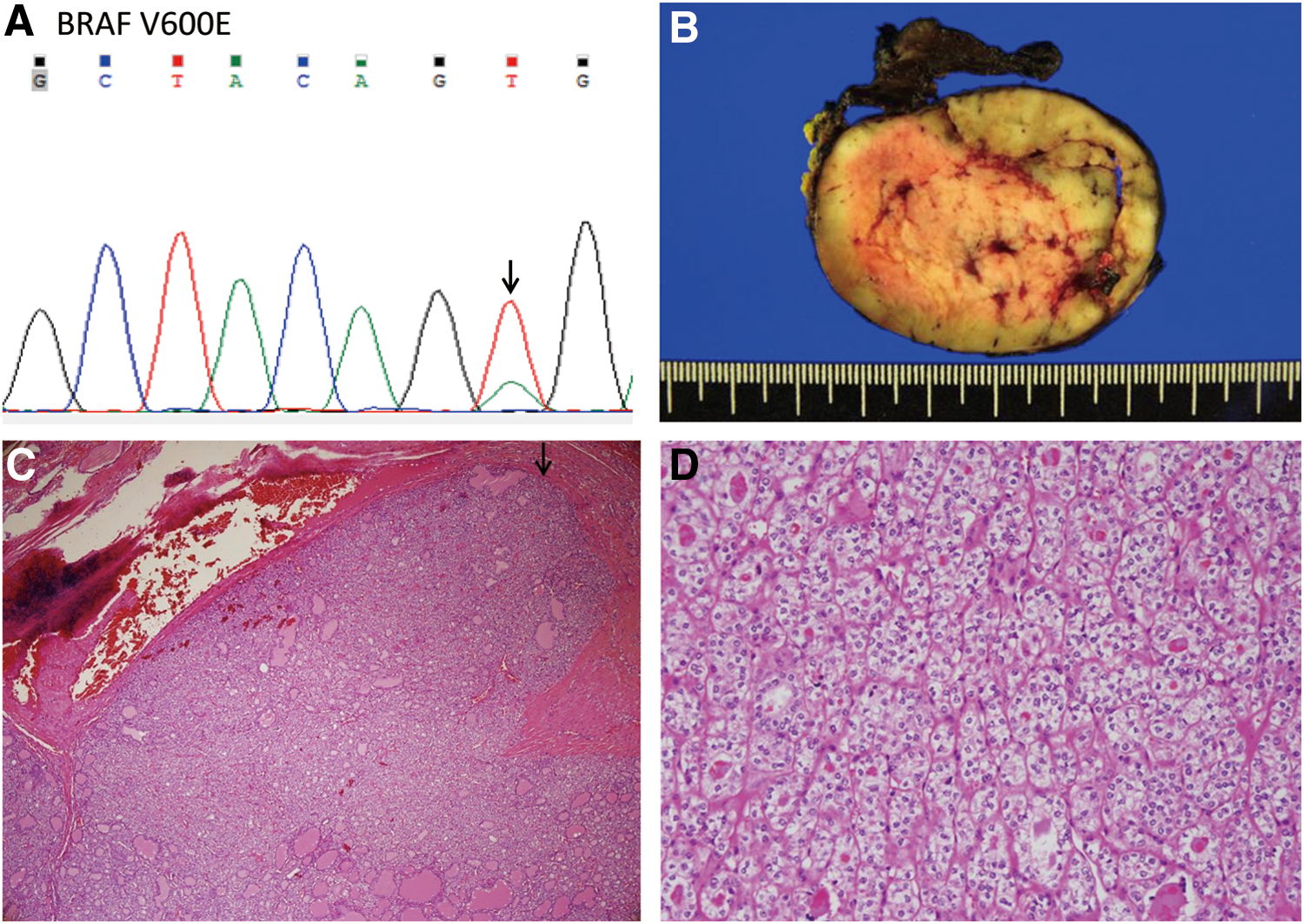
A case of invasive encapsulated follicular variant of papillary thyroid carcinoma (EFVPTC) harboring a BRAFV600E
mutation. (
BRAFV600E was detected in one invasive EFVPTC with minor solid growth and cytoplasmic clear features by direct sequencing of the postoperative FFPE specimen (Fig. 1A). The patient was a 21-year-old female and underwent right hemithyroidectomy with prophylactic central compartment node dissection. A well-demarcated huge encapsulated mass (7.0 cm in the greatest dimension) replaced nearly the entire right lobe of the thyroid (Fig. 1B). Microscopic examination revealed two foci of capsular invasion (Fig. 1C, arrow) without vascular invasion. Tumor cells with minor solid growth and cytoplasmic clear features (about 45%) showed mild nuclear atypia, including nuclear enlargement, nuclear overlapping, oval nuclear shape, pale chromatin, and nuclear grooves (Fig. 1D).
A BRAFK601E mutation was detected in one invasive EFVPTC by direct sequencing of the postoperative fresh-frozen specimen (Fig. 2A). The patient was a 72-year-old female who underwent left hemithyroidectomy. A well-demarcated partially encapsulated mass (2.2 cm in the greatest dimension) was identified in the left lower pole of the thyroid (Fig. 2B). Microscopic examination revealed two foci of capsular invasion (Fig. 2C, arrow) without vascular invasion. Tumor cells with microfollicular growth pattern showed subtle mild nuclear atypia, including nuclear enlargement, nuclear overlapping, oval nuclear shape, and occasional nuclear grooves (Fig. 2D).
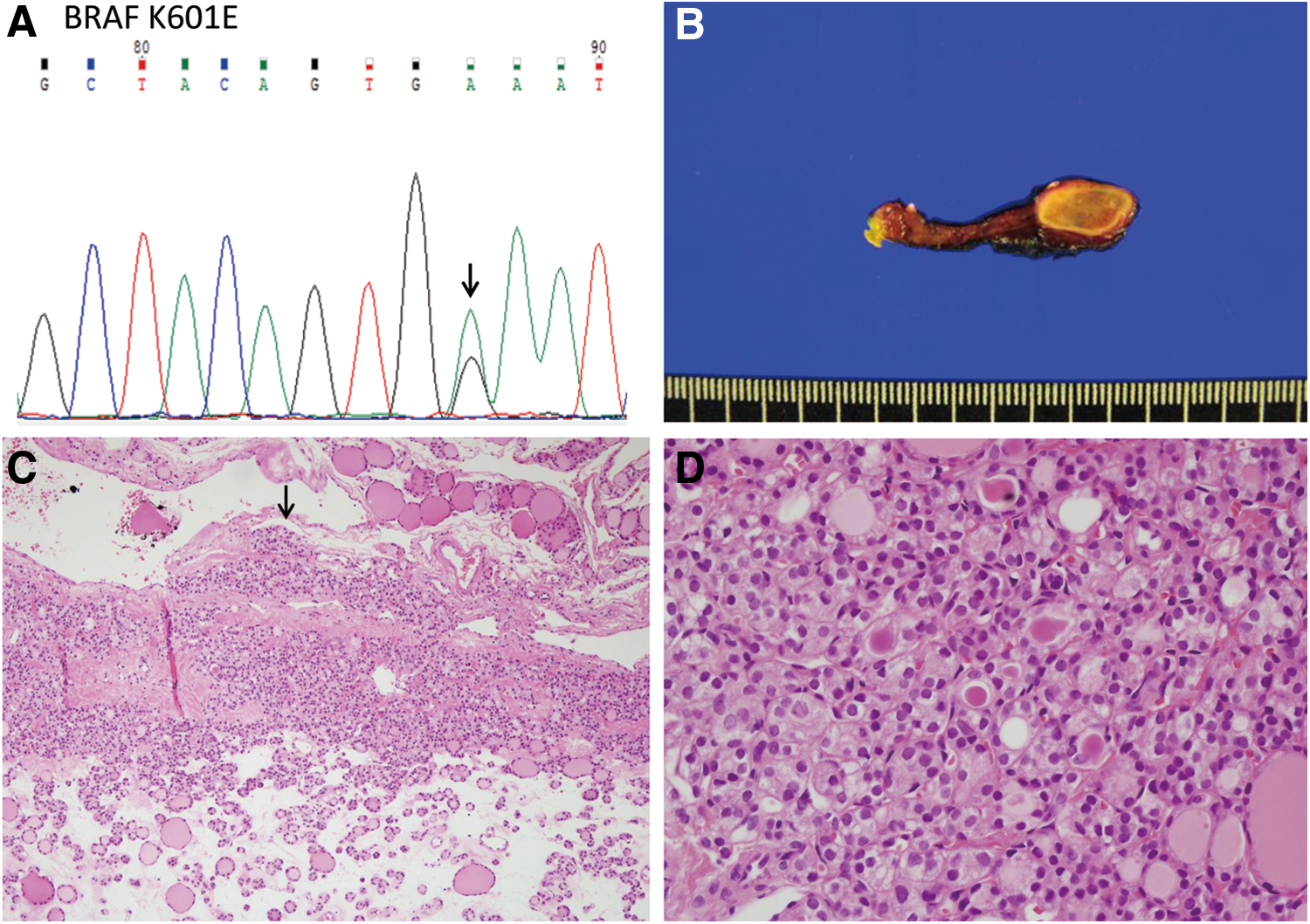
A case of invasive EFVPTC harboring a BRAFK601E
mutation. (
Discussion
This study evaluated BRAF and RAS mutations in NIFTPs and invasive EFVPTCs. There was no BRAF mutation in the series of NIFTPs, which is in contrast to a previous study from Korea. BRAF mutations were detected in only 8% of invasive EFVPTCs, and these were associated with solid growth and cytoplasmic clear features or microfollicular growth pattern of the cancer cells. RAS mutations were the most common mutations in both NIFTPs (47%) and invasive EFVPTCs (46%). There was no significant difference in the frequency of RAS mutations between the two groups.
For the pathological diagnosis of EFVPTC, strict criteria were used for the cutoff for 0% classic papillae and a modified parallel transverse sectioning method. EFVPTC has been a controversial diagnosis in thyroid gland pathology because tumors with a follicular growth pattern can show focal or subtle nuclear features of PTC (1). Recently, an international multidisciplinary study suggested that noninvasive EFVPTC should be renamed NIFTP, with defined diagnostic criteria as follows: (i) encapsulation or clear demarcation; (ii) follicular growth pattern with <1% papillae, no psammoma bodies, and <30% solid/trabecular/insular growth pattern; (iii) a nuclear score of 2–3, (iv) no vascular or capsular invasion; (v) no tumor necrosis, and (vi) no high mitotic activity (1). A recent study demonstrated that the arbitrary cutoff of 1% papillae has resulted in the misclassification of noninvasive classic PTCs with predominant follicular architecture as NIFTPs (17). In this study, strict histopathologic criteria were used for the accurate classification of NIFTPs and invasive EFVPTC.
In the present study, there was no BRAF mutation in NIFTPs, and BRAF mutations were only detected in invasive EFVPTCs. These findings are consistent with the results of previous studies that reported that the absence of BRAFV600E mutations is a characteristic feature of NIFTPs (1,6,14), while 0–30% of invasive EFVPTCs harbor a BRAFV600E mutation (15 –17). However, a recent study from Korea suggested that 28.6% of NIFTPs harbor BRAF mutations (18). The authors of that study suggested that the differences in the prevalence of BRAF mutations in NIFTPs could be explained by ethnic differences. However, given the results of the present study, there is no evidence that this difference is indeed related to ethnicity. Rather, the difference is likely due to the uncertainty of the diagnostic criteria of NIFTPs in that study (18). Another study from Korea indicated that more rigid histologic criteria (no papillary structure) could reclassify all BRAFV600E harboring EFVPTCs as classic PTC with predominant follicular growth (17). NIFTPs are not expected to have the molecular alterations associated with classic PTC, such as the BRAFV600E mutation, when defined by strict histopathologic criteria (1). Therefore, applying stricter diagnostic criteria for NIFTPs, including genetic characterization of the thyroid tumors, is important in clinical practice.
In the present study, two (67%) of three tumors that harbored a BRAFV600E mutation demonstrated microscopically minor solid growth and cytoplasmic clear features (35% and 45%, respectively). There are numerous histopathologic variants of PTC, and each variant of PTC has a combination of specific growth patterns, cell types, and stromal changes (25). A major problem in classifying PTC into various subtypes is that the defining criteria used are not rigorously defined. For this reason, different pathologists may not agree on certain subtype classifications (25). The solid variant of PTC is a rare subtype, and it is associated with a less favorable prognosis than EFVPTC (26). Currently, this variant is defined as a tumor with >50% of the tumor cells demonstrating a solid growth pattern, with solid nests resembling filled follicles surrounded by a thin rim of capillary-rich connective tissue on histology (26,27). If the cutoff for the solid variant of PTC had been set at 30% rather than at 50%, the two BRAFV600E -harboring tumors would have been classified as solid variant PTC rather than invasive EFVPTC.
One invasive EFVPTC in this study had a BRAFK601E mutation. The BRAFK601E mutation results from a single nucleotide substitution of adenine to guanine at position 1801 in the cDNA (c.1801A>C), which leads to a lysine to glutamate substitution at residue 601 (p.K601E) (28). The BRAFK601E mutation is associated with FVPTC rather than with classic PTC, and it has a prevalence of about 9% (28 –30). Among FVPTCs, BRAFK601E -mutated FVPTCs have less aggressive pathologic features than those harboring BRAFV600E mutations (28). Further studies are needed to determine whether the presence of a BRAFK601E mutation could be helpful in distinguishing NIFTPs and invasive EFVPTCs.
In conclusion, there was no BRAF mutation in the NIFTPs from Korea included in this study. RAS mutations, particularly mutations in codon 61 of NRAS, were the most common mutations in both NIFTPs and invasive EFVPTCs. The presence of RAS mutations is not helpful for the preoperative differentiation between NIFTPs and invasive EFVPTCs. Further comprehensive studies about genetic alterations are needed to identify the biomarkers that may be able to distinguish NIFTPs from invasive EFVPTCs preoperatively.
Footnotes
Acknowledgments
This study was supported by a grant (no. 2017-582) from the Asan Institute for Life Sciences, Asan Medical Center, Seoul, Korea. The biospecimens and data used in this study were provided by Asan Bio-Resource Center, Korea Biobank Network (2013-3(62)).
Author Disclosure Statement
No authors have any conflicts of interest in relation to this manuscript.